Thomas Brown Rudd Health Center - Hamilton College
Thomas Brown Rudd Health Center - Hamilton College
Thomas Brown Rudd Health Center - Hamilton College

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
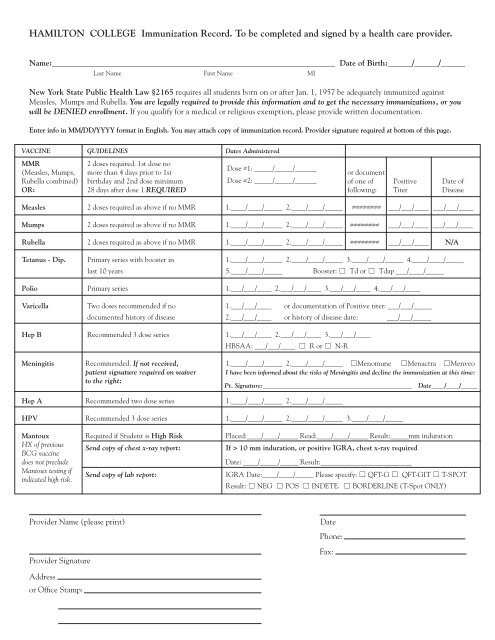
HAMILTON COLLEGE Immunization Record. To be completed and signed by a health care provider.<br />
Name:______________________________________________________________________ Date of Birth:______/______/______<br />
Last Name First Name MI<br />
New York State Public <strong>Health</strong> Law §2165 requires all students born on or after Jan. 1, 1957 be adequately immunized against<br />
Measles, Mumps and Rubella. You are legally required to provide this information and to get the necessary immunizations, or you<br />
will be DENIED enrollment. If you qualify for a medical or religious exemption, please provide written documentation.<br />
Enter info in MM/DD/YYYY format in English. You may attach copy of immunization record. Provider signature required at bottom of this page.<br />
VACCINE GUIDELINES Dates Administered<br />
MMR<br />
2 doses required. 1st dose no<br />
Dose #1: _____/_____/______<br />
(Measles, Mumps, more than 4 days prior to 1st or document<br />
Rubella combined) birthday and 2nd dose minimum Dose #2: _____/_____/______ of one of Positive Date of<br />
OR: 28 days after dose 1 REQUIRED following: Titer Disease<br />
Measles 2 doses required as above if no MMR 1.____/____/_____ 2.____/____/_____ ######## ___/___/____ ___/___/____<br />
Mumps 2 doses required as above if no MMR 1.____/____/_____ 2.____/____/_____ ######## ___/___/____ ___/___/____<br />
Rubella 2 doses required as above if no MMR 1.____/____/_____ 2.____/____/_____ ######## ___/___/____ N/A<br />
Tetanus - Dip. Primary series with booster in 1.____/____/_____ 2.____/____/_____ 3.____/____/_____ 4.____/____/_____<br />
last 10 years 5.____/____/_____ Booster: ☐ Td or ☐ Tdap ___/____/_____<br />
Polio Primary series 1.___/___/____ 2.___/___/____ 3.___/___/____ 4.___/___/____<br />
Varicella Two doses recommended if no 1.___/___/____ or documentation of Positive titer: ___/___/_____<br />
documented history of disease 2.___/___/____ or history of disease date: ___/___/_____<br />
Hep B Recommended 3 dose series 1.___/___/____ 2.___/___/____ 3.___/___/____<br />
HBSAA: ___/___/____ ☐ R or ☐ N-R<br />
Meningitis Recommended. If not received, 1.____/____/_____ 2.____/____/_____ ☐Menomune ☐Menactra ☐Menveo<br />
patient signature required on waiver I have been informed about the risks of Meningitis and decline the immunization at this time:<br />
to the right:<br />
Pt. Signature:______________________________________________ Date____/____/_____<br />
Hep A Recommended two dose series 1.____/____/_____ 2.____/____/_____<br />
HPV Recommended 3 dose series 1.____/____/_____ 2.____/____/_____ 3.____/____/_____<br />
Mantoux Required if Student is High Risk Placed:____/____/_____ Read:____/____/_____ Result:_____mm induration<br />
HX of previous<br />
BCG vaccine<br />
does not preclude<br />
Send copy of chest x-ray report:<br />
If > 10 mm induration, or positive IGRA, chest x-ray required<br />
Date: ____/_____/_____ Result:_________________________<br />
Mantoux testing if<br />
Send copy of lab report:<br />
IGRA Date:____/____/_____ Please specify: ☐ QFT-G ☐ QFT-GIT ☐ T-SPOT<br />
indicated high risk.<br />
Result: ☐ NEG ☐ POS ☐ INDETE. ☐ BORDERLINE (T-Spot ONLY)<br />
Provider Name (please print)<br />
Provider Signature<br />
Date<br />
Phone:<br />
Fax:<br />
Address<br />
or Office Stamp: