

Towards Safer Radiotherapy
Towards Safer Radiotherapy
Towards Safer Radiotherapy

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Chapter 2: Nature and frequency of<br />
human errors in radiotherapy<br />
In any system errors are inevitable but, by understanding why they occur, systems can be put into<br />
place to minimise their frequency and maximise detection before harm can be done. The actions<br />
and failures of individual people play a central role, but their thinking and behaviour is strongly<br />
influenced and constrained by their working environment and by wider organisational processes. 20<br />
Major incidents almost always evolve over time, involve a number of people and a number of<br />
broader contributory factors. For example, a change in a radiotherapy planning system without<br />
matching changes to other procedures may unexpectedly result in an error being made when a<br />
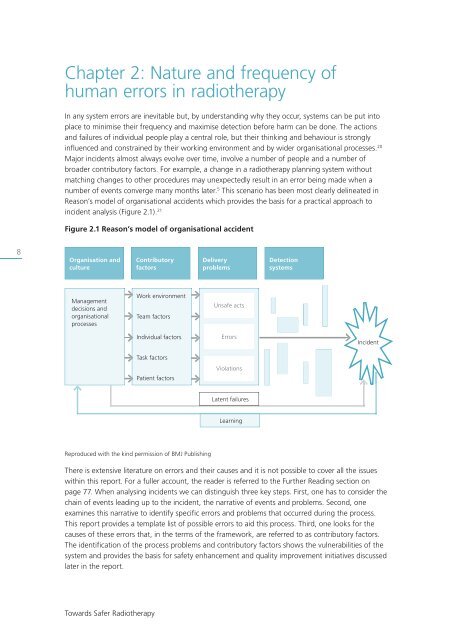
number of events converge many months later. 5 This scenario has been most clearly delineated in<br />
Reason’s model of organisational accidents which provides the basis for a practical approach to<br />
incident analysis (Figure 2.1). 21<br />
Figure 2.1 Reason’s model of organisational accident<br />
8<br />
Organisation and<br />
culture<br />
Contributory<br />
factors<br />
Delivery<br />
problems<br />
Detection<br />
systems<br />
Management<br />
decisions and<br />
organisational<br />
processes<br />
Work environment<br />
Team factors<br />
Unsafe acts<br />
✹<br />
Individual factors<br />
Task factors<br />
Patient factors<br />
Errors<br />
Violations<br />
Incident<br />
Latent failures<br />
Learning<br />
Reproduced with the kind permission of BMJ Publishing<br />
There is extensive literature on errors and their causes and it is not possible to cover all the issues<br />
within this report. For a fuller account, the reader is referred to the Further Reading section on<br />
page 77. When analysing incidents we can distinguish three key steps. First, one has to consider the<br />
chain of events leading up to the incident, the narrative of events and problems. Second, one<br />
examines this narrative to identify specific errors and problems that occurred during the process.<br />
This report provides a template list of possible errors to aid this process. Third, one looks for the<br />
causes of these errors that, in the terms of the framework, are referred to as contributory factors.<br />
The identification of the process problems and contributory factors shows the vulnerabilities of the<br />
system and provides the basis for safety enhancement and quality improvement initiatives discussed<br />
later in the report.<br />
<strong>Towards</strong> <strong>Safer</strong> <strong>Radiotherapy</strong>
