Breast radiotherapy in women with pectus excavatum ... - Quantason
Breast radiotherapy in women with pectus excavatum ... - Quantason
Breast radiotherapy in women with pectus excavatum ... - Quantason

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
The British Journal of Radiology, 79 (2006), 785–790SHORT COMMUNICATION<strong>Breast</strong> <strong>radiotherapy</strong> <strong>in</strong> <strong>women</strong> <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong> (funnelchest): is the lateral decubitus technique an answer? A dosimetricstudyM A BOLLET, MD, F CAMPANA, MD, Y M KIROVA, MD, R DENDALE, MD, M-G SALIOU, MD,J-C ROSENWALD, PhD and A FOURQUET, MDDepartment of Radiation Oncology, Institut Curie, Paris, FranceABSTRACT. <strong>Breast</strong> <strong>radiotherapy</strong> is a technical challenge <strong>in</strong> <strong>women</strong> <strong>with</strong> <strong>pectus</strong><strong>excavatum</strong>. We aim to assess isocentric lateral decubitus (ILD) technique as a means toirradiate breasts for patients <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong>. Four <strong>women</strong> present<strong>in</strong>g <strong>with</strong> leftsidedbreast cancers and found to have <strong>pectus</strong> <strong>excavatum</strong> were offered breastconserv<strong>in</strong>gtreatments. Post-operative breast <strong>radiotherapy</strong> was <strong>in</strong>dicated (50 Gy) <strong>in</strong> twopatients, <strong>with</strong> an additional boost to the tumour bed (16 Gy). Both ILD and sup<strong>in</strong>etechniques were simulated. We report the dosimetric comparison of these techniquesand the acute sk<strong>in</strong> toxicity of ILD <strong>radiotherapy</strong>. ILD permitted the same breast dosehomogeneityas the sup<strong>in</strong>e technique while decreas<strong>in</strong>g breast thickness by 4.5–6.8 cm.The width of lung and/or heart receiv<strong>in</strong>g . 20 Gy ranged between 2.1 cm and 4.3 cm<strong>with</strong> the sup<strong>in</strong>e technique and between 0.5 cm and 1.1 cm <strong>with</strong> ILD. The estimatedpercentage of ipsilateral lung receiv<strong>in</strong>g . 20 Gy ranged from 21% to 34% <strong>with</strong> thesup<strong>in</strong>e technique and from 0% to 5% <strong>with</strong> ILD. Acute sk<strong>in</strong> toxicity was scored 1 for allpatients at completion of ILD <strong>radiotherapy</strong>. ILD is an effective breast <strong>radiotherapy</strong>technique for patients <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong> that preserves the underly<strong>in</strong>g heart andlung from unnecessary toxicity.Received 6 January 2006Revised 3 May 2006Accepted 30 May 2006DOI: 10.1259/bjr/23839243’ 2006 The British Institute ofRadiology<strong>Breast</strong> conserv<strong>in</strong>g treatment is considered as standardmanagement for early-stage breast cancer when technicallyfeasible. Post-operative <strong>radiotherapy</strong> to the breast isan important part of the treatment and has been shownto significantly dim<strong>in</strong>ish the rate of local relapse, the rateof breast cancer mortality and the risk of overallmortality [1]. However, the irradiation of normal tissues,especially of the underly<strong>in</strong>g lung and left ventricle, canlead to lethal complications expla<strong>in</strong><strong>in</strong>g the <strong>in</strong>crease <strong>in</strong>non-cancer related deaths. The risk of late toxicities suchas radiation-<strong>in</strong>duced pneumonitis or coronary morbidityhas been related to the volume of, respectively, underly<strong>in</strong>glung and left ventricle receiv<strong>in</strong>g a dose higher than20–25 Gy [2–4].The standard breast radiation technique uses tangentialfields delivered to the breast <strong>in</strong> a sup<strong>in</strong>e position [5].In the case of <strong>women</strong> present<strong>in</strong>g <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong>,a congenital deformation of the anterior chest walllead<strong>in</strong>g to a deep depression of the sternum, alsodescribed as funnel chest, this sup<strong>in</strong>e technique exposestoo much of the underly<strong>in</strong>g lung and/or left ventricle <strong>in</strong>the treatment fields. To try and comply <strong>with</strong> the twocontradictory breast <strong>radiotherapy</strong> requirements of breastdose homogeneity and lung/heart preservation presentsAddress correspondence to: Marc A Bollet, MD, Institut Curie,Radiotherapy Department, 26, rue d’Ulm, 75005 Paris, France.E-mail: marc.bollet@curie.net.a particularly difficult technical challenge that, up tonow, has been dealt <strong>with</strong> by us<strong>in</strong>g sophisticated threedimensional,<strong>in</strong>tensity-modulated <strong>radiotherapy</strong> (IMRT)or proton therapy techniques [6–8]. In this study wepresent a convenient solution: the isocentric lateraldecubitus technique (ILD). <strong>Breast</strong> irradiation <strong>in</strong> thelateral decubitus set-up was orig<strong>in</strong>ally developed for<strong>women</strong> <strong>with</strong> large, pendulous breasts and has been usedto treat thousands of patients [9]. The need to comply<strong>with</strong> modern requirements has prompted our departmentto adapt the technique to an isocentric set-up asdescribed by Campana et al [10]. To ensure a goodreproducibility of position, the alignment of the patient isverified by us<strong>in</strong>g laser projections marked on thepatient’s sk<strong>in</strong>. The position of the epoxy breast-supportis also marked on the patient’s sk<strong>in</strong>. Day-to-dayreproducibility is verified us<strong>in</strong>g the distance from thetop of the treated breast to the corner of the epoxybreast-support. Portal imag<strong>in</strong>g controls are regularlyperformed.Methods and materialsFour <strong>women</strong> present<strong>in</strong>g <strong>with</strong> cancer of the left breastand found to have <strong>pectus</strong> <strong>excavatum</strong> were offeredbreast-conserv<strong>in</strong>g treatments at the Institute Curie fromOctober 2002 to September 2004. Surgery consisted ofThe British Journal of Radiology, October 2006 785
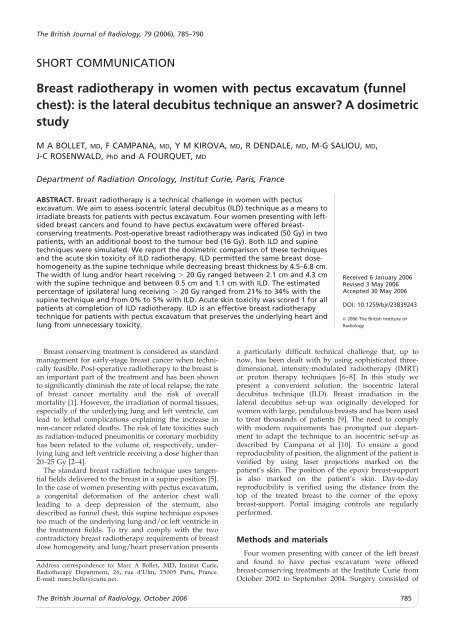
Short communication: ILD breast irradiation – <strong>pectus</strong> <strong>excavatum</strong>(a)(b)Figure 2. Pictures of the same patient <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong> at simulation <strong>in</strong> both (a) the sup<strong>in</strong>e and (b) the lateral decubitusset-ups.target volume <strong>with</strong><strong>in</strong> a range correspond<strong>in</strong>g to 95–107%of the prescription dose. In the case of patient D, the dosecoverage of the breast <strong>with</strong> the sup<strong>in</strong>e technique wasoptimal when only 48 Gy were prescribed at the ICRUpo<strong>in</strong>t <strong>in</strong> 24 fractions.<strong>Breast</strong> thickness ranged between 3.6 cm and 6.4 cm<strong>with</strong> the ILD technique and between 9.4 cm and 12 cm<strong>with</strong> the sup<strong>in</strong>e technique.The <strong>in</strong>ternal tangent fields’ simulation films of bothtechniques are shown <strong>in</strong> Figure 4. An overview of theresults of the dosimetry study is reported <strong>in</strong> Table 1. Thecentral lung distance ranged from 2.6 cm to 4 cm <strong>with</strong>the sup<strong>in</strong>e technique and from 0 cm to 1 cm <strong>with</strong> the ILDtechnique. The estimation of ILV20 ranged from 21% to34% <strong>with</strong> the sup<strong>in</strong>e technique and from 0% to 5% <strong>with</strong>the ILD technique. The maximal heart distance rangedbetween 0 cm and 1.7 cm and the estimation of the HV20from 0% to 9% <strong>with</strong> the sup<strong>in</strong>e technique. They wereboth zero <strong>with</strong> the ILD technique.The maximal width of lung and/or left ventricle thatreceived 20 Gy or more ranged between 2.1 cm and4.3 cm <strong>with</strong> the sup<strong>in</strong>e technique and between 0.5 cmand 1.1 cm <strong>with</strong> the ILD technique.Acute toxicityNo patient needed to have her <strong>radiotherapy</strong> suspended.Acute sk<strong>in</strong> toxicity at the completion of treatment wasmild and scored 1 (RTOG) for all four patients.Discussion<strong>Breast</strong> conserv<strong>in</strong>g treatments for breast cancers cansometimes be denied to <strong>women</strong> <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong>,where <strong>radiotherapy</strong> would <strong>in</strong>volve too high a risk ofpulmonary or cardiac toxicity.As previously discussed, the ILD is a simple, reproduciblebreast irradiation technique that can easily beimplemented <strong>in</strong> <strong>radiotherapy</strong> departments [10]. Morethan 500 patients have already been treated us<strong>in</strong>g thistechnique <strong>in</strong> our centre. Most often, this technique wasdecided on <strong>in</strong> the case of patients <strong>with</strong> large pendulousbreasts who needed breast alone irradiation. In thisstudy, we address the possibility of us<strong>in</strong>g this techniquefor <strong>women</strong> <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong> who need breast-aloneirradiation. We performed dosimetric studies on four<strong>women</strong> and report here the acute toxicity of thistechnique. Because the set-up device we used was toocumbersome to fit <strong>in</strong>to our dosimetric CT-scan, we couldnot perform whole lung and heart scann<strong>in</strong>g and thusdose–volume histogram comparisons were not available.We could nevertheless perform a number of CT slices thataccurately reflected the dosimetry of both the sup<strong>in</strong>e andthe ILD breast <strong>radiotherapy</strong> techniques. In addition, weused the two-dimensional <strong>in</strong>formation available from thesimulation field to estimate the percentage of theipsilateral lung and heart receiv<strong>in</strong>g 20 Gy or more [15].The formula we used was generated by Kong et al fromdata of 40 patients simulated for breast <strong>radiotherapy</strong> (22left side) <strong>in</strong> a sup<strong>in</strong>e position <strong>with</strong> a prescribed dose ofThe British Journal of Radiology, October 2006 787
M A Bollet, F Campana, Y M Kirova et al(a)(b)Figure 3. CT-scan slices at the level of the central axis (z50) of the same patient <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong> taken <strong>in</strong> (a) the sup<strong>in</strong>eand <strong>in</strong> (b) the lateral decubitus set-ups. Dosimetry of whole-breast <strong>radiotherapy</strong> was made for a prescribed dose of 50 Gy at midthicknessus<strong>in</strong>g 4 MV photons.46.8 Gy at the central slice at the mid-bridge for tangents.This formula is to be handled <strong>with</strong> caution when it comesto estimat<strong>in</strong>g the lung and heart volumetric doses <strong>in</strong> ourpatients. First, because we prescribed 50 Gy, i.e. 7% morethan <strong>in</strong> Kong et al series. Second, because this formulawas not meant to be applied to ILD. We assumed that, ifanyth<strong>in</strong>g, the results us<strong>in</strong>g this formula would underestimatethe difference between the sup<strong>in</strong>e and the ILDtechniques <strong>in</strong> terms of volumes of lung and heartreceiv<strong>in</strong>g 20 Gy or more as the craniocaudal lengths ofeither lung or heart <strong>with</strong><strong>in</strong> the simulation field weredim<strong>in</strong>ished <strong>in</strong> the lateral position (data not shown).Pectus <strong>excavatum</strong> is a rare condition and therefore thisstudy suffers from a small number of patients mak<strong>in</strong>g aformal statistical comparison of the two techniques<strong>in</strong>appropriate. We can nevertheless observe that, asexpected, the change of position from the sup<strong>in</strong>e to thelateral decubitus position, <strong>with</strong> the breast spread out on an<strong>in</strong>dividually chosen dedicated breast support, made thethickness of breast smaller by 41–62% and thus also madethe dose <strong>in</strong> depth more homogeneous. The breast took theshape of a parallelogram mak<strong>in</strong>g it easier to obta<strong>in</strong> ahomogeneous dose <strong>with</strong> the use of a s<strong>in</strong>gle wedge(Figure 3b). The most important benefit is that the breastFigure 4. Simulation films of the<strong>in</strong>ternal fields of the four patientspresent<strong>in</strong>g <strong>pectus</strong> <strong>excavatum</strong> both<strong>with</strong> the isocentric lateral decubitus(ILD) and the standard sup<strong>in</strong>e (Sup)<strong>radiotherapy</strong> techniques. Each graduationrepresents a centimetre.Central lung distance (CLD) is theperpendicular distance from thetangential field edge to the posteriorpart of the anterior chest wall atthe centre of the field. Maximalheart distance (MHD) is the maximalwidth of heart <strong>in</strong> the fields.788 The British Journal of Radiology, October 2006
Short communication: ILD breast irradiation – <strong>pectus</strong> <strong>excavatum</strong>Table 1. Dosimetric study compar<strong>in</strong>g the isocentric lateral decubitus (ILD) and the sup<strong>in</strong>e breast <strong>radiotherapy</strong> techniques <strong>in</strong> four<strong>women</strong> present<strong>in</strong>g <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong>. Dosimetries of whole-breast <strong>radiotherapy</strong> were made for a prescribed dose of 50 Gyat mid-thickness us<strong>in</strong>g either 60-Cobalt gammas or 4 MV photonsPatient<strong>Breast</strong> thickness(cm)Central lungdistance (cm)20 Gy ipsilaterallung volume (%)Maximal heartdistance (cm)20 Gy heartvolume (%)Maximal dose tobreast (Gy)Sup<strong>in</strong>e ILD Sup<strong>in</strong>e ILD Sup<strong>in</strong>e ILD Sup<strong>in</strong>e ILD Sup<strong>in</strong>e ILD Sup<strong>in</strong>e ILDA 10.9 6.4 2.6 1.0 21 5 0.0 0.0 0 0 52 52B 12.0 5.2 4.0 0.0 34 0 1.7 0.0 9 0 54 53C 9.4 3.6 3.2 0.0 26 0 0.0 0.0 0 0 53 52D * 11.4 5.6 2.7 0.4 22 0 0.8 0.0 4 0 54 52*For the dosimetry study of this patient, we chose to reduce the prescribed dose to 48 Gy <strong>in</strong> 24 fractions <strong>with</strong> the sup<strong>in</strong>etechnique <strong>in</strong> order to keep the maximum dose below 54 Gy (this patient has however been treated <strong>with</strong> the ILD technique toa total dose of 50 Gy <strong>in</strong> 25 fractions).tissue is located at a greater distance from the chest wall,mak<strong>in</strong>g it easier to encompass the whole breast <strong>with</strong><strong>in</strong> theradiation field <strong>with</strong>out tak<strong>in</strong>g <strong>in</strong> any of the heart and lessthan 1 cm of the underly<strong>in</strong>g lung. The resultant estimatedpercentage of ipsilateral heart and lung are thus reduced toa maximum of 0% and 5%, respectively. In contrast to this,the standard sup<strong>in</strong>e position had central lung depths of atleast 2.5 cm result<strong>in</strong>g <strong>in</strong> the estimated volume of lungreceiv<strong>in</strong>g 20 Gy always be<strong>in</strong>g greater than 20%. Theprotocols <strong>in</strong> use at the Institut Curie def<strong>in</strong>e the maximumdepth of lung and/or left ventricle receiv<strong>in</strong>g greater than20 Gy to be 2 cm, thus the standard sup<strong>in</strong>e techniquewould be unacceptable.IMRT has been proposed as a means to decrease thevolume of the ipsilateral lung receiv<strong>in</strong>g a radiation dosethat is above the tolerance threshold [6, 7]. Fogliata et alhave suggested that three-field conformal <strong>radiotherapy</strong>technique permitted a reduction of the ipsilateral lungvolume receiv<strong>in</strong>g more than 20 Gy from 24% <strong>with</strong> twofieldtangential treatment to less than 20%. This reductionwas the same whether us<strong>in</strong>g IMRT or not [8]. Thedrawback of IMRT and the 3D conformal techniquedescribed by Fogliata et al, contrary to the ILD technique,is that it <strong>in</strong>creases the volume of surround<strong>in</strong>g normaltissues (the heart, sp<strong>in</strong>al cord, and contralateral breast andlung) receiv<strong>in</strong>g low-dose irradiation compared <strong>with</strong> thesup<strong>in</strong>e technique [6]. The other advantage the ILDtechnique has over a three-dimensional <strong>radiotherapy</strong>approach is its cost-effectiveness, both f<strong>in</strong>ancially andtime-wise. However, we have to bear <strong>in</strong> m<strong>in</strong>d that the ILDtechnique is not designed to treat the breast <strong>in</strong> the case of atreatment <strong>with</strong> <strong>radiotherapy</strong> to the lymph node bear<strong>in</strong>gareas; <strong>in</strong> such cases, IMRT <strong>with</strong> or <strong>with</strong>out active breath<strong>in</strong>gcontrol, or even proton therapy [8], could be considered.The acute sk<strong>in</strong> toxicity of the ILD technique was good,<strong>with</strong> no need for a suspension of treatment and only agrade I RTOG sk<strong>in</strong> toxicity <strong>in</strong> all of our four patients ofwhom two were treated <strong>with</strong> a boost of up to 66 Gy.ConclusionsThe ILD technique is an easy, cost-effective means tooffer breast preservation to patients <strong>with</strong> <strong>pectus</strong> <strong>excavatum</strong>,<strong>with</strong>out expos<strong>in</strong>g the underly<strong>in</strong>g heart and, moreparticularly, ipsilateral lung to unnecessary toxicity.AcknowledgmentsWe thank J Y Kristner for design<strong>in</strong>g the treatment setupdevice, Chantal Dauph<strong>in</strong>ot and Yann Brunet for theirhelp <strong>in</strong> the dosimetry study and all the members of theGroupe Se<strong>in</strong> at the Institut Curie for their participation <strong>in</strong>the care of the patients.References1. Clarke M, Coll<strong>in</strong>s R, Darby S, et al. Effects of <strong>radiotherapy</strong>and of differences <strong>in</strong> the extent of surgery for early breastcancer on local recurrence and 15-year survival: an overviewof the randomised trials. Lancet 2005;366:2087–106.2. L<strong>in</strong>d PA, Pagnanelli R, Marks LB, et al. Myocardialperfusion changes <strong>in</strong> patients irradiated for left-sided breastcancer and correlation <strong>with</strong> coronary artery distribution. IntJ Radiat Oncol Biol Phys 2003;55:914–20.3. Graham MV, Purdy JA, Emami B, et al. Cl<strong>in</strong>ical dosevolumehistogram analysis for pneumonitis after 3Dtreatment for non-small cell lung cancer (NSCLC). Int JRadiat Oncol Biol Phys 1999;45:323–9.4. Yu X, Prosnitz RR, Zhou S, et al. Symptomatic cardiacevents follow<strong>in</strong>g radiation therapy for left-sided breastcancer: possible association <strong>with</strong> radiation therapy-<strong>in</strong>ducedchanges <strong>in</strong> regional perfusion. Cl<strong>in</strong> <strong>Breast</strong> Cancer2003;4:193–7.5. Perez CA, Garcia DM, Kuske RR. <strong>Breast</strong>: Stage Tis, T1, andT2 tumors. In: Company JL, editor. Pr<strong>in</strong>ciples and practiceof radiation oncology. Second Edition. Philadelphia: JBLipp<strong>in</strong>cott Company, 1994:877–947.6. Teh BS, Lu HH, Sobremonte S, et al. The potential use of<strong>in</strong>tensity modulated <strong>radiotherapy</strong> (IMRT) <strong>in</strong> <strong>women</strong> <strong>with</strong><strong>pectus</strong> <strong>excavatum</strong> desir<strong>in</strong>g breast-conserv<strong>in</strong>g therapy.<strong>Breast</strong> J 2001;7:233–9.7. Thilmann C, Zabel A, Kuhn S, et al. Inversely planned<strong>in</strong>tensity modulated <strong>radiotherapy</strong> for irradiation of awoman <strong>with</strong> breast cancer and funnel chest. StrahlentherOnkol 2002;178:637–43.8. Fogliata A, Bolsi A, Cozzi L. Critical appraisal of treatmenttechniques based on conventional photon beams, <strong>in</strong>tensitymodulated photon beams and proton beams for therapy of<strong>in</strong>tact breast. Radiother Oncol 2002;62:137–45.9. Fourquet A, Campana F, Rosenwald JC, et al. <strong>Breast</strong>irradiation <strong>in</strong> the lateral decubitus position: technique ofthe Institut Curie. Radiother Oncol 1991;22:261–5.10. Campana F, Kirova YM, Rosenwald JC, et al. <strong>Breast</strong><strong>radiotherapy</strong> <strong>in</strong> the lateral decubitus position: a techniqueto prevent lung and heart irradiation. Int J Radiat Oncol BiolPhys 2005;61:1348–54.The British Journal of Radiology, October 2006 789
M A Bollet, F Campana, Y M Kirova et al11. ICRU. Report 62: Prescrib<strong>in</strong>g, record<strong>in</strong>g, and report<strong>in</strong>gphoton beam therapy (supplement to ICRU Report 50).Bethesda, MD: International Commission on RadiationUnits and Measurements; 1999.12. ICRU. Report 50: Prescrib<strong>in</strong>g, record<strong>in</strong>g, and report<strong>in</strong>gphoton beam therapy. Wash<strong>in</strong>gton DC: InternationalCommission on Radiation Units and Measurements; 1993.13. Bartel<strong>in</strong>k H, Garavaglia G, Johansson KA, et al. Qualityassurance <strong>in</strong> conservative treatment of early breast cancer.Report on a consensus meet<strong>in</strong>g of the EORTC Radiotherapyand <strong>Breast</strong> Cancer Cooperative Groups and the EUSOMA(European Society of Mastology). Radiother Oncol1991;22:323–6.14. Bornste<strong>in</strong> BA, Cheng CW, Rhodes LM, et al. Can simulationmeasurements be used to predict the irradiated lungvolume <strong>in</strong> the tangential fields <strong>in</strong> patients treated for breastcancer? Int J Radiat Oncol Biol Phys 1990;18:181–7.15. Kong FM, Kle<strong>in</strong> EE, Bradley JD, et al. The impact of centrallung distance, maximal heart distance, and radiationtechnique on the volumetric dose of the lung and heartfor <strong>in</strong>tact breast radiation. Int J Radiat Oncol Biol Phys2002;54:963–71.16. Cox JD, Stetz J, Pajak TF. Toxicity criteria of the RadiationTherapy Oncology Group (RTOG) and the EuropeanOrganization for Research and Treatment of Cancer(EORTC). Int J Radiat Oncol Biol Phys 1995;31:1341–6.790 The British Journal of Radiology, October 2006