cary academy athletic training policy procedures manual (parent
cary academy athletic training policy procedures manual (parent
cary academy athletic training policy procedures manual (parent

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
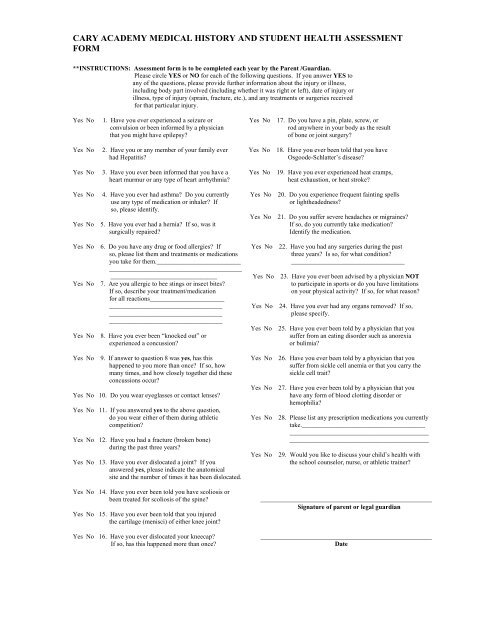
CARY ACADEMY MEDICAL HISTORY AND STUDENT HEALTH ASSESSMENT<br />
FORM<br />
**INSTRUCTIONS: Assessment form is to be completed each year by the Parent /Guardian.<br />
Please circle YES or NO for each of the following questions. If you answer YES to<br />
any of the questions, please provide further information about the injury or illness,<br />
including body part involved (including whether it was right or left), date of injury or<br />
illness, type of injury (sprain, fracture, etc.), and any treatments or surgeries received<br />
for that particular injury.<br />
Yes No 1. Have you ever experienced a seizure or Yes No 17. Do you have a pin, plate, screw, or<br />
convulsion or been informed by a physician<br />
rod anywhere in your body as the result<br />
that you might have epilepsy?<br />
of bone or joint surgery?<br />
Yes No 2. Have you or any member of your family ever Yes No 18. Have you ever been told that you have<br />
had Hepatitis?<br />
Osgoode-Schlatter’s disease?<br />
Yes No 3. Have you ever been informed that you have a Yes No 19. Have you ever experienced heat cramps,<br />
heart murmur or any type of heart arrhythmia?<br />
heat exhaustion, or heat stroke?<br />
Yes No 4. Have you ever had asthma? Do you currently Yes No 20. Do you experience frequent fainting spells<br />
use any type of medication or inhaler? If<br />
or lightheadedness?<br />
so, please identify.<br />
Yes No 21. Do you suffer severe headaches or migraines?<br />
Yes No 5. Have you ever had a hernia? If so, was it If so, do you currently take medication?<br />
surgically repaired?<br />
Identify the medication.<br />
Yes No 6. Do you have any drug or food allergies? If Yes No 22. Have you had any surgeries during the past<br />
so, please list them and treatments or medications<br />
three years? Is so, for what condition?<br />
you take for them.__________________________<br />
___________________________________<br />
_________________________________________<br />
_________________________________ Yes No 23. Have you ever been advised by a physician NOT<br />
Yes No 7. Are you allergic to bee stings or insect bites? to participate in sports or do you have limitations<br />
If so, describe your treatment/medication<br />
on your physical activity? If so, for what reason?<br />
for all reactions_______________________<br />
___________________________________ Yes No 24. Have you ever had any organs removed? If so,<br />
___________________________________<br />
please specify.<br />
___________________________________<br />
Yes No 25. Have you ever been told by a physician that you<br />
Yes No 8. Have you ever been “knocked out” or suffer from an eating disorder such as anorexia<br />
experienced a concussion?<br />
or bulimia?<br />
Yes No 9. If answer to question 8 was yes, has this Yes No 26. Have you ever been told by a physician that you<br />
happened to you more than once? If so, how<br />
suffer from sickle cell anemia or that you carry the<br />
many times, and how closely together did these<br />
sickle cell trait?<br />
concussions occur?<br />
Yes No 27. Have you ever been told by a physician that you<br />
Yes No 10. Do you wear eyeglasses or contact lenses?<br />
have any form of blood clotting disorder or<br />
hemophilia?<br />
Yes No 11. If you answered yes to the above question,<br />
do you wear either of them during <strong>athletic</strong><br />
Yes No 28. Please list any prescription medications you currently<br />
competition?<br />
take.______________________________________<br />
___________________________________________<br />
Yes No 12. Have you had a fracture (broken bone)<br />
___________________________________________<br />
during the past three years?<br />
Yes No 29. Would you like to discuss your child’s health with<br />
Yes No 13. Have you ever dislocated a joint? If you<br />
the school counselor, nurse, or <strong>athletic</strong> trainer?<br />
answered yes, please indicate the anatomical<br />
site and the number of times it has been dislocated.<br />
Yes No 14. Have you ever been told you have scoliosis or<br />
been treated for scoliosis of the spine?<br />
Yes No 15. Have you ever been told that you injured<br />
the cartilage (menisci) of either knee joint?<br />
Yes No 16. Have you ever dislocated your kneecap?<br />
If so, has this happened more than once?<br />
_____________________________________________________<br />
Signature of <strong>parent</strong> or legal guardian<br />
_____________________________________________________<br />
Date