Mercy Hospital Medical Staff Credentialing Manual - Mercy Health
Mercy Hospital Medical Staff Credentialing Manual - Mercy Health
Mercy Hospital Medical Staff Credentialing Manual - Mercy Health

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.1.1.11.Information about each voluntary and involuntary withdrawalfrom a medical staff or a voluntary or involuntary withdrawal ofan application for a medical staff appointment or ClinicalPrivileges; at any other hospital, health maintenance organization,health care entity or academic institution;2.1.1.12.Information about each pending or final suspension, revocationor restriction, or the voluntary or involuntary relinquishment ofan applicant’s:2.1.1.12.1.license to practice in any state;2.1.1.12.2.specialty board certification;2.1.1.12.3.state or federal narcotics registration certificate;2.1.1.12.4.ability to participate in any Federal <strong>Health</strong> Program;2.1.1.13.All professional malpractice claim information relative to theapplicant within the last ten (10) years2.1.1.14.Information about health status;2.1.1.15.Consent to submit to such physical or mental examination as theMEC may require. Taking or passing a physical or mentalexamination must not be a part of the application process, but theexercise of Clinical Privileges that are otherwise granted may bemade subject to the successful completion of such anexamination. The identity of the examining physician(s) must beby mutual consent. In the event of a disagreement concerning theneed for an examination or the identity of the examiningphysician(s), the matter must be referred to the Board, whosedecision on the matter is final;2.1.1.16.Consent to release of information from, and releases fromliability in favor of, insurance carriers, references, all institutionswhere applicant has worked, trained or practiced and to which hehas applied and all other sources of information required in theapplication, and consent to appear for an interview, if requested;2.1.1.17.Statement acknowledging and understanding <strong>Mercy</strong>Confidentiality policy;2.1.1.18.A Medicare fraud attestation;2.1.1.19. The initial applicant shall submit four (4) passport sizephotographs which will be attached to the release executed by theapplicant and distributed to references to confirm the applicant’sidentity;2
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.1.1.20.Verification that the applicant has received and reviewed theBylaws, Rules and Regulations and all policies of the <strong>Medical</strong><strong>Staff</strong> and of the <strong>Hospital</strong> relating to appointment to the <strong>Medical</strong><strong>Staff</strong> and the delineation of Clinical Privileges and that he agreesto be bound by them;2.1.1.21.A non-refundable application fee.2.1.1.22.Statement of Physician Expectations whereby the practitionerattests to having read and agrees to abide by the Expectations.2.1.1.23. <strong>Mercy</strong> <strong>Health</strong> supplemental forms, attestation, release and otherrelated documents.2.1.2. Applications for Reappointment: At least six months prior to theexpiration of a Member’s <strong>Medical</strong> <strong>Staff</strong> appointment, the CCO will sendthe Member a written reappointment form. The applicant must provide inhis reapplication, at a minimum, the following information or documents:2.1.2.1. Verification that all information provided on previousapplications remains correct, or updated information as necessary.The form must specifically seek, at a minimum, previouslyundisclosed information relating to:2.1.2.1.1.previously successful or currently pending challenges to anylicensure or registration or the voluntary relinquishment of suchlicensure or registration;2.1.2.1.2.voluntary or involuntary termination of medical staffmembership or voluntary or involuntary limitation, reduction orloss of clinical privileges at another hospital;2.1.2.1.3.Any evidence of an unusual pattern of an excessive number ofprofessional liability actions resulting in a final judgment againstthe applicant; involvement in each professional liability action,including all judgments and settlements within the past ten (10)years.2.1.2.1.4.relevant practitioner-specific data are compared to aggregatedata, when available; Performance Measurement Data includingmorbidity and mortality data when available; and2.1.2.2.Information about health status,2.1.2.3.Specific request for delineated Privileges,2.1.2.4. Sufficient clinical performance information to grant, limit or denythe requested privileges.3
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.1.3. Applications to Modify Status or Privileges: A Member may apply in writing fora change in his <strong>Medical</strong> <strong>Staff</strong> category, Department assignment or ClinicalPrivileges. Such an application must be in writing.2.1.4. Effect of Applications (Initial and Reappointment): Each person who signs theconsent and release and submits an application under this Article:2.1.4.1. Warrants that the information submitted with the application andon all prior applications, as amended, is complete and accurate;agrees that he will provide updated information as soon aspracticable concerning each change to a response to any questionon an application; and agrees that material misstatements,omissions or misleading statements may be grounds for suspensionor termination without a hearing under the Fair Hearing Plan;2.1.4.2. Consents to appear for such interviews and provide such additionalinformation or documents as any Professional Review Body mayrequire;2.1.4.3. Authorizes each Professional Review Body to consult with personswho may have information bearing on the applicant’squalifications;2.1.4.4. Consents to the inspection of all documents and the release of allinformation that any Professional Review Body may determine tobe relevant in assessing the applicant’s qualifications, including allrecords and documents pertaining to his or her licensure, specifictraining, experience, current competence and ability to perform theprivileges requested;2.1.4.5. Agrees to submit any reasonable evidence of current ability toperform the privileges requested and to submit to such physical ormental examination as the MEC may require. Taking or passing aphysical or mental examination must not be a part of theapplication process, but the exercise of Clinical Privileges that areotherwise granted may be made subject to the successfulcompletion of such an examination. The identity of the examiningphysician(s) must be by mutual consent. In the event of adisagreement concerning the need for an examination or theidentity of the examining physician(s), the matter must be referredto the Board, whose decision on the matter is final.2.1.4.6. Releases all <strong>Mercy</strong> Representatives, each Professional ReviewBody and its individual members from liability for acts performedin connection with the evaluation of the applicant’s qualifications;2.1.4.7. Releases all persons from liability who provide information,including information that is otherwise privileged or confidential,in connection with the evaluation of the applicant’s qualifications;4
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.1.4.8. Authorizes <strong>Mercy</strong> Representatives to release informationpertaining to the applicant’s qualifications to other hospitals,health care entities and authorized health care licensing, datacollection and reporting agencies, to the extent to which consentedin writing or permitted or required by law, and releases the<strong>Hospital</strong> Representatives for so doing;2.1.4.9. Acknowledges that he has received a copy of the Bylaws, Rulesand Regulations and all policies of the <strong>Medical</strong> <strong>Staff</strong> and of the<strong>Hospital</strong> relating to appointment to the <strong>Medical</strong> <strong>Staff</strong> and thedelineation of Clinical Privileges (and all revisions to thosedocuments), and that he understands them and agrees to be boundby them;2.1.4.10. Agrees to perform and abide by the obligations set forth underResponsibilities of <strong>Medical</strong> <strong>Staff</strong> Membership in the Bylaws,including the obligation to provide continuous care for his or herpatients;2.1.4.11. Agrees to comply with all state and federal laws regarding thepractice of medicine, including without limitation, the prohibitionsagainst fee splitting, antireferral and antikickback statutes;2.1.4.12. Agrees that in the event any Professional Review Body takes,recommends or considers the taking or recommending of aProfessional Review Action, he will exhaust all steps provided inthese Bylaws, including the provisions of the “ResolvingProfessional Competence, Conduct or Discipline Issues” Articleand the Fair Hearing Plan as his exclusive remedy.2.2. Processing Applications2.2.1. CCO General Function: The CCO will perform the following functionsrespecting all applications for <strong>Medical</strong> <strong>Staff</strong> membership or ClinicalPrivileges at each <strong>Mercy</strong> <strong>Hospital</strong> or affiliate2.2.1.1.Collect and organize all applications and associatedmaterials;2.2.1.2.Conduct all necessary primary source and otherverifications;2.2.1.3.Serve as repository of credentialing information;2.2.1.4.Provide Practitioner-specific credentialing information toeach <strong>Mercy</strong> <strong>Hospital</strong> or affiliate where a Practitionerapplies for or holds <strong>Medical</strong> <strong>Staff</strong> membership, ClinicalPrivileges.5
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.2.2. Confidentiality Safeguards: The CCO must establish and enforceappropriate safeguards to ensure that credentialing information --2.2.2.1.Is protected from disclosure to persons or organizationsother than <strong>Mercy</strong> <strong>Hospital</strong>s or affiliate, except upon awritten, dated release signed by the Practitioner anddirected specifically to <strong>Mercy</strong> <strong>Health</strong> Partners (MHP)authorizing such disclosure;2.2.2.2.Is provided only to persons at such <strong>Hospital</strong>s, affiliatesinvolved in pursuit of a legitimate credentialing function;and2.2.2.3.Is provided with the express caution that such informationis confidential and may not be further disclosed.2.2.3. Incomplete Applications: The duty to file a complete, signed application,rests exclusively with the applicant. Efforts by the CCO or others to assistin the collection of documents or information do not shift theresponsibility from the applicant in any respect. The rules related totimely submission of applications contained in the System-wide<strong>Credentialing</strong> Services Operations <strong>Manual</strong> will be strictly enforced:2.2.3.1.Initial Applicants: Initial applicants who file an incompleteapplication will receive a letter from the CCO requestingcompletion within a stated deadline. If the applicant doesnot comply within the deadline it is deemed voluntarilywithdrawn as of that date. The applicant may reapply bysubmitting a new application and an additional nonrefundableprocessing fee.2.2.3.2.Applicants for Reappointment: Applicants who fail toreturn a completed application for reappointment withintimeframes approved in the System-wide <strong>Credentialing</strong>Services Operations <strong>Manual</strong> will receive a letter from theCCO requesting completion. If the application is notsubmitted or remains incomplete the application will bedeemed voluntarily withdrawn at the end of the currentappointment.2.2.4. CCO Handling: All applications must be mailed or delivered to the CCO.When an applicant has properly filled in and signed his application, theCCO will do the following:2.2.4.1.For initial and applicants for reappointment2.2.4.1.1. Verify the applicant’s current licensure, specifictraining, experience and current competencethrough primary sources. Action on an initialapplication may not proceed until all thisinformation has been collected and verified;6
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.2.4.1.2.Query the National Practitioner Data Bank;2.2.4.1.3.Obtain professional malpractice claiminformation;2.2.4.1.4.Assure the presence of completed references andall other required forms and consents;2.2.4.1.5.Verify the status of privileges at other health carefacilities;2.2.4.1.6.Check for sanctions through the Office of theInspector General and the Excluded Provider ListSystem;2.2.4.2. Collection of statistical data to grant, limit or deny therequested privileges.2.2.4.2.1.Assure the presence of one peer reference and onehospital verification, if required; (reappointmentonly)2.2.5. Peer References: Recommendations from peers are obtained andevaluated for all new applicants for privileges. Upon renewal ofprivileges (reappointment), when insufficient practitioner-specific data areavailable, the medical staff obtains and evaluates peer recommendations.A recommendation from peers is defined as an appropriate practitioner inthe same professional discipline as the applicant who has personalknowledge of the applicant and the applicant’s ability to practice. Theyreflect a basis for recommending the granting of privileges. Sources forpeer recommendation may include the following:2.2.5.1.An organization performance improvement committee, the majority ofwhose members are the applicant’s peers;2.2.5.2.A reference letter(s), written documentation or documented telephoneconversation(s) about the applicant from a peer(s) who is knowledgeableabout the applicant’s professional performance and competence;2.2.5.3.A department or major clinical service chairperson who is a peer;2.2.5.4.The <strong>Medical</strong> Executive CommitteePeer recommendations include the following:2.2.5.5.Relevant training and experience2.2.5.6.Current competence2.2.5.7.Any effects of health status on privileges being requested7
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008of the review, interview and inquiry, the Chairperson must make a writtenrecommendation to the Credentials Committee relating to the requested status andClinical Privileges. The interview, if one is conducted, is not a hearing, and neither theinterview nor the recommendation entitles the applicant to any rights under the FairHearing Plan. Where the applicant is a Department Chairperson, the report will beprepared by the Credentials Committee.2.2.9. Credentials Committee Action: The Credentials Committee must review theApplication File, Department and peer recommendation(s). The Credentials Committeemust collect and consider available information concerning the applicant’s professionalconduct, performance and conduct both in the <strong>Hospital</strong> and at other health care entities.The Credentials Committee may conduct an interview and must make a record of theinterview and include the record in the Application File. At the conclusion of its review,the Credentials Committee must make a recommendation to the MEC pertaining to therequested <strong>Medical</strong> <strong>Staff</strong> status, staff category, Department assignment and ClinicalPrivileges, with suggested special conditions or limitations, if any.2.2.10 MEC Action: At its next regular meeting after receipt of the CredentialsCommittee report and recommendation, or as soon thereafter as is practical, the MECshall consider the Credentials Committee report and any other relevant information. TheMEC may request additional information, return the matter to the Credentials Committeefor further investigation, and/or elect to interview the applicant. The MEC shall thenprepare and forward to the Chief of <strong>Staff</strong>, for prompt transmittal to the Board, arecommendation as to <strong>Medical</strong> <strong>Staff</strong> appointment and, if appointment is recommended,as to membership category, Clinical Privileges to be granted and any special conditionsto be attached to the appointment.2.2.11 If the recommendation Affects Adversely the applicant’s membership or ClinicalPrivileges, the MEC must give Notice to the applicant of his right to a hearing inaccordance with the Fair Hearing Plan.2.2.12 Board Action: The Board must review each favorable recommendation of theMEC requesting <strong>Medical</strong> <strong>Staff</strong> appointment and Clinical Privileges.SUBCOMMITTEE OF THE BOARD: In lieu of review by the fullBoard, the Board may, pursuant to authority in the Board’s bylaws, directthat initial and reappointment applications which meet the criteria forexpedited credentialing and privileging process, and have receivedapproval by the Department Chair, Credentials Committee and <strong>Medical</strong>Executive Committee may be reviewed by a Board subcommittee of atleast two voting members of the governing body Only those applicantsthat qualify under <strong>Medical</strong> <strong>Staff</strong> Standard 4.35 of the ComprehensiveAccreditation <strong>Manual</strong> for <strong>Hospital</strong>s published by the Joint Commissionmay be reviewed. Approval of such applicants is effective as of the dateof approval by the designated subcommittee. An application which hasbeen deemed complete and has received approval by the DepartmentChair, Credentials Committee and the <strong>Medical</strong> Executive Committee shallbe forwarded to the Board Committee of two or more persons. The<strong>Medical</strong> staff uses criteria developed for the expedited process whenrecommending privileges. The following situations are evaluated on acase by case basis and usually are ineligible for Board Subcommitteeapproval if any of the following has occurred:9
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.2.12.1. Submission of an incomplete application;2.2.12.2 Recommendation from the Credentials or <strong>Medical</strong> ExecutiveCommittee that is adverse or with limitation.2.2.12.3 A current challenge or a previous successful challenge tolicensure or registration2.2.12.4. Involuntary termination of medical staff membership at anotherorganization.2.2.12.5. Involuntary limitation, reduction, denial or loss of clinicalprivileges; or,2.2.12.6. The hospital determines that there has been either an unusualpattern of, or an excessive number of, professional liability actionsresulting in a final judgment against the applicant.FULL BOARD:The actions of the Governing Board Subcommittee will be reported to the fullBoard at their next regular scheduled meeting.2.2.12.7. If the Board (or designated subcommittee) accepts therecommendation, its decision is final. The applicant will bepromptly notified of his department assignment, staff category,clinical privileges and any special conditions.2.2.12.8. If the full Board rejects a recommendation, and its decisionAffects Adversely the applicant’s membership or ClinicalPrivileges, it must direct the Chief Executive Officer to giveprompt Notice to the applicant of his right to a hearing inaccordance with the Fair Hearing Plan.2.2.12.9. If a designated committee of the board rejects therecommendation, the committee must refer it back to the MEC forfurther consideration.2,2.13 Time for Processing of Applications:2.2.13.1 Initial Applications: The application process must be completedwithin a reasonable time. The CCO should collect and verifyinformation within 41 days of the applicant’s delivery of theapplication. The Department Chairperson should prepare and deliverhis or her report to the Credentials Committee at its next regularmeeting. The Credentials Committee, MEC (except as may benecessary for JRC review) and the Board, in turn, should each act on anapplication at the next regular meeting following receipt of thepreceding recommendation. “Complete applications” (as defined in the<strong>Credentialing</strong> <strong>Manual</strong>) should normally be processed within 90 days,10
8his own personal experiences of realisation. The essential thing here—and the choice offormulation is intentionally provocative, but also quite literally accurate—is that Ibn ‘Arabî (likePlato) has no ‘teachings’ or ‘doctrines’ of his own. In other words, his constant emphasis and isto force his ‘readers’ to undertake their own indispensable effort of tahqîq (both ‘verification’and ‘realisation’). That is, they are intended to help his readers discover the essentialconnections between the ‘forms’ of revelation (or their endless social and historicaltransmutations) and their underlying realities as revealed in each individual’s experience; andthen to help them actualise the further demands of that haqq 7 which are inherent in its ongoingdiscovery.4. A further implication of each of the above-mentioned points is that Ibn ‘Arabî has nosingle or exclusive ‘audience’ for which his writings are intended. In particular, the interpreterof any of his typical works is faced in this regard with a strange double paradox. First, it isreadily apparent that most of those ‘people of God’ (to use Ibn ‘Arabî’s own pregnant expressionfor his true companions and ideal readers) who would be uniquely qualified to understand thesestrange writings, in his time or any other, do not ordinarily devote most of their time to readingbooks and pursuing similar intellectual pursuits. Yet most of Ibn ‘Arabî’s writings presupposenonetheless an rare and challenging intellectual mastery of religious and philosophic sciencesand Arabic literary forms which must have been relatively uncommon even in his own day (notto mention our own). The second, further paradox is the extraordinary, lasting (indeed oftenlifelong) interest which those writings have nonetheless for centuries tended to awaken andsustain in so many devoted students and readers, as evidenced by the profusion of well-annotatedmanuscripts in the past, and of extensive translations, elaborate studies and Arabic editions morerecently. An adequate resolution of this puzzle would require a book in itself, but two basicpreliminary observations can already be noted here. First, even a cursory reader of Ibn ‘Arabî’sworks will quickly notice that he was deeply suspicious of the increasingly institutionalisedforms of what would later be called ‘Sufism’ that he encountered during his lifetime, forperennial reasons (not at all limited to the historical or individual particularities of that age) that7 This underlying Arabic term, a favourite of Ibn ‘Arabî, encompasses both the divine ‘Reality’and all that is right and due or obligatory as an inseparable dimension of that same Reality.
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008Corp. (MRC), Emergency System for Advance Registration ofVolunteer <strong>Health</strong> Care Personnel( ESAR-VHP), or otherrecognized state or federal organizations or groups;2.3.1.4. Identification indicating that the individual has been grantedauthority to render patient care in emergency circumstances, withsuch authority having been granted by a federal, state or municipalgovernmental entity;2.3.1.5. Present Identification by a current hospital or medical staff memberwith personal knowledge regarding practitioner’s identityvolunteer’s ability to act as a licensed independent practitionerduring a disaster;2.3.1.6. The medical staff oversees the professional practice of volunteerlicensed independent practitioners.2.3.1.7. The organization makes a decision (based o information obtainedregarding the professional practice of the volunteer) within 72 hoursrelated to the continuation of the disaster privileges initially granted.2.3.2 The verification of information in accordance with the <strong>Medical</strong> <strong>Staff</strong> Bylaws formembership continues as a high priority during the implementation of theEmergency Management Plan.2.3.3 The physicians who are granted Disaster Privileges will report to the DisasterControl Center Chief <strong>Medical</strong> Officer for direction and management.Upon presentation of any of the information in 2.3.1 above, the Chief Executive Officer,or the Chief of <strong>Staff</strong> or their designees may grant disaster privileges on a case by case basis at hisor her discretion. Unless membership is granted pursuant to the Expedited <strong>Credentialing</strong> Policy,said privileges shall terminate when the Emergency Management Plan implementation isterminated, the immediate situation is under control and the practitioner to whom disasterprivileges have been granted has transferred care of patients treated during the emergency to amember of the <strong>Medical</strong> <strong>Staff</strong>. Furthermore, the Chief of <strong>Staff</strong> may terminate these privileges atany time and for any reason during the implementation of the Emergency Management Plan. Saidtermination shall not be considered a reportable event with the National Practitioner Data Bank.12
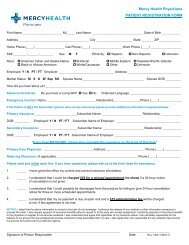
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008MERCY HEALTH PARTNERSDISASTER INFORMATION & RELEASE AUTHORIZATION FORM(WHEN THE EMERGENCY SITUATION NO LONGER EXISTS, THE DISASTER PRIVILEGES WILL BETERMINATED)APPLICANT’S NAME: ___________________________________________________SPECIALTY:_________________________ BOARD STATUS: __________________GROUP PRACTICE NAME: _______________________________________________OFFICE ADDRESS: _____________________________________________________Street City State ZipTELEPHONE: ( )____________________ FAX: ( )_________________RESIDENCE ADDRESS: _________________________________________________Street City State ZipTELEPHONE: ( )____________________ FAX: ( )_________________PRIMARY HOSPITAL NAME: _____________________________________________HOSPITAL ADDRESS: _________________________________________________Street City State ZipDATE OF BIRTH: ________________ SS # _______________________________MEDICAL LICENSURE #: _________ EXPIRATION: _____ STATE _____________DEA #: ________________________ EXPIRATION: __________________________MALPRACTICE INSURANCE CARRIER: ____________________________________LIABILITY COVERAGE LIMITS EQUAL TO $1M/$3M ____ YES ___ NOExpiration _____________* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *13
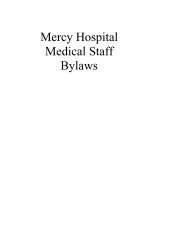
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008ADMINISTRATIVE COMPLETIONCredentials Presented :□□□□□Government Issued ID (driver’s license or passport) and <strong>Hospital</strong> ID BadgeGovernment Issued ID (driver’s license or passport) and <strong>Medical</strong> LicenseGovernment Issued ID (driver’s license or passport) and DMAT IdentificationGovernment Issued ID (drivers license or passport) and Identification indicating that theindividual has been granted authority to render patient care in emergencycircumstances, with such authority having been granted by a federal, state or municipalgovernmental entityGovernment Issued ID (drivers license or passport) and presents identification by acurrent hospital or medical staff member with personal knowledge regardingpractitioner’s identity volunteer’s ability to act as a licensed independent practitionerduring a disaster;Disaster Privileges Authorized by: _______________________ _____ Title______________<strong>Mercy</strong> Member Assigned to: ______________________________________________Location Assigned: ____________________________________ Time: _______* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *MEDICAL STAFF PERSONNELCredentials Verified by: __________________________________ Title _______________If unable to verify credentials within 72 hours of disaster, please indicate reason below:________________________________________________________________________________________________________________________________________________________14
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200815
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082.4 Monitoring Continuing EligibilityThe CCO will continuously monitor, verify and maintain current information on each<strong>Medical</strong> <strong>Staff</strong> Member respecting licensure, narcotics permits, TB Testing documentationas required by the Ohio Department of <strong>Health</strong>, and professional liability insurance.2.5 Applications for Return From Leave of Absence2.5.2 A Member whose appointment has not expired and who seeks return from a leaveof absence must file a written request to return. At a minimum, the request mustcontain:2.5.2.1 A summary of his or her activities during the period of leave; and2.5.2.2 Details of all medical training and experience and other circumstances duringthe period of leave demonstrating the maintenance of skills; and2.5.2.3 Evidence of current licensure, current professional liability insurance, currentcompetence and current ability to perform the privileges requested.2.5.3 The MEC may request any additional information it may require to assure that theMember is qualified for <strong>Medical</strong> <strong>Staff</strong> membership and possesses currentcompetence to exercise the Clinical Privileges to which he seeks to return.2.5.4 The <strong>Medical</strong> <strong>Staff</strong> Offices at each entity must conduct a National PractitionerData Bank query and primary source verification of licensure2.5.5 The MEC must process the request for return from leave, with the assistance andrecommendation of the Credentials Committee if desired, applying the samestandards as an applicant for reappointment.2.5.6 Reinstatement is not effective until approved by the Board.2.5.7 Where a Member’s appointment expires during the leave of absence, the MEC inits discretion may require a full initial application2.6 TelemedicineTelemedicine is the use of medical information exchanged from one site to another viaelectronic communications. The medical staff recommends which clinical services areappropriately delivered by licensed independent practitioners through this medium.The clinical services offered are consistent with commonly accepted quality standards.<strong>Mercy</strong> facilities are defined as the originating site, where the patient is located at thetime the service is provided.16
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008All licensed independent practitioners who are responsible for the patient’s care,treatment and services via telemedicine links are credentialed and privileged to do so atthe originating site through one of the following mechanisms:2.6.2 The originating site fully privileges and credentials the practitioner, according toThe JC standards2.6.3 The originating site privileges practitioners using credentialing information fromthe distant site if the distant site is a The JC accredited organization; or2.6.4 The originating site uses the credentialing and privileging decisions from thedistant site to make a final privileging decision if all the following requirements aremet:2.6.4.1. The distant site is a The JC accredited hospital or ambulatory careorganization;2.6.4.2 The practitioner is privileged at the distant site for those services to beprovided at the originating site;2.6.4.3 The originating site has evidence of an internal review of thepractitioner’s performance of these privileges and sends to the distant siteinformation that is useful to assess the practitioner’s quality of care,treatment, and services for use in privileging and performanceimprovement.3 CLINICAL PRIVILEGES3.1 Department Responsibility for PrivilegesEach Department must have a system for the development of delineation criteria, theadjustment of criteria to meet developing community needs and the state of medicalknowledge, and the monitoring of delineated Privileges. At a minimum, this systemmust:3.1.1 Make quality of patient care its main design objective;3.1.2 Establish and revise criteria that include, at a minimum, evidence ofcurrent licensure, relevant training or experience, current competence, andability to perform the Privileges requested;3.1.3 Ensure that quality of care among those with the same Privileges isuniform within Departments and, working with other Departmentchairpersons and <strong>Medical</strong> <strong>Staff</strong> leadership, uniform between Departmentsand among <strong>Medical</strong> <strong>Staff</strong> Members and non-Members;3.1.4 Ensure that where categories are used, they are clear and well-defined;17
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20083.1.5 Include mechanisms for ensuring that those who hold Clinical Privilegesremain within their respective delineations;3.1.6 Employ appropriate means of surveillance, including the results of<strong>Hospital</strong> quality monitoring, to assess the exercise of delineated Privileges;3.1.7 Where new Privileges are sought, privilege criteria are developed by theDepartment, reviewed by the Credentials Committee and the MEC andapproved by the Board before Privileges are granted to particularPractitioners.3.2 Processing Temporary Privileges3.2.1 Temporary privilege requests will be processed as promptly as possible ina manner consistent with the Bylaws.3.2.2 Initial Applicants Awaiting Credentials Committee, MEC or Board Action3.2.2.1 An applicant is considered for temporary privileges when allprimary source verifications have been completed, including, butnot limited to,• A complete application• Current licensure;• Relevant training and experience;• Current competence and ability to perform the privilegesrequested;• Results of the National Practitioner Data Bank query have beenobtained and evaluated;• The applicant has in force professional liability insurance asspecified by the Board, covering the exercise of the privilegesrequested;• No current or previously successful challenge to licensure orregistration• No voluntary or involuntary limitation, reduction, loss orsuspension of membership or clinical privileges at anotherorganization.3.2.2.2 Once the preceding requirements are met, temporary privilegesmay be granted for a limited period of time, not to exceed 120days, by the Chief Executive Officer (or designee) uponrecommendation of either the applicable clinical department18
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008chairperson or the chief of the medical staff (or their respectivedesignees) when the applicant’s file is awaiting review andapproval of the Credentials Committee, <strong>Medical</strong> ExecutiveCommittee or the Board of Directors.3.2.3 Temporary Privileges to Fulfill an Important Patient Care Need3.3 Locum Tenens3.2.3.1 Temporary privileges may be granted on a case-by-case basis whenthere is an important patient care need.3.2.3.2 Under these circumstances, the Chief Executive Officer (ordesignee) applicable clinical department chairperson or the chiefof the medical staff (or their respective designees) provided there isverification of current licensure and current competence. Inaddition, a query to the National Practitioner Data Bank isrequired. A documented Internet or telephone verification oflicensure is sufficient. A documented telephone call to a Physicianwith firsthand knowledge of the applicant’s current competencesuffices for verification of competence. Verification ofprofessional liability insurance must occur as soon as possible, andnot later than the next business day.Applications for Locum Tenens practitioners are processed in the same manneras an initial applicant.3.4 Procedural Sedation3.4.1 For the following specialties procedural sedation is included in the coreprivileging for those invasive procedures that normally utilize suchsedation: Anesthesiology, Cardiology, Emergency Medicine, ENT,Gastroenterology, General Surgery, Oral Surgery, Orthopedics, PlasticSurgery, Pulmonary Medicine, Radiology, Thoracic Surgery and VascularSurgeryIn order to perform procedural sedation, physicians must:Complete the MHP Procedural Sedation Competency Test and supplyrequired documentation to support the request.Monitoring for continued competency is performed at the individual sites,with outcomes provided for review at the time of request for privileges.4.0 LOW VOLUME/NO VOLUME PRACTITIONER POLICY FORREAPPOINTMENT APPLICANTS:LOW VOLUME PRACTITIONERS - The Practitioner that treats a majority or all ofhis or her patients at another facility.19
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008Those practitioners who have not had 24 patient encounters throughout <strong>Mercy</strong> <strong>Health</strong>Partners during a two-year period shall be required to have the department chair at his or herprimary facility complete a reference form which will include the following elements:• volume or clinical activity at that facility• confirmation of medical staff status, “in good standing with no disciplinary actions, nocontemplated investigations and no ongoing investigations or quality/review adverseaction,• confirmation that the physician is clinically competent in all areas covered by his or herrequested privileges.NO VOLUME PRACTITIONERS - The physician is not clinically active at anotherinstitution but is active within the community:Will be required to provide the names of two peers, to whom they refer patients forinpatient services (only one of which the practitioner may be affiliated with), to validatecompetency. These practitioners will be moved to Supplemental <strong>Staff</strong>.Those practitioners who have had no clinical activity at any facility within the previoustwo-year review period and who still request “clinical privileges” will be required to submitevidence of competency via a report card from a Managed Care Organization or otherdocumentation required by the Credentials Committee, <strong>Medical</strong> Executive Committee orGoverning Body.4.1 ALLIED HEALTH PROFESSIONAL – CREDENTIALING PLANSCOPE<strong>Mercy</strong> <strong>Health</strong> Partners has identified categories of healthcare professionals (hereinafterreferred to as Allied <strong>Health</strong> Professionals or AHPs) that may be needed to provide patient careservices within the <strong>Mercy</strong> <strong>Health</strong> Partners system. These healthcare professionals are noteligible to be members of the medical staff organizations. They are, however, given permissionto practice at <strong>Mercy</strong> <strong>Health</strong> Partners sites pursuant to this policy. The purpose of this policy is toestablish minimum standards and procedures.This policy applies to the following AHPs:1. Licensed mid-level practitioners supervised by or in collaborative practice withmembers of the medical staff, specifically Physician Assistants (PAs) and Advanced PracticeNurses(APNs). These individuals may be employed by <strong>Mercy</strong> <strong>Health</strong> Partners oremployed/sponsored by a member of the medical staff (Category 1); and1).2. AHPs who are employed/sponsored by a member of the medical staff (Category20
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008This policy does not apply to AHPs whose discipline is listed in Category 2 but who areemployed by <strong>Mercy</strong> <strong>Health</strong> Partners or who have a contractual arrangement with <strong>Mercy</strong> <strong>Health</strong>Partners (by individual, group or staff agency contract or lease).The Governing Board, with recommendations from Administration and the <strong>Medical</strong>Executive Committee, shall approve categories of AHPs who may practice at its site as well asgrant clinical privileges or authorization to practice to each AHP. If AHP services are alreadyprovided by <strong>Mercy</strong> <strong>Health</strong> Partners associates, the Governing Board may choose to disapprovethat category. Governing Board, <strong>Medical</strong> <strong>Staff</strong>s and management staff are involved in thecredentialing or authorization process for AHPs.PURPOSEThe purpose of this <strong>Credentialing</strong> Plan (“Plan”) is:1. To establish the procedures to assess, evaluate and review the qualifications,professional conduct, quality and appropriateness of care provided by AHPs in approvedcategories; and2. To establish the procedures and guidelines for consideration of new categories ofAHPs to practice at <strong>Mercy</strong> <strong>Health</strong> Partners facilities and sites, based upon the available medicalresources, equipment, supplies and staff, patient convenience, community need, quality of care,efficiency of operations, provider qualifications, and other business and patient care objectivesof <strong>Mercy</strong> <strong>Health</strong> Partners.III.CATEGORIESCategory 1- Physician Assistants (PAs)-Advanced Practice Nurses (APNs) – including Certified Registered Nurse Anesthetist,Certified Nurse Midwife, Advanced Practice Nurse, Certified Clinical Nurse SpecialistPAs must be: 1) credentialed through medical staff processes, 2) granted delineatedclinical privileges, 3) afforded rights of hearing as set forth in this Plan but not a <strong>Medical</strong> <strong>Staff</strong>Fair Hearing Plan, 4) monitored through the hospital’s performance improvement activities, 5)subject to reappointment and evaluation at least every two years through medical staff processesand, 6) subject to all The JC standards relevant to practitioners with delineated clinicalprivileges.APNs are subject to all of the above except with regard to the credentialing process,which may be the same as, or equivalent to the <strong>Medical</strong> <strong>Staff</strong> process in one of the followingways:a) same as PAs,b) same as PAs with the additional participation of a Nurse Management Reviewer, or21
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008c) the same as PAs but with a hospital Nurse Management Review taking the place ofthe MS Credentials Committee in the credentials review process.Category 2• Dental Assistant• Intraoperative Monitoring Technician• Orthopedic Technician• Perfusionist• Registered Nurse• Scribes• Scrub Nurse• Social Worker• Surgical Assistant• Surgical TechnicianThe scope of practice is set forth in the approved AHP Category Description. Thesepractitioners have no right to review of an action negatively affecting their ability to practice.AHP 2s (sponsored by members of any <strong>Mercy</strong> <strong>Health</strong> Partners <strong>Medical</strong> <strong>Staff</strong>) will becredentialed using The JC Human Resources Standards. <strong>Mercy</strong> Employed Clinician whosupervises the area/unit in which the AHP most frequently provides services (for example, theSurgery Supervisor for Surgical Assistants) Department Chair, and Credentials Committee Chairare to review applications, and if approved, the latter shall report approvals to the CredentialsCommittee, <strong>Medical</strong> Executive Committee and Governing Board. Ongoing monitoring ofclinical competence and performance evaluation will be performed by <strong>Mercy</strong> EmployedClinician who supervises the area/unit in which the AHP most frequently provides services (forexample, the Surgery Supervisor for Surgical Assistants) and sponsoring physician (ifapplicable) using data provided by performance improvement department.CREDENTIALING CRITERIA<strong>Credentialing</strong> criteria for each type of Allied <strong>Health</strong> Professional shall include, at least,the following:a. Education22
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008b. Trainingc. Licensure/Certificationd. Experiencee. Current Competencef. Collaborative Agreement (Advanced Practice Nurses), Physician Supervisory Plan(Physician Assistant)g. Continuing Educationh. Requirements for Supervisioni. Professional Referencesj. Ability to Performk. Identification of medical staff member(s) providing supervision/sponsorshipl. Evidence of continuing comprehensive professional liability insurance coverage in theamount of $1,000,000/ $3,000,000. (If an AHP is covered under the employingphysician’s policy, the AHP must submit documentation from the professional liabilityinsurer which acknowledges coverage for the physician’s employment or supervision ofAHPs and, if the physician group employs the AHP, indicates that the specific AHP, byname, is covered by the policy in the amounts required in this Plan.)APPLICATION PROCESSA. Release of ApplicationAn AHP shall be provided an application only where an <strong>Mercy</strong> <strong>Health</strong> Partners <strong>Hospital</strong>Governing Board has approved the AHP category/profession and an appropriate categorydescription.B. Application and FeeAHPs shall be credentialed in accordance with this Plan and shall bear the actual costs of thecredentialing process. AHPs must complete the State of Ohio application form in its entiretyalong with <strong>Mercy</strong> <strong>Health</strong> Partners supplemental forms, attestation, release and other relateddocuments, and submit the application fee.C. Burden of Providing InformationAHPs shall have the burden of producing information deemed adequate by <strong>Mercy</strong> <strong>Health</strong>Partners for a proper evaluation of current competence, character, ethics and other qualificationsand for resolving any doubts about such qualifications. An application is not complete unlessthe application form is completed, all items required to be verified are completed, and anyadditional information necessary to evaluate the applicant’s qualifications has been provided. If,after 30 days (from the date of signature), the application is incomplete due to outstandinginformation, documents, verification/references, the application shall be automaticallywithdrawn, and the applicant shall be notified that the application will not be considered.23
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008The provision of information by an applicant which contains material misrepresentations,misstatements, omissions or inaccuracies, whether intentional or not, and /or failure of anapplicant to sustain the burden of providing adequate information for the evaluation of theapplicant’s qualifications, shall result in denial of the application.If such misrepresentations, misstatements, omission or inaccuracies are discovered after theapplicant has been authorized for clinical duties, the ability to practice shall be immediatelyterminated.D. VerificationThe following shall be verified with the primary source for all AHPs:1. Licensure, certification and/or registration, as applicable to the AHP category.2. Professional education and training.3. Employers for the past five years, as applicable (dates and services provided and/or jobclassification). If previously employed by <strong>Mercy</strong> <strong>Health</strong> Partners, check with HRassociate database to verify affirmative “rehire” status.4. Competence questionnaires completed by health care professionals who have workedwith the AHP in the last 2 years. (Number of references and type of health careprofessionals completing questionnaire to be defined in the AHP Category Description.)5. Medicare/Medicaid Sanctions.6. National Practitioner Data Bank.Additional items may be verified, depending upon the AHP Category Description.E. Screenings (cost to be the responsibility of the AHP and/or sponsoring physician)All screenings must be complete, documented and in the credentialing file prior to the AHPproviding any services.All AHPs must:1. meet the minimum screening requirements as outlined in the Human ResourcesDepartment.2. authorize a Criminal Background check by <strong>Mercy</strong> <strong>Health</strong> Partners Central <strong>Credentialing</strong>Office3. submit a drug screening report that meets the requirements of <strong>Mercy</strong> <strong>Health</strong> Partners andhas been performed at the time of application.24
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008Evaluation of ApplicationsThe following guidelines shall be used to evaluate completed applications by the responsibleparties as set forth in Section III:1. The applicant meets the applicable criteria and qualifications for all requested clinicalduties.2. The applicant submits signed Supervisory or Collaborative Agreement/PhysicianSupervisory Plan (if applicable) which meets criteria set forth in this Plan.3. The applicant has received positive references with respect to the applicant’s competenceand ability to work cooperatively with others in the hospital and ambulatory settings.4. The applicant has not had any restrictions, suspensions, probations, or revocations of theapplicant’s clinical services at a health care facility or managed care plan or of the applicant’sprofessional license or certification, and if previously employed by <strong>Mercy</strong> <strong>Health</strong> Partners, has“rehire” status.5. The applicant has not had any disciplinary actions or investigations by any licensing orcertifying authority, health care facility or health care plan including Medicare/Medicaid.6. The <strong>Hospital</strong> has determined that there has been either an unusual pattern of, or anexcessive number of, professional liability actions resulting in a final judgment against theapplicant.7. There are no other indications that the applicant does not meet the qualifications forclinical duties.POST APPROVALA. OrientationAHPs must receive a general orientation to <strong>Mercy</strong> <strong>Health</strong> Partners and to the facility(s)area(s) in which each AHP will be providing services.1. General Orientation - A general orientation program for AHPs will be provided by<strong>Mercy</strong> Employed Clinician who supervises the area/unit in which the AHP most frequentlyprovides services (for example, the Surgery Supervisor for Surgical Assistants) but not limited totraining on HIPAA confidentiality, Corporate Compliance and other pertinent hospital policies.2. Orientation to Specific Patient Care Areas - AHPs shall also be oriented to the specificpatient care areas in which the AHP will provide services. Responsibility for provision25
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008of the department-specific orientation will be the responsibility of the <strong>Mercy</strong> EmployedClinician who supervises the area/unit in which the AHP most frequently providesservices (for example, the Surgery Supervisor for Surgical Assistants).B. Responsibilities of all AHPsAs a condition of the ability to practice within <strong>Mercy</strong> <strong>Health</strong> Partners, each AHP shall:1. Abide by all applicable state and federal laws regulating health care providers.2. Abide by and comply with all applicable bylaws, policies, rules, regulations andrequirements in force during the time the individual is granted permission to practice at<strong>Mercy</strong> <strong>Health</strong> Partners including <strong>Mercy</strong> <strong>Health</strong> Partners Mission, Values and Philosophy.3. Maintain all qualifications to perform as an AHP.4. Submit to such physical and/or mental examinations(s) or provide documentation ofcurrent health status as may be required to verify the AHPs ability to fully meet his/herresponsibilities and/or to perform the requested clinical duties.5. Document in patient medical records in a complete and timely fashion only to the extentauthorized in the AHP scope of practice.6. At all times observe and promote the confidentiality of patient health information.7. Disclose to patients the individual’s status as an Allied <strong>Health</strong> Professional and wear an<strong>Mercy</strong> <strong>Health</strong> Partners approved name tag identifying themselves at all times while at afacility which is part of <strong>Mercy</strong> <strong>Health</strong> Partners. The name tag will be different fromthose worn by <strong>Mercy</strong> <strong>Health</strong> Partners employees.8. Provide continuous and timely care to all patients for whom the individual hasresponsibility.9. Cooperate in performance improvement and quality monitoring activities of <strong>Mercy</strong><strong>Health</strong> Partners.10. Work cooperatively and professionally with medical staff and <strong>Mercy</strong> <strong>Health</strong> Partnersassociates.11. Provide to the <strong>Credentialing</strong> <strong>Staff</strong>, updates and modifications to his/her credentials dataas follows:a. revocation, suspension, restriction or probation of State professional license orother certification; Medicare or Medicaid sanctions; revocation or restriction of privilegesor permission to practice at any health care institutions; any lapse in professional liabilityinsurance coverage required by <strong>Mercy</strong> <strong>Health</strong> Partners; a conviction of a felony,drug/alcohol related misdemeanors or other crimes bearing on risk to patient safety;26
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008receipt of notice of any formal charges or the commencement of a formal investigation byany professional regulatory or licensing agency; the filing of charges by the Department of<strong>Health</strong> and Human Services; Peer Review Organization, or any law enforcement agency orhealth regulatory agency of the United States or the State of Ohio, initiation, settlement orentry of a final judgment against the AHP for professional liabilityb. any other change in the information from the date the AHP knew of the change.SUPERVISORY AND COLLABORATIVE RELATIONSHIPSA. Physician Supervisory Plans for Physician Assistants and Collaborative Agreements forAdvanced Practice NursesPhysician Assistants are required to obtain Physician Supervisory Plans which have been signedby the AHP and each supervising physician. Advanced Practice Nurses (APNs) (excludingCRNAs) are required to obtain Collaborative Agreements which have been signed by the AHPand the appropriate physician. A copy of the agreement will be maintained in the AHP’scredentialing files. The Agreement shall describe the arrangements for personal and responsiblesupervision or collaboration which have been made between the AHP and the physician. It isalso the responsibility of the AHP and the physician to provide the <strong>Hospital</strong>(s), in a timelymanner, with any revisions or modifications that are made to the agreement. The Agreementmust meet all requirements of applicable laws and regulations, as well as all criteria set forth inthis Plan and the applicable AHP Position Description.It is the AHP’s responsibility to obtain the Agreement and to adhere to the requirements of theAgreement. Failure to do so may result in termination of the AHP’s authorization to practice.B. Supervising PhysiciansEach supervising physician must annually sign an acknowledgment for each AHP, acceptingresponsibility for the actions of the AHP and agreeing to provide appropriate supervision of theirservices.The number of Dependent Practitioners acting under the supervision of one physician, as well asthe acts they may undertake, shall be consistent with applicable State statutes and regulations,the rules and regulations of the <strong>Medical</strong> <strong>Staff</strong> and policies of <strong>Mercy</strong> <strong>Health</strong> Partners. An AHPmay have multiple physician supervisors, as permitted by law (for example: a physicianassistant may work for more than one physician).In the event the <strong>Medical</strong> <strong>Staff</strong> appointment or clinical privileges of the supervising physiciancease for any reason (including suspension for incomplete medical records), permission for theAHP to practice at the <strong>Hospital</strong> and scope of practice shall automatically cease unless or until the27
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008<strong>Medical</strong> <strong>Staff</strong> Office is notified of a replacement supervisor and has received and approved allappropriate documents required under this policy.CREDENTIALS FILESEach AHP will have a credentials file which is maintained by the <strong>Medical</strong> <strong>Staff</strong> Office.IPERFORMANCE AND CLINICAL COMPETENCE EVALUATIONS OF AHPsA. AHP Category 1s will be evaluated as part of the bi-annual medical staff reappointmentprocess.B. AHP Category 2s1. Annual Performance ReviewAHP Category 2s shall have an annual performance review and a clinicalcompetence evaluation by the appropriate Supervising Physician and anAdministrative Review by the <strong>Mercy</strong> Employed Clinician who supervises thearea/unit in which the AHP most frequently provides services. Completedperformance evaluations shall be forwarded to the <strong>Medical</strong> <strong>Staff</strong> Office prior tothe AHP’s anniversary date.2. Clinical CompetenceThe clinical competence of AHP Category 2s will be evaluated according toHuman Resources policies and procedures and The JC standards through reviewby peers.Competency reviews shall be forwarded to the <strong>Medical</strong> <strong>Staff</strong> Office at least 60days prior to the AHP’s anniversary date and shall be evaluated as part of theannual performance evaluation process.3. Quality ReviewThe quality management/performance improvement department shall screen andreview any case(s) in which a quality issue has been identified. A report shall beprepared of all screened/reviewed cases. Cases in which problems are identifiedshall be referred to the Advisory Committee.CATEGORY DESIGNATION AND APPROVAL OF ADDITIONAL AHP TYPES28
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008- Certification (and maintenance thereof) by certification organizations approved by IDPR(listed on the IDPR web site www.idpr.com/who/ar/apn.asp); or Certification Board forUrologic Nurses and Associates as a Urologic Nurse PractitionerCertified Clinical Nurse Specialist- Current Ohio licensure as an Advanced Practice Nurse - Clinical Nurse Specialist- Certification (and maintenance thereof) by the certification organizations approved byIDPR (listed on the IDPR web site www.idpr.com/who/ar/apn.asp)Physician Assistant- Completion of an ARC-PA accredited program (masters degree preferred) in PhysicianAssistant Practice, consistent with Ohio Law.- Current certification (and maintenance thereof) by NCCPA- Current Ohio licensure as a Physician AssistantCATEGORY 2Audiologist- Evidence of a Master’s Degree in speech-language pathology or audiology from aprogram approved by the Ohio Department of Professional Regulation- Current Ohio licensure as a Speech Language Pathologist or AudiologistDental Assistant- Graduation from a program accredited by the American Dental Association’sCommission on Dental AccreditationInteroperative Monitoring Technician- MA, MS, Ph.D. or Au.D from a graduate program in Audiology accredited by the AmericanSpeech-Language Hearing Association; or Foreign Trained MD Degree, or B.A., B.S. degree inrelated science field.- Requires board certification ABNM (American Board of Neurophysiological Monitoring) orABRET (American Board of Registration of Electroencephalographic and EvokedPotential Technologists), D.ABNM (Diplomat of the American Board of NeurophysiologicalMonitoring), or a Certified Neurophysiological Intraoperative Monitoring (CNIM)Orthopedic Technician- Completion of an Orthopedic Technician Training Program- Certification (and maintenance thereof) by the National Association of OrthopedicTechnologists (NAOT)Perfusionist- Graduation from a school accredited by the Commission on the Accreditation of Allied<strong>Health</strong> Education Programs (CAAHEP)- Certification (and maintenance thereof) by the American Board of CardiovascularPerfusion (ABCP)Registered Nurse30
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008- Current Ohio licensure as a Registered NurseScribes (Emergency Department)- High School Diploma. A strong interest and/or involvement in a medical field,premedical students, nursing students, EMT and EMT students.Scrub Nurse- Current Ohio licensure as a Registered NurseSocial Worker- Current State of Ohio licensure as a Clinical Social Worker- Two years of full-time experience in psychiatric social work with prior experience in ahospital or partial hospital setting- Social workers with child psychology practices must have training with children/families.Surgical Assistant- Graduation from a program accredited by the Commission on Accreditation of Allied<strong>Health</strong> Education Programs (CAAHEP)- Current (and maintenance, thereof) certification by the National Surgical AssistantAssociation (CSA)Surgical Technician- Graduation from a program accredited by the Commission on Accreditation of Allied<strong>Health</strong> Education Programs (CAAHEP)- Current certification (and maintenance thereof) as a Certified Surgical Technologist(CST)Section 6. HEALTH ASSESSMENT/TUBERCULOSIS SCREENING PROGRAM FORMEDICAL/ALLIED HEALTH PROFESSIONALS INVOLVED WITH MATERNITYUNIT, CARDIAC CATH LAB AND RADIATION ONCOLOGY DEPARTMENTSPURPOSE:The purpose of this policy is to provide direction and guidelines for monitoring and complyingwith the Ohio Department of <strong>Health</strong> Administrative Code regarding TB Testing for thosepractitioners utilizing the following services within the hospital: Maternity Units, Cardiac CathLabs and Radiation Oncology Departments. This requirement will be incorporated in the coreprivilege forms as a necessary requirement for all <strong>Medical</strong> <strong>Staff</strong> Members and Allied <strong>Health</strong>Practitioners who may utilize these services within <strong>Mercy</strong>.This policy reflects the Ohio Department of <strong>Health</strong> Administrative Code Section 3701-84 as itpertains to hospital maternity units and maternity homes, Cardiac Cath lab and RadiationOncology Department which requires all persons involved with patients and activities in thematernity unit, Cardiac Cath lab and Radiation Oncology Department to have a health evaluationand a tuberculin test on an annual basis.31
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008<strong>Medical</strong>/Allied <strong>Health</strong> Professional <strong>Staff</strong> Members (practitioners and specified health personnel)are required to undergo PPD Testing or show evidence of testing as outlined in the surveillanceguidelines. A letter notifying them of the need for health exam and PPD testing will be sent bythe Central <strong>Credentialing</strong> Office on a yearly basis.The charge for the annual PPD testing will be incurred by <strong>Medical</strong> <strong>Health</strong> Partners if <strong>Mercy</strong>Employee <strong>Health</strong> is utilized. Further follow-up testing/treatment will be the responsibility of the<strong>Medical</strong>/Allied <strong>Health</strong> Professional <strong>Staff</strong> Member.Follow-up of positive PPD testing will be coordinated through the <strong>Medical</strong> Director ofEmployee <strong>Health</strong> Services and the Chief of <strong>Staff</strong>.TUBERCULOSIS SURVEILLANCE PROGRAM FOR HEALTH CARE WORKERSI. GENERAL GUIDELINESA. BASELINE TESTING1) All <strong>Medical</strong> <strong>Staff</strong>/Allied <strong>Health</strong> Personnel in the Maternity Unit,Cardiac Cath Labs and Radiation Oncology Departments will be skintested annually for TB using the Mantoux Method of intradermalinjection of PPD (purified protein derivative).2) All <strong>Medical</strong> <strong>Staff</strong>/Allied <strong>Health</strong> Personnel who receive BCG vaccinewill be included in the screening process to establish a baseline. Theywill be given the option to receive a PPD skin test or have a chest x-ray.3) A <strong>Medical</strong> <strong>Staff</strong>/Allied <strong>Health</strong> Professional staff Member who presentsas a known positive TB reactor will be exempt from PPD testing. All<strong>Medical</strong> <strong>Staff</strong>/Allied <strong>Health</strong> members with a history of a Positive PPDreaction will have a chest x-ray as part of the baseline TB SurveillanceProgram and will be assessed for signs and symptoms of active TB. Arepeat chest x-ray will be necessary only if signs and symptoms of TBOccur.4) When a skin test conversion, abnormal chest x-ray or signs/symptomsof TB occur, directions on how to proceed can be found in theemployee health departments.5) Evidence of no active TB will be based on one of the following:a. Negative PPD skin testb. Known positive PPD Skin Test and absence of clinical signs andsymptoms of active TBc. Newly converted positive PPD skin test with radiologist’sverification of normal chest x-ray.B. ANNUAL PPD SKIN TESTINGEvidence of annual PPD skin testing will be required of all practitioners who have privileges inthe maternity units, cardiac cath laboratories and Radiation Oncology Departments. AllPPD skin testing must be administered and read by a <strong>Health</strong> Care Professional who has been32
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 20082) Physicians who fail to provide documentation of current TB Testinginformation shall be forwarded to the <strong>Medical</strong> <strong>Staff</strong> Offices forassistance in obtaining documentation. Failure to provide upon requestwill result in loss of privileges until documentation of current TB testinformation is provided.SECTION 7. NEW TECHNOLOGIES/NEW PROCEDURES (see following pages):34
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200835
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200836
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200837
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200838
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200839
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200840
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200841
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200842
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200843
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 200844
CREDENTIALING MANUAL REVISED AND APPROVED BY THE BOARD OF DIRECTORS JANUARY 24, 2008ADOPTED by the <strong>Medical</strong> Executive Committee on the dates indicated below:<strong>Mercy</strong> <strong>Hospital</strong> Anderson: January 21, 2008<strong>Mercy</strong> <strong>Hospital</strong> Clermont: January 10, 2008<strong>Mercy</strong> <strong>Hospital</strong> Fairfield: January 15, 2008<strong>Mercy</strong> Franciscan - Mt. Airy: January 8, 2008<strong>Mercy</strong> Franciscan - Western Hills: January 22, 2008Approved by the Board of Trustees: January 24, 200845