guidelines for the management of urological cancer - Merseyside ...
guidelines for the management of urological cancer - Merseyside ...
guidelines for the management of urological cancer - Merseyside ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
For patients referred from <strong>the</strong> local MDT to <strong>the</strong> SMDT, <strong>the</strong> following in<strong>for</strong>mation is<br />
required:-<br />
• Muscle invasive TCC bladder<br />
• Staging results from <strong>the</strong> pelvic MR and abdominal/chest CT scan with radiology review<br />
where required<br />
• Histology report with pathology review where required<br />
• Assessment regarding fitness <strong>for</strong> radical treatment including<br />
• Co-morbidity, Life expectancy<br />
• Bladder symptoms, bladder pathology eg diverticulum, hydronephrosis<br />
• Hip replacements<br />
• Renal function<br />
• Bone biochemistry<br />
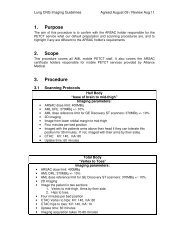
Radiology Guidelines<br />
Please refer to <strong>the</strong> Royal College <strong>of</strong> Radiologists <strong>guidelines</strong> attached<br />
http://www.rcr.ac.uk/<br />
Imaging <strong>of</strong> Cancer Patients<br />
Network approved imaging protocols are detailed in Appendix 9.<br />
6.1 Treatment <strong>of</strong> new non-muscle invasive tumours – see Figure<br />
2/Appendix 5<br />
At <strong>the</strong> first resection, as <strong>the</strong> histology is not available, those patients with clinically<br />
superficial bladder tumours receive intravesical MMC following resection.<br />
pTaG1 or pTaG2 – see Figure 3<br />
• Single dose <strong>of</strong> intravesical chemo<strong>the</strong>rapy at initial resection(S) [1,2]<br />
• MDT (S)<br />
• Cystoscopy at three months (S)<br />
• At 3 month cystoscopy, assign to a recurrence risk group (S), as follows.<br />
Initial Resection 3 month Cystoscopy Recurrence risk group<br />
Solitary tumour and clear low risk <strong>of</strong> recurrence<br />
Solitary tumour and recurrence medium risk <strong>of</strong> recurrence<br />
or<br />
Multifocal tumour and clear medium risk <strong>of</strong> recurrence<br />
Multifocal tumour and recurrence high risk <strong>of</strong> recurrence<br />
Page 13 <strong>of</strong> 44