Thomas Brown Rudd Health Center - Hamilton College
Thomas Brown Rudd Health Center - Hamilton College
Thomas Brown Rudd Health Center - Hamilton College

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
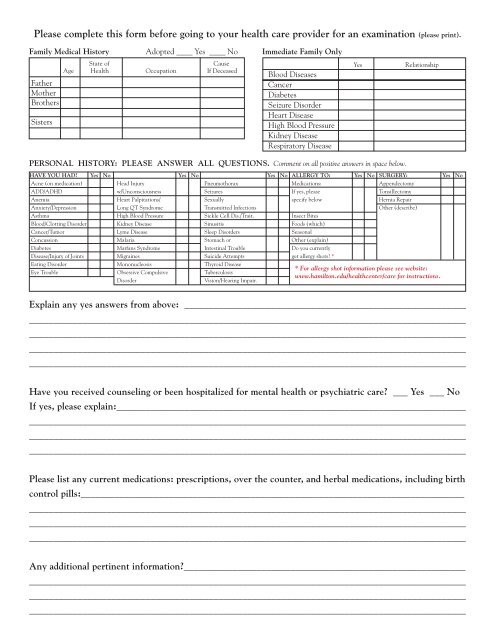
Please complete this form before going to your health care provider for an examination (please print).<br />
Family Medical History Adopted ____ Yes ____ No Immediate Family Only<br />
Father<br />
Mother<br />
Brothers<br />
Sisters<br />
State of<br />
Cause<br />
Age <strong>Health</strong> Occupation If Deceased<br />
Blood Diseases<br />
Cancer<br />
Diabetes<br />
Seizure Disorder<br />
Heart Disease<br />
High Blood Pressure<br />
Kidney Disease<br />
Respiratory Disease<br />
Yes<br />
Relationship<br />
PERSONAL HISTORY: PLEASE ANSWER ALL QUESTIONS. Comment on all positive answers in space below.<br />
HAVE YOU HAD Yes No Yes No Yes No ALLERGY TO: Yes No SURGERY: Yes No<br />
Acne (on medication) Head Injury Pneumothorax Medications: Appendectomy<br />
ADD/ADHD w/Unconsciousness Seizures If yes, please Tonsillectomy<br />
Anemia Heart Palpitations/ Sexually specify below Hernia Repair<br />
Anxiety/Depression Long QT Syndrome Transmitted Infections Other (describe)<br />
Asthma High Blood Pressure Sickle Cell Dis./Trait. Insect Bites<br />
Blood/Clotting Disorder Kidney Disease Sinusitis Foods (which)<br />
Cancer/Tumor Lyme Disease Sleep Disorders Seasonal<br />
Concussion Malaria Stomach or Other (explain)<br />
Diabetes Marfans Syndrome Intestinal Trouble Do you currently<br />
Disease/Injury of Joints Migraines Suicide Attempts get allergy shots *<br />
Eating Disorder Mononucleosis Thyroid Disease<br />
Eye Trouble Obsessive Compulsive Tuberculosis<br />
Disorder<br />
Vision/Hearing Impair.<br />
* For allergy shot information please see website:<br />
www.hamilton.edu/healthcenter/care for instructions.<br />
Explain any yes answers from above: __________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
Have you received counseling or been hospitalized for mental health or psychiatric care ___ Yes ___ No<br />
If yes, please explain:________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
Please list any current medications: prescriptions, over the counter, and herbal medications, including birth<br />
control pills:_______________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
Any additional pertinent information__________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________