James M. Dougherty, MD - AkronCantonMDNews
James M. Dougherty, MD - AkronCantonMDNews
James M. Dougherty, MD - AkronCantonMDNews

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Greater Akron/Canton Edition | May-June 2008 VOL. 12, NO. 3www.akroncantonmdnews.comAGMC Offers IGRTSeven Steps toPatient-FriendlyWebsitesSpecial SectionWomen’s Health<strong>James</strong> M. <strong>Dougherty</strong>, <strong>MD</strong>Taking Research from Benchto Bedside at Akron General
R E G E N C Y H O S P I T A L C O M P A N YGiving People Their Lives BackRegency Hospitals are critical care hospitals serving the needs of patients that require acutelevel care for a longer period of time than traditional hospitals are set up to provide. We area national network of hospitals with a different way of thinking, a different way of caring,and a different way of treating, and it shows in everything we do.We have four locations with 140 beds in northeast Ohio to serve the community. FromAkron to Ravenna to the suburbs of Cleveland, we are here to care for your medicallycomplex patients.R E G E N C Y P R O G R A M S A N D S E R V I C E SPulmonary/ventilator programMedically complex/multi-system failure programWound care program (stage III and IV decubitus)Low-tolerance rehabilitation servicesRegency Hospital of Akron155 Fifth Street NE • Barberton, Ohio 44203Main: 330.615.3792 • Referral: 330.615.3800Regency Hospital Cleveland East4200 Interchange Corporate Center Rd. • Warrensville Heights, Ohio 44128Main: 216.910.3800 • Referral: 216.910.3900Regency Hospital of Ravenna6847 North Chestnut Street • Ravenna, Ohio 44266Main: 330.296.2350 • Referral: 330.615.3800Regency Hospital Cleveland West6990 Engle Road • Middleburg Heights, Ohio 44130Main: 440.202.4200 • Referral: 440.202.4300
contents VOL.12, NO. 3MAY-JUNE 2008 44 COVER STORYJAMES DOUGHERTY, <strong>MD</strong>:TAKING RESEARCH FROMBENCH TO BEDSIDEAs hospitals look for innovative ways toutilize their resources to solve complexmedical problems and enhance patientcare, research is becoming an increasinglyimportant focus. Perhaps no one is moreaware of this than Dr. <strong>James</strong> <strong>Dougherty</strong>,chairman of Medical Education andResearch at Akron General.8Seven Steps to aPatient-Friendly Website15 FEATUREWOMEN’S HEALTHAn in-depth look at some of the diseasesand medical issues that affect women.29Keys to BreakthroughPhysician-to-PhysicianRelationshipsDEPARTMENTS26 from the OSMA34 local docs innational news35 hospital roundsON THE COVER<strong>James</strong> M. <strong>Dougherty</strong>, <strong>MD</strong> 15PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTON18 SPECIAL SECTIONWOMEN’S HEALTHAkron General First in Area with Conebeam IGRTCancer treatment is improving—saving lives and extendingsurvival for people with cancer, according tothe National Cancer Institute’s (NCI’s) Cancer TrendsProgress Report released last year. Mitchel Fromm, <strong>MD</strong>,chairman of the Department of Radiation Oncology at24 Akron General HOSPITAL Medical Center, agrees. SPOTLIGHT“We’ve made tremendous advances in radiation therapytreatment planning and delivery. In many situations, theAKRON areas that we treat are very precise. GENERALThere is very littlemargin of normal tissue around the tumors we’re treating,”said Dr. Fromm.In March, Akron General was the first in Summit,FIRST Portage and Stark Counties to IN install Conebeam AREA Image WITHGuided Radiation Therapy (IGRT) technology. ConebeamIGRT technology enables CT images of the tumor remotely to do this.CONEBEAM site and surrounding tissues to be acquired immediately IGRThospital spotlightbefore treatment. These images may then be comparedto the treatment planning CT images, and the patient’sposition matched, so that the actual treatment more preciselyconforms to the treatment plan.“Before patients begin their radiation therapy treatment,they undergo a planning process. This generally includesa treatment-planning CT scan from which we devisea complex, but precise plan,” explained Dr. Fromm.“However, if the position of the patient, or the criticalsensitive structures or tumor target area within the patient,has changed once treatment begins, then you’llmiss part of the tumor target or excessively treat criticalsensitive structures. So treatment may be less effectiveand increase the risk of damaging normal tissues.”Akron General’s IGRT system—the Elekta Synergy—features integrated 3D volume imaging. This allows animage of the tumor site to be acquired and reconstructedimmediately before treatment, with the patient alreadyset up in the treatment position. If the patient needs tobe re-positioned, the treatment table can be controlled“With IGRT, while the patient is in the treatment room,we’re able to image the structures and adjust the patient’sposition—actually move the treatment table—in such away that it will match the treatment plan that we have,”said Dr. Fromm. “Immediately before treatment, we’reactually seeing/imaging the target area and critical structureswith the same imaging modality that was used for245PHOTO COURTESY OF AKRON GENERAL MEDICAL CENTERMitchel Fromm, <strong>MD</strong>, chairman of the Department of Radiation Oncology at Akron General Medical Center, reviews images of a patient’s tumor siteacquired by the hospital’s new IGRT linear accelerator.2 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
coverstory<strong>James</strong> M. <strong>Dougherty</strong>, <strong>MD</strong>Taking Research from Bench to Bedside at Akron GeneralBy Alex StraussAs hospitals look for innovative ways to utilize their resourcesto solve complex medical problems and enhance patient care,research is becoming an increasingly important focus. Perhaps noone is more aware of this than <strong>James</strong> <strong>Dougherty</strong>, <strong>MD</strong>, chairman ofMedical Education and Research at Akron General Medical Center.Having previously served as both a member of the InstitutionalResearch Review Board and director of Emergency Medicineresearch, Dr. <strong>Dougherty</strong> has spent over two decades involved inAkron General’s research efforts.“This hospital has a history of medical education and academics thatgoes back more than 50 years,” said Dr. <strong>Dougherty</strong>. “In a teachingenvironment, a culture of scientific inquiry exists because you alwaysquestion the accepted ways to do things, ‘Is there a better way to do<strong>James</strong> <strong>Dougherty</strong>, <strong>MD</strong>, is chairman of Medical Education and Research and chairman of theResearch Oversight Committee at Akron General Medical Center. He is also a professor ofEmergency Medicine and associate dean of Clinical Education at NEOUCOM.this procedure or treat this condition?’ If you are in an academic center,whether it’s a hospital, university or other teaching environment,you should always be asking questions. Research is just about tryingto answer a question in the most accurate way possible.”Since 2002, Dr. <strong>Dougherty</strong> has been chairman of the ResearchOversight Committee at Akron General. In this role, he is responsiblefor reviewing the hospital’s research protocols and ensuringthe scientific merit and validity of all research being conducted atAkron General.“One of the unique things about conducting research at AkronGeneral is that, because we are a community-based academic hospital,researchers and clinicians are actually able to get together tosolve issues related to patient care,” he said. “Since we are relativelycontained and not sprawling like someinstitutions, those two groups can prettymuch rub shoulders on a day to day basis atAkron General.”PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTONTECHNOLOGYTRANSFER OFFICEAnother example of the unique nature ofresearch opportunities at Akron General isthe newly-developed Technology Transfer,Commercialization and Innovation Office(TTCI Office). Opened just over a yearago, the Office focuses on bringing innovativehealthcare-related ideas and productsto the marketplace and ultimately to thepatient’s bedside. Designed as a gatewayfor entrepreneurial individuals, companiesand organizations to access researchers andother AGMC services, the TTCI Officefacilitates the linkage between the inventorand the clinical and research expertiseof the hospital.“There are people out there that haveideas or they have a prototype of a medicaldevice that may be fantastic, but theydon’t know what the next step is,” saidDr. <strong>Dougherty</strong>. “One of the things thatwe can do is take that idea or product andask our specialists to review it and offer4 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
Through Akron General’s Technology Transfer, Commercialization and Innovation Office, innovative companies and inventors can now accessthe extensive resources of The Kenneth Calhoun Research Laboratory, a 10,000 square-foot facility where basic scientific research andclinical research is conducted.PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTONreal-world feedback as to whether they’re going down the rightpath or whether the product they’re developing may not be thatuseful for patients.”Dr. <strong>Dougherty</strong> explained that the hospital recognized that itsextensive clinical and bench research capabilities coupled with theskill sets and knowledge base of a large medical staff (over a thousandphysicians) could be used to enhance the process of bringing newproducts to the patient’s bedside by establishing strategic partnershipswith select companies or individuals. Through the TTCIOffice, innovative companies and inventors can now access theextensive resources of the Kenneth Calhoun Research Laboratory,a 10,000 square-foot facility where basic science research is conducted.Established in 1987, this laboratory has demonstrated corecompetencies in wound care research, tissue culturing techniquesand the testing of biomaterials including orthopedic fixation devicessuch as surgical screws, pins and stabilization plates.Close collaboration with the Northeastern Ohio Wound CareConsortium for Wound Healing, Research and Education Groupalso allows ideas in wound care to be examined in a multicentermodel involving the other members of this group which includeAkron Children’s Hospital, Summa Health System, Kent StateUniversity, the University of Akron and the Northeastern OhioUniversities Colleges of Medicine and Pharmacy.In addition, the hospital has significant clinical research experiencein the areas of cardiovascular and pulmonary disease,oncology, obstetrics and gynecology, emergency medicine, orthopedicsand, most recently, rehabilitation medicine. Dr. <strong>Dougherty</strong>sees rehabilitation medicine in particular as an up-and-coming areafor research opportunities, for which Akron General can draw uponthe expertise of its affiliated Edwin Shaw Hospital for Rehabilitation.The TTCI Office is currently in discussions with a Finnish companyworking to develop a rehabilitation-related product for lymphedema,a common problem in certain patient populations.PROMISING NEW PROJECTSAccording to Dr. <strong>Dougherty</strong>, research collaboration at AkronGeneral can be as simple as consultation with physician specialistsfor expert feedback on projected clinical applications or as complexas prototype testing or assisting in the development of clinical trialsor sophisticated analytics testing. Close interaction between thebasic science and clinical investigators and the treatment teams allowsfor optimum advancement of new products and enhancementof current ones.“Let’s say someone comes to our TTCI Office and needs to dosome testing to see if a new type of wound covering is effective,”suggested Dr. <strong>Dougherty</strong>, making reference to a recent collaboration.“We can have our researchers in the Calhoun Lab conduct testswith different types of tissue stabilizers or scaffolds while we haveclinicians evaluating the most promising ones in our Wound CareCenter. We can help them find real answers while, at the same time,GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 5
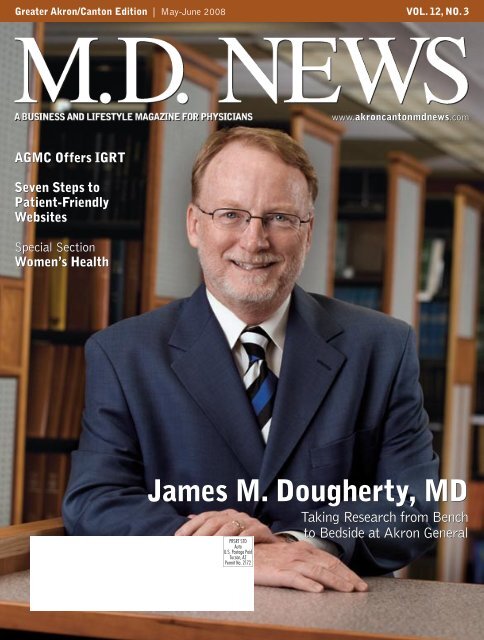
getting a first look at something that couldbenefit our patients and the community.”A recent collaboration through theTechnology Transfer Office involves aninventor who has developed a highly sensitiveimaging technology that may lenditself, among other things, to earlier diagnosisof Alzheimer’s disease. To examinethe possibilities, a research team has beenassembled. It includes an Akron Generalsenior medical staff neurologist withexpertise in Alzheimer’s disease, a professorwith special expertise and interest inneuropharmacology from the College ofPharmacy at NEOUCOM and a specialistin imaging technologies.THE FUTURE OF RESEARCHInterest in product and idea testing at U.S.healthcare facilities is on the rise around theworld, and Akron General hopes to be anarea leader. This fall on October 2, thehospital along with the NEO Wound CareResearch and Education Consortium willsponsor what Dr. <strong>Dougherty</strong> describes asthe first state-wide symposium on woundcare: Heal Ohio 2008, Showcasing Wound CareCompetencies. The goal is to provide a forumin which to present the latest advances inwound management, foster networking andthe sharing of best practices, and facilitatediscussions on regulatory and funding issuesinvolving wound research.“Developing these relationships infusesboth the researchers and their institutionswith enthusiasm and vastly increases thediversity of ideas that can be studied,” saidDr. <strong>Dougherty</strong>.He feels the strategic partnerships madepossible by the Technology Transfer Officeand the hospital’s other efforts can also helpto create a synergy leading to discovery and advancements whichwill continue to improve the lives of patients and the community.Ultimately, successful commercial ventures that result from thesepartnerships will also help to feed new research and bring newbusiness into the area.“It is a cyclical process. Right now, Ohio and, in particular,northeast Ohio are extremely active with various start-up venturesand new ideas and prototypes. By working with some of these companiesand individuals, we see a win-win situation. If they becomesuccessful and we’ve contributed to that success, then we are in aAkron General’s Calhoun Research Laboratory and comprehensive Wound Care Centerprovide ideal testing grounds for new technology. Judith A. Fulton, PhD, coordinator of BasicScience Research, is shown here holding an earlier design of a disposable wound healingdevice she helped test. The device, which delivers concentrated oxygen directly to the wound24 hours per day for up to 15 days, is now being marketed to physicians.position to receive some revenue through business arrangementswith these companies,” said Dr. <strong>Dougherty</strong>.He explained that this revenue can help fund other types ofimportant scientific research that might not get funded otherwise.So it is really a way of moving all of Akron General’s research effortsforward.“By getting a first-hand look at new technologies and linking ourexpertise with the needs of the innovators, we have the opportunityto improve patient care, bring new business into the area, andenhance our academic culture.” ■PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTON6 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
Tort Reform:Where Are We Today?By Barry Riggs, AUSince the advent of tort reform in 2005many have asked the question, “Is it working.”Let’s take a moment and see how this actionhas impacted medical malpractice insurancein Ohio.First and foremost we need to distinguishsome key elements in our current climate.The Tort Reform Act of 2004 limitedthe amount of money a plaintiff canreceive for non-economic damages at$350,000. This by itself has helped stemthe tide of larger awards, but there are otherfactors to consider.There is proportionate liability whichmeans you only pay damages proportionateto your share of the medical negligence.The “deep pocket” is no longer availablein Ohio.The affidavit of merit was not part ofthe tort reform but has had the impact ofreducing claims that are without merit downto a trickle. It states that an expert within thespecialty must attest to the merit of a lawsuitwhen filed. If an affidavit is not produced,the defense counsel may petition the courtto have all defense costs paid by the plaintiff.This has had the desired effect of reducing thenumber of claims filed by upwards of 60 percentover the past year. When you considerthe average claim in Ohio cost $24,443 perclaim in 2005, this is a significant decreasein overall cost.Prejudgment interest reform limitscalculations to the time when a defendant firstreceived notice of a claim and not when theinjury first occurred; prejudgment interestis also now prohibited from being applied tofuture damages.The result has been a reduction of premiumsfor most specialties in Ohio. While notas quick as the medical community wouldhave liked, it has removed the “crisis” labelin our state. Pricing continues to go downslowly and the appetite for business continuesto drive the cost downward throughoutthe specialties. In the past, we have seenmarkets dive too quickly and the result hasbeen a negative impact for the market, afterwhich prices then start to increase. A gradualdecrease will allow the market to continue tostabilize and offset this historical yo-yo cyclewe have seen previously.In the past, market cycles have beendependent on investment strategies andunderwriting profitability. Where in 2003and 2004 the combined ratios of malpracticecompanies were in the 120s we are nowseeing these companies with ratios as lowas 85 percent. This equates to an average 15percent underwriting profit not includinginvestment income. It is clear we are in themidst of a “soft” market, and it would appearthat as long as the combined ratios continue tostay low we can expect further rate decreasesover time.In regard to legislation itself, the SupremeCourt of Ohio has deemed previous tort reformlaws as unconstitutional. No less thanfive times between 1991 and 1999, varioustort reform statutes have been defeatedin court. Our current court however, hasupheld SB 80. On December 27, 2007, inArbino v. Johnson & Johnson, the OhioSupreme Court decided the first set of challengesto this statute. (See slip Opinion No.2007-Ohio-6948, Dec. 27, 2007, availableat http://www.supremecourtofohio.gov/default_highres.asp)While this was not a medical malpracticecase, it has set a precedent wherebythe medical community can take as a positivestep forward that this law has stoodon appeal. At least the current court hasdone something no other has done beforein Ohio.In conclusion, the tort reform act forthe medical community has helped toa significant degree. Prudent underwritingand pricing strategies shouldkeep us heading in the right direction intothe future.Barry Riggs is vice president of Specialty Productsat Sirak-Moore Insurance Agency in Canton. ■There’s a BETTER way to treat chronic wounds....FDAApprovedwith EpiFLO ®EpiFLO ® ....Because it’s allabout gettingBETTERVOLUNTEERS NEEDED! Are you or someone you know suffering fromdiabetic, pressure, or venous stasis ulcers? Ogenix Corporation islooking for volunteers to participate in a 10-week product trial of its FDAapprovedEpiFLO ® If you would like to determine if you or your patientsare eligible to participate in this study, please call 216-378-4281.GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 7
eMarketingSeven Steps to a Patient-Friendly WebsiteBy Collyn FloydWith physicians being urged to provideonline electronic medical records(EMRs) for their patients in the next fewyears, having a website may go from auseful marketing/ information tool to amandated requirement.The push for EMRs on both the state and61 N. Cleveland Massillon Rd, Suite CAkron 330-670-826333 North Ave, Suite 201Tallmadge 330-633-98077981 Hills & Dales Rd.Massillon 330-833-9411federal level, combined with the fact thatmore patients than ever before are onlineand desiring access to online services andcommunication, means that having a patientfriendlywebsite is becoming increasinglyimportant for your medical practice.When patients enter your site, they should3812 W. Tuscarawas St.Canton 330-479-00201220 W. State Rd.Alliance 330-821-4918be able to define two things right off thebat: your website’s purpose and whether ornot your site offers relevant information. Ifwithin a few clicks your site remains cloakedin mystery, it’s a safe assumption that visitorswill leave your site for greener pastures.Following are seven steps to creating a usablewebsite that helps you retain and buildyour patient base:Step 1 – Identify your user. Dependingon the nature of your practice, you mayhave a diverse patient base (i.e., InternalMedicine) or a more specialized one (i.e.,Pediatrics). Ask yourself some questions:Do you care for mostly older patients? Doyou care for minors whose parents wouldbe accessing your website? Do you have alot of new patient referrals to your practice?Your website should be tailored to suityour patients’ age and situation as muchas possible.Step 2 – Identify why users are comingto your site. There are a number ofreasons why a user may be visiting your site;here are just a few:• They’re searching for a new doctor/medicalpractice• They’ve been referred to you and are lookingfor more information• They’re looking up your contact information• They’re looking for medical related information• They’re seeing what services/proceduresyou provide.Make sure your website addresses yourvisitors’ questions. Not only is it a goodmarketing strategy, but it will also cut downon phone calls.Step 3 – Provide content in an easilyaccessible manner. Accessibility includesfeatures like font size options and textdescriptions of images for vision-impairedindividuals. This is especially important inthe medical profession, since you are morelikely to have visitors using assistive technologywhen browsing the internet. You mayremember that the Target stores chain wassued because their website was inaccessibleto people with disabilities.8 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
financial planningHow to DonateMoney EffectivelyBy Paul D. Guerra, AIFWhether it’s the holidays or an unexpecteddisaster, Americans are alwayswilling to donate to those less fortunate.It’s the easiest thing in the world for us toopen our checkbooks to a worthy causewithout a second thought.Yet your donation, regardless of size,should make the largest impact possible onyour cherished causes and issues. Whenyou support a charity’s best interests,you’re not selfish to support your ownas well.Give to efficient operations. Ina perfect world, every cent you donatewould go to fulfilling the mission yousupport. But some portion of every dollargoes to staff salaries, rent, fundraising,mailings, and possibly professional telemarketers.These expenses may leave yourcause with very little.Well-run organizations put most ofyour money toward their services orprograms, not their operational overhead.The American Institute for Philanthropyrecommends that no more than 40 percentof your charitable donation shouldgo to overhead expenses; other charitywatchdogs advise 25 percent. (This maynot apply to newer, smaller, or moreobscure causes.)This percentage can be determinedby requesting a charity’s IRS Form 990,required for a nonprofit to prove itstax-exempt status. Federal law requirescharities to provide the form for the pastthree years to anyone who asks. Divideline 13 (Program Services) by line 17(Total Expenses) to calculate the percentagepaid to services and programs versusoverhead expenses.You can research charities with TheAmerican Institute of Philanthropy’swww.charitywatch.org, the BetterBusiness Bureau Wise Giving Alliance’sgive.org, or Philanthropic Research,Inc’s. www.guidestar.org. All provideinformation on charities andtheir efficiencies.You can also ask for the charity’s annualreports. The report should include themission statement, board of directors, andthe year’s accomplishments and finances.See if the charity’s goals seem reasonableand achievable. If the charity tells youa report isn’t available, is too expensiveto mail, or otherwise discourages yourinterest, don’t contribute.Av o i d t h e s c a m a r t i s t s .Unfortunately, there are people who tryto take advantage of others’ generosity.Here are ways to reduce your chances offalling victim:• If a solicitor mentions previous pledgesyou don’t remember, check your recordsfirst. Don’t fund donations youdidn’t make.• Don’t provide personal financial informationin an e-mail, over the phone,or to door-to-door fundraisers. Use awebsite like www.networkforgood.orgto donate safely with your credit card toover one million organizations. Ignoree-mail solicitations from organizationsyou don’t support.• Never give cash, or make checks out toCash, or to an individual. Write checksout to the charity’s exact name, notinitials. Some scammers use names thatare similar to well-known ones.• Don’t be swayed by on-the-spot highpressuretactics or emotional sad stories.Ask for written information, or checkthe charity out online first.• While many representatives for charitablecauses are genuine, be aware of1 0 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
swindlers who often pretend to representcauses for missing children, soldiersor veterans, firefighters and police, orwhatever disaster is in the news.Know your tax benefits. Yourphilanthropy may provide possible taxadvantages. Tax exempt organizationsare not required to pay taxes. Tax-deductibledonations are those you candeduct from your taxes if you itemize.The IRS has a listing of organizationsto which deductions are tax-deductibleper section 501(c)(3) of the InternalRevenue Code.The IRS now requires actual receiptsfor all tax-deductible contributionsof $250 or more. You should use anindependent appraiser when donatingproperty worth more than $5,000. TheIRS won’t take your or the charity’sword for it. Consult your tax advisor formore help.Reduce your solicitations. Manycharities rent or trade their donorlists to other organizations to raisemuch-needed funds. As a result, youmight get more requests in the mailthe more you donate. The National DoNot Call Registry doesn’t apply to nonprofitorganizations.You can send a letter, along with yourdonations, asking the recipient not rent,sell, or trade your personal information,name, or donation history to anyone. Orask the recipient to limit its solicitations toonly a few times a year. Explain that yourfuture support is contingent on its cooperation.When your charity complies withyour request, consider increasing yourdonations to reward it and to offset anylost revenue from renting your name.If you are receiving unsolicited addresslabels, note cards, pens, pads, orother gifts from charities, you are notfinancial planningobligated to make a donation in return. Tostop receiving these mailings, return thecharity’s envelope with a note requestingthat your name be removed from its list.Be aware, however, that the organizationmight not be able to remove your name ifit rented the list from a list provider.Politely decline in-person solicitationsby saying, “I limit my support to charitiesthat I know well and support the causesthat are most important to me.” Considerconcentrating your support to singularmissions, such as curing cancer; or tohelping institutions in your hometown.Become a stakeholder in the cause yousupport. You deserve to know how yourmoney is used. With a little research, youcan feel confident your donations are beingused wisely to better the world.Paul Guerra is an Accredited InvestmentFiduciary (AIF) and the president of BrookshireFinancial Group, Inc., in Canton. ■GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 11
Solo Practice – Can It Survive?By Diane M. Burge, CPAThe solo practice of medicine in today’s healthcare environment is a challenge. Administrativeburdens are daunting; employees tend to preferworking for larger organizations that offer awider range of fringe benefits and third partypayers basically tell a solo doc to “take it or leaveit” when it comes to contracting.However, as long as there is small independentbusiness in this country, there will be a place forsolo practice. Rural settings are a more conduciveenvironment for going it on your own and mostspecialists have an easier time because of theirhigher revenues. Despite the negatives, if youhave an entrepreneurial spirit and are determinedto be your own boss, here are some things thatcan help you succeed:1. Don’t overstaff. Personnel costs are usually thepractice’s highest budget item. Wasted stafftime is wasted money;2. Get the right-size office and try to sub-let if youcan. The second largest budget item is typicallyfacility. Don’tget more roomthan you needand if you findthere is unusedspace or time,lots ofincomegood doctorpersonallifetry to sub-let or have someone time-sharewith you.3. Organize yourself and get the most out ofevery day. Don’t procrastinate because workdoesn’t disappear if you put off doing it.4. Keep hands-on when it comes to office finances.No-one minds the store better thanthe business owner.5. Manage inventories effectively. Excessivesupplies on hand are dollars spent before theyhave to be. Supplies that are languishing ina room may become obsolete and may alsoconveniently disappear.6.Analyze your practice activities to determineif ineffective services can beeliminated. For instance, many primarycare physicians have hospitalists providingin-patient care to their patients when hospitalwork nets less profit than expandingoffice time.7. Try to hook up with a call group so it’s not always24/7. Keep in mind that you have to make sureyour group colleagues are credentialed with thesame insurance companies if your contractsrequire it.8. Start building up an emergency cash reserveto smooth out the peaks and valleys ofcash flow.9. Decide what your priorities are and committo them.It’s possible to have two out of three,but you can’t have it all. Something is goingto suffer, so don’t convince yourself thatyou’re super-human.Diane Burge is a CPA and principal of Weidrick,Livesay, Mitchell & Burge, LLP, in Bath. ■We Can KeepYour Practice HealthyGrow your business your way with Physician-based accounting.Weidrick, Livesay, Mitchell & Burge’s is staffed with experienced accountingprofessionals with a focus on physician practices. We specialize in physician-basedbusiness accounting to help doctors achieve their potential and remain successful.Controlling overhead, managing collections, personal taxes and retirement planningfor our clients means you are free to concentrate on your specialties...your patients, your practice, your family.Call us today to find out what we can do for you!WEIDRICK, LIVESAY,MITCHELL & BURGE, LLCC E R T I F I E D P U B L I C A C C O U N T A N T S2150 North Cleveland-Massillon Road • Akron, Ohio Akron: 330-659-5985 Medina: 330-722-52491 2 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
Are Your MalpracticeInsurance Limits Burning?By Stephan R. Wright, Esq.legal-easeNearly all medical professionals hopeto have a successful career withoutever needing to look at their medicalmalpractice insurance policy. The onlyinteraction most physicians have withtheir malpractice carrier is makingpayments on those monthly, quarterly,or yearly premiums. However, medicalmalpractice insurance policies are tooimportant to ignore as they provide anexit strategy in defending against malpracticelawsuits, whether frivolous ornot. Despite the importance of medicalmalpractice policies, many medicalprofessionals may not fully understandhow their policies work when a lawsuitis filed.Nearly all professional liability insurancepolicies contain a per claim amountand a separate total aggregate limit. Atypical policy may have coverage of $1million per claim and a $3-million totalaggregate limit. However, what manyprofessionals who are paying for suchcoverage may not appreciate is that these“limits” are often reduced by hard costs,consisting primarily of attorneys’ fees aswell as other costs expended in defendingagainst a lawsuit. Such a policy istypically referred to as a “Claim ExpenseInside” policy, or colloquially referredto as “burning limits,” “diminishinglimits,” or a “cannibal policy.” Underthis type of policy every dollar over thepractitioner’s deductible that is used todefend the lawsuit is applied to the PerClaim Limit. Such a feature in a professionalliability policy is in stark contrastto the typical automobile liability policywhich contains a limit of liability amountregardless of any fees or expenses incurredin defending against a claim.For example, in a typical automobileliability policy, someone who is sued forcausing a rear-end collision is affordedthe total limit of liability insurance (i.e.$100,000 per person/$300,000 per occurrence).If a lawsuit is brought againstthat insured, the insurance company willhire an attorney who will generate fees indefending against the lawsuit. However,if the claim is settled for the full amountof the limits of liability, in our example,$100,000 per person, then the injuredparty will receive the full $100,000regardless of any fees expended in defendingagainst the claim, as the cost ofdefense comes from a separate “pot.”In a professional liability policy withdiminishing limits, a physician with $1million dollars in coverage may quicklyfind him or herself with a significantlylower limit of liability than initiallythought. This is especially true if thematter is tried to a jury and an unfavorablejury verdict is rendered againstIn a professional liability policy with diminishing limits,a physician with $1 million dollars in coverage mayquickly find him or herself with a significantly lowerlimit of liability than initially thought. This is especiallytrue if the matter is tried to a jury and an unfavorablejury verdict is rendered against the physician.the physician. In this type of policy,in an instance where a jury verdict isrendered for $1 million dollars, thepolicy of insurance will not fully coverboth the jury verdict and the cost ofdefense. Stated differently, the totalamount of “exposure” for the insurancecompany in this situation is $1 milliondollars, which includes both any verdictplus the cost of defense (i.e., attorneys’fees, law firm costs, etc.). Thus, ifthe verdict is returned for $1 milliondollars, and the insurance company’shard costs equal $200,000, then theinsurance benefit remaining to pay theverdict is only $800,000, leaving thephysician exposed for the balance ofthe verdict.Although professional liability policieswhich contain “burning limits” arecommonplace, such policies are not necessarilyproblematic for the physician.The important aspect of any professionalliability policy is fully understandingwhat type of policy it is, what the policycovers and what the policy excludes.Professional liability insurance is oftenexpensive and any questions regarding aspecific professional liability insurancepolicy should be directed either to yourinsurance agent or to your legal counsel,who can provide a detailed review ofthe policy.NOTE: This general summary of thelaw should not be used to solve individualproblems since slight changes in the factsituation may require a material variancein the applicable legal advice.Stephan R. Wright (swright@kwgd.com)is a litigation attorney with the law firm ofKrugliak, Wilkins, Griffiths & <strong>Dougherty</strong>Co., LPA ■1 4 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
special section: women’s health GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 15
1 6 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
■GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 17
special section: women’s healthMenopause UpdateBy Barbara Coen, <strong>MD</strong>In 1993, the National Institute ofHealth decided to look for definitiveanswers to what disease processes hormonetherapy might slow or prevent,and if adding progestin to estrogen (toprevent endometrial cancer in womenwith a uterus) would impact the effectsof estrogen on other organ systems.The study was a randomized, controlledstudy known as the Women’s HealthInitiative (WHI). The main thrust ofthe WHI was to determine the exactdegree to which hormone therapiespresumably protected the heart, and toinvestigate the degree to which someof the known and potential risks ofhormone therapies, such as breast cancerand blood clots, cancelled out anybenefits. The WHI also investigatedwhether hormone therapies preventedfractures, colon cancer and dementia,such as Alzheimer’s, as well as the effectsof hormone therapy on quality oflife issues.The combined hormone therapy(CHT) arm of the study was haltedin 2002 after showing an increase inbreast cancer as well as stroke, heartattack and blood clots. The individualrisk of developing breast cancer whileusing CHT was less than one tenth ofone percent per year but was cumulativeover time. The CHT did offer thebenefit of decreasing spine and hipfractures. Although the study foundthat CHT decreased the risk of coloncancer by 37%, the risk of breast cancerand cardiovascular events outweighedthe benefit.The estrogen therapy (ET) arm ofthe study continued for two years afterthe estrogen-progestin arm was halted.The ET arm of the study was haltedin 2004 when researchers discoveredthat ET didn’t prevent cardiovasculardisease and increased the risk of strokeand blood clots at about the same rate asCHT did. On the other hand, ET didn’tappear to increase or decrease the riskof breast cancer during the seven yearsthe women took it.When the results of the WHI werereleased, approximately 65% of womenon hormone therapy stopped their treatment,often at the recommendation oftheir physician. However 1 in 4 womenstarted CHT again due to withdrawalsymptoms such as hot flashes, fatigueand emotional changes.In 20 0 4, the American Collegeof Obstetricians and Gynecologists(ACOG) released a comprehensiveguide of clinical recommendations abouthormone therapy. The guide advises thatCHT should not be used for the preventionof diseases such as cardiovasculardisease. Estrogen alone therapy, usedin women who have had a hysterectomy,should also not be used for theprevention of diseases due to the risksdiscussed above. Hormone therapies areappropriate for the relief of vasomotorsymptoms, provided that the womanhas weighed the risks and benefits withher physician.In patients with vasomotor symptoms,CHT and ET are still the mosteffective therapies, reducing hot flashesby up to 90 percent. For women whowish to avoid or are not candidates forHT, patients should first try lifestylechanges such as wearing layers of lightclothing, setting the thermostat to alower temperature and avoiding spicyfoods and caffeinated beverages andalcohol. The category of antidepressantsknown as SSRIS may also be usedto alleviate hot flashes. Alternativetherapies such as black cohosh, soy,red clover, and wild yam showed noimprovement in vasomotor symptoms.Soy and dietary isof lavones appearto affect estrogen receptors and maynot be safe for women with estrogendependent cancers. Patients shouldalso be advised that these alternativetherapies are not regulated by theF DA a nd shou ld be approachedwith caution.The jury is still out on the effectsof hormone therapies on libido. Thereare too few studies to prove that takingestrogen or testosterone — eitherorally or topically — can improvesex drive. However, there is ampleevidence that estrogen given topicallyor orally can improve the quality of awoman’s sex life by relieving vaginaldryness or related symptoms that makeintercourse uncomfortable.Most menopausal symptoms willresolve within four years of beginningmenopause. Although women shoulduse hormones for the shortest period oftime, about 10% of menopausal womenwill continue to have vasomotor symptomsbeyond the usual four years. Itis inappropriate to withhold HT frompersistently symptomatic women whoprefer to continue HT. Patients andproviders should weigh the risks andbenefits of HT and make decisions on acase-by-case basis.Dr. Barbara Coen is an Obstetrics &Gy n e c olog y s p e c ia l i s t a t W R H HSWomen’s Center. ■1 8 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
A symposiumof distinguishedinvestigators andclinicianspresenting currenttreatments andresearch findingsfor cardiovasculardisease, ACS, Stroke,CHF, arrhythmiaand hypertension.Wednesday,July 30, 2008For registrationinformation, call330-344-6622.P R O U D L YP R E S E N T S20th Annual2008 CardiovascularInvitationalAkron General’s Heart & Vascular Center 20th Annual Cardiovascular Invitationalprovides presentations directed to physicians in Cardiology, CardiothoracicSurgery, Emergency, Interventional Medicine, Family Practice and InternalMedicine along with cardiology allied professionals. In this informal setting,course participants will have ample opportunity to interact with faculty todiscuss current therapeutic issues. This event is held in conjunction with theBridgestone-Firestone Golf Invitational at Firestone Country Club in Akron.TOPICS AND PRESENTERS ARE:“Controversies in Hyperlipidemia Management”– Elliot Davidson, <strong>MD</strong>“What’s New in Peripheral Artery Disease”– Brendan Duffy, <strong>MD</strong>“Risk of Salt in Hypertension: It Doesn’t Only Increase Blood Pressure”– Edward Frohlich, <strong>MD</strong>“Acute Coronary Syndrome – Is there Anything New?”– <strong>James</strong> Hoekstra, <strong>MD</strong>“Future Perspectives in the Management of Heart Failure”- John O’Connell, <strong>MD</strong>“Coronary CT Angiography: Here and Now”– Lawrence Tanenbaum, <strong>MD</strong>“Current Stroke Treatments”– Cathy Sila, <strong>MD</strong>“The Cardiac Surgeon’s View of Atrial Fib Treatment”– John Sirak, <strong>MD</strong>“What’s New in Coronary Intervention”– Steven Yakubov, <strong>MD</strong>“Common Arrhythmias, New Therapies”– Andrea Natale, <strong>MD</strong>Course Director: George I. Litman, <strong>MD</strong>, Director of Cardiology EducationChief Emeritus - Cardiology
special section: women’s healthChronic Pelvic PainBy Bradford W. Fenton, <strong>MD</strong>, PhDChronic pelvic pain is a disabling and distressingcondition which afflicts up to 10%of women. Often women suffer with painfor many months before seeking medicalattention, and finding a multidisciplinarycenter specializing in chronic pelvic paincan be challenging. Unfortunately for physicianstreating these patients, there is rarelya single diagnosis present. Each individualmay have up to five different organ systemsinvolved in pain generation. The diagnosestypically encountered include endometriosisor adenomyosis, interstitial cystitis,myofascial pain syndrome, pelvic floortension myalgia, vulvodynia, and irritablebowel syndrome. Making managementeven more complex, not only do patientshave several different pain generators, theyalso have a significant amount of psychopathologyalong with their pain, which ifnot managed can overwhelm any othertreatment efforts.Although novel therapeutic approachesmay eventually provide new treatments,current management focuses on the accuratediagnosis and management of each paingenerator present in the individual patient.The number of pain generators is variable,and the presence of each depends on theexistence of another. A matrix for determiningthe likelihood of both the numberand nature of secondary pain diagnoses hasbeen published 1 which highlights the needto consider all possible pain generatorswhen managing these patients. The numberof diagnoses is important in predicting thedegree of disability present 2 .The vast majority of chronic pelvic painpatients are female, and many referralcenters are based around gynecologistsand either psychiatrists or other pain managementspecialists. The reasons for thisare multiple, and may also stem from theunderlying connections of the meso-limbictracts in the midbrain, as well as the factthat the uterus is a muscle that contracts ona monthly basis with menstruation. Nodulesof adenomyosis or small fibroids can lead tosecondary dysmenorrhea, and endometriosismay be present as well. Suppression ofovulation represents a mainstay of medicaltherapy, with many options available forwomen who wish to preserve their uterus.Hysterectomy with oophrectomy remainsthe definitive procedure for palliation ofgynecologic pain, but care must be taken toseek out other pain generators, in particularthe bladder.Interstitial cystitis is a poorly understoodsyndrome with pain of bladder origin,and is this area is currently undergoinga renaming process to the more precisedescription of Painful Bladder Syndrome(PBS). Regardless of the nomenclatureused, up to 30% of women with chronicpelvic pain suffer from PBS and hysterectomywill certainly not provide any relief.Making the diagnosis of PBS can be difficult,and the current National Instituteof Health definition is really most usefulfor research purposes. Several of the currentlyused evaluation measures have lessthan perfect diagnostic performance 3 . Evenso, a straightforward diagnostic algorithmhas been described 4 and properly selectedpatients can get significant relief from avariety of measures 5 .Although endometriosis and interstitialcystitis make up the classical “evil twins” ofchronic pelvic pain, many other diagnosesare commonly encountered. Myofascialpain originating in the lower abdomen andpelvic floor tension myalgia (previouslycalled levator ani syndrome) are both verycommon in chronic pelvic pain patients 6 .Management of these muscle pain disorderscan be done medically using anti-inflammatoryor muscle relaxant regimens. Triggerpoint injection can also be done, either withlocal anesthetics, paralytics, or neurolytics.The same approach can also be take for vulvodynia,which has also been termed vulvarvestibulitis and which is most accuratelycalled vestibulodynia, since the conditionis really a perception of pain on light touchof the vaginal vestibule. Another conditioncommonly encountered in chronic pelvicpain patients is irritable bowel syndrome(IBS), for which several subcategories exist.Some of the available medications for IBSshould be used with caution due to seriousside effects.One of the most difficult challengesfacing physicians managing patients withany chronic pain is the problem of narcoticabuse. This comes in many forms, fromaddiction to dependence and can includeselling prescribed narcotics for cash. A recentreview of chronic pelvic pain patients 7conservatively estimated about 13% wereactually seeking narcotics rather than managementof the underlying pain. A knownassociation with a history of previous sexualabuse has consistently been demonstrated,and potentially plays a role in what may bean underlying pain perception disorder.This type of pain is based on the medialpain perception pathway in the brain andhas been dubbed Limbic Associated PelvicPain 8 . Experimental attempts to directlymanage brain pain perception pathways arecurrently underway 9 in research supportedby the Summa Foundation.Dr. Bradford Fenton is Medical Director of thePelvic Pain Specialty Center and a physician withSee Page 222 0 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
special section: women’s healthCervical Length a GoodPredictor of Preterm DeliveryBy Justin Lavin, <strong>MD</strong>Preterm birth, defined as one that occursat less than 37 weeks gestation, is the leadingcause of neonatal mortality and morbidity.While babies born before 32 weeks havethe greatest risk of death and severe illness,those born between 32 and 36 weeks (whichmake up the greatest number of pretermbirths) are still at higher risk for health anddevelopment problems.Now, this risk can be greatly reduced by anew intervention which involves routine measurementof cervical length via transvaginalultrasound during the 20th to 24th weeksof pregnancy. When the cervix is short (15mm or less), progesterone is recommendedto ward off premature birth. In high-riskwomen, a cervical length of 25 mm or lesswould be a warning sign.In Britain, this intervention was foundto significantly reduce preterm delivery,according to a study published in the August2007 issue of the New England Journal ofMedicine. In that study, researchers foundthat progesterone treatment reduced pretermdelivery in women with a short cervix by 34percent, compared with 19 percent of thosetreated with a placebo. Progesterone appearsto slow the shortening of the cervix.In the British study, just 413 women out of24,620 were found to have a cervical lengthof 15 mm or less, which is 1.6 percent of thestudy participants. Although that numbermay seem low, universal screening is stillwarranted. Once a woman goes into pretermlabor, there’s not a lot that can be done totreat it. We may be able to delay delivery for72 hours to give the baby steroids for lungdevelopment, but we’re not very successfulat stopping preterm labor.This is a huge step forward in identifyingand treating women at risk for spontaneouspreterm delivery. Routine screening willresult in lives saved and improved quality oflife for many children who may, otherwise,be born too soon.We know of no other intervention that isanywhere near as effective. If we limit the use ofthis screen to patients with a history of pretermbirths, we will achieve only a small effect on theoverall rate of prematurity because only about10 percent of spontaneous early preterm birthsoccur in women with this history.Cervical length assessment should bestandard for all pregnant women, even thoseexpecting their first child and those with nohistory of preterm delivery. Please get theword out to as many women as possible.Dr. Justin Lavin is a board-certified perinatologistand director of the Division of Maternal/FetalMedicine at Akron Children’s Hospital. ■Continued from Page 20Summa Physicians, Gynecology, ComprehensiveWomen’s Specialty Physicians.References(Endnotes)1The frequency and distribution of multiplediagnoses in chronic pelvic pain related toprevious abuse or drug seeking behavior.Bradford W. Fenton, <strong>MD</strong>, PhD; ChristopherDurner, DO; <strong>James</strong> Fanning, DOGynecol Obstet Invest 2008;65: 247-251.2Symptom severity and disability in chronicpelvic pain worsens when an increasingnumber of pain diagnoses are present.Bradford Fenton, <strong>MD</strong>, PhD; Robert Flora,<strong>MD</strong>; <strong>James</strong> Fanning, DO. Journal of theSociety of Laparoendoscopic Surgeons, 11(2): 2007.3A Novel Measure of Interstitial Cystitis SeverityProvides a Greater Diagnostic Accuracy forthe Evaluation and Management of ChronicPelvic Pain than Previous Methods. Fenton,B.W.; Fanning, J.; Flora, R. J MinimInvasive Gynecol. Volume 14, (6): 46.2007.4Response to hydrodistension for interstitialcystitis defined by a sequential diagnosticalgorithm. Bradford William Fenton <strong>MD</strong>,PhD; Robert Flora, <strong>MD</strong>; <strong>James</strong> Fanning,DO. Obstetrics and Gynecology, 109 (4):24s. 2007.5Hydrodistension for interstitial cystitis consistentlyprovides improvement in properlyselected patients.Bradford W. Fenton, <strong>MD</strong>, PhD, Robert Flora,<strong>MD</strong>, <strong>James</strong> Fanning, DO. Journal of theSociety of Laparoendoscopic Surgeons, 11(2): 2007.6The presence of endometriosis increases therisk for myofascial pain and pelvic floortension myalgia in patients with chronicpelvic pain. Bradford W. Fenton, <strong>MD</strong>,PhD, Thida Nunthirapakorn, <strong>MD</strong>, RobertFlora, <strong>MD</strong>, <strong>James</strong> Fanning, DO. Journal ofthe Society of Laparoendoscopic Surgeons,2008, submitted7The frequency and distribution of multiplediagnoses in chronic pelvic pain related toprevious abuse or drug seeking behavior.Bradford W. Fenton, <strong>MD</strong>, PhD; ChristopherDurner, DO; <strong>James</strong> Fanning, DOGynecol Obstet Invest 2008;65: 247-251.8Limbic associated pelvic pain: A hypothesisto explain the diagnostic relationships andfeatures of patients with chronic pelvic pain.Bradford W. Fenton, M.D., Ph.D. MedicalHypothesis. 2007 Vol. 69 (2) pp 282-286.9 Transcranial direct current stimulation for thetreatment of refractory chronic pelvic pain.Bradford W. Fenton, <strong>MD</strong>, PhD; <strong>James</strong> Fanning,DO; Felipe Fregni, <strong>MD</strong>, PhD. Obstetrics andGynecology, 111: (4s), p82 2 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
Want to increase patient referrals?Gain the attention of 4,000 local physicians through M.D. NEWS!Published every other month, M.D. NEWS offers the opportunity to• Promote your services through display advertising, and• Show your expertise through editorial.Call us today at 330-499-5332 to learn how you can gain theattention (and the patient referrals) you want, or visit our websitewww.akroncantonmdnews.comComing up in the July-August issue of M.D. NEWS:Two Special Sections of ads and articles focused on1. Neurology and neurosurgery--including the diagnosis andtreatment of brain tumors, stroke, TIA, epilepsy, Parkinson’sand other movement disorders, Alzheimer’s, and MS.2. Technology--for diagnosis (MRI, CT, PET, mammography, etc),treatment (lasars, IMRT, IGRT, surgery robots, radiosurgery,etc), and medical records and storage systems (PACS, EMRsystems, etc).If you have expertise in one of these areas, you’ll want to be included.For information, call 330-499-5332 or 1-877-499-5332or e-mail jraabe@mdnews.com
GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 27
CBLH Design“We listen. We plan. We deliver.” That’s the hallmark ofCBLH Design, Inc., an architectural and interior design firmwhich has specialized in healthcare design for the past 37 years.Founded in 1971 by Hal Braun and Don Spice as Braun & Spice,principals Marc Bittinger, Mike Liezert and Tim Hunsickernow compose the leadership of CBLH Design. Today, whilehealthcare is still the focus of more than 60 percent of theirbusiness, CBLH Design also specializes in the architecture,planning and design of universities and libraries.“We have a lot of great longstanding relationships with clientssuch as Louis Stokes Cleveland VA Medical Center, MedinaGeneral Hospital, The Ohio State University Medical Center,Cleveland State University and Akron-Summit County LibrarySystem,” said Liezert. “More recently, we’ve established newrelationships with Mercy Medical Center and NEOUCOM andhave expanded our marketplace into the Akron/Canton areaand other areas of Northeast and Central Ohio in response toour clients’ needs.”In fact, CBLH Design’s business has grown by more than 50percent in the past two years. Hunsicker credits this to the firm’s“very talented, passionate staff of 28 people,” which includesseven registered architects, four staff members in the processof taking the Architect Registration Examination, one boardcertified by the American College of Healthcare Architects,two LEED (Leadership in Energy and Environmental Design)accredited professionals, a full-time interior designer, supporttechnicians and administrative staff.“The principals, along with other members of the CBLHteam, maintain active memberships in respected organizationssuch as The American Institute of Architects, ConstructionSpecifications Institute, Cleveland Green Building Council,American Library Association, Society for College andUniversity Planning and others that provide valuable resourceson a national level,” Bittinger explained. “We have a variety oftalents that blend well into our team concept.”He stressed that their approach to a project is always ateam approach, and not just with the members of his firm,but also with the owners, engineers and contractors. Thegoal is to develop the best solution and physical environmentin which to work. And the best way to do this, according toBittinger, is to listen, plan and deliver.Mercy Medical Center ICU project currently under constructionbusiness profile(Left to right) Marc Bittinger, Mike Liezert and Tim Hunsicker“We really listen to our clients instead of trying to force ourideas on them, and we strive to create designs that maximizereturn on investment,” he said.When planning, the team explores various potentialsolutions, does feasibility studies, prepares site planningoptions, etc. Prior to the bidding process, they advise theowner of the different methods of project delivery that wouldbest suit their needs. After the bidding, they assist the ownerin the evaluation of bids and contractors. Once the projectis underway, they visit the project site on a regular basis andattend job meetings with the owner and contractor.“We make sure the intent of the design documentsis being carried out, and the work being performed bythe contractors is in the best interest of the owner,” saidLiezert.Currently, CBLH is assisting in the implementation of aMaster Plan at Mercy Medical Center which will includea 24-bed ICU with rooftop helipad above a new 100-carparking structure, major renovations and additions to thefirst floor, an expanded Emergency Department (ED) anda 50,000-square-foot buildout of existing shell space foroutpatient services. The firm is also currently designing a120,000-square-foot West Wing addition at Medina GeneralHospital for a new ED, cardiology/nuclear medicine unit,sleep lab and 30-bed patient care unit.“Our success is based on a hands-on approach to designand a personal commitment to service and innovation,” saidLiezert. “This approach not only leads to more effectivedesign concepts, it builds the foundation for strong, longtermrelationships.”CBLH Design is located at 7550 Lucerne Drive, Cleveland, Ohio44130. For more information, visit their website cblhdesign.com orcall 440-243-2000. 2 8 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
Keys to Breakthrough Physician-to-Physician RelationshipsBy Lito RamirezAsk any physician what they expectfrom their personal banker oraccountant, and they will likely saysomething like this: “I want them tosolve my problems, return my phonecalls, and value my business.” Guesswhat? Other physicians expect thisfrom you, too, but chances are, you’renot delivering.Too many physician practices arewoefully ill equipped to provide eventhe most basic level of client servicethat we regularly demand from nonhealthcare service providers. Whocan blame them? MBA-level courseswere never part of the med school curriculum.But in ignoring these clientservice fundamentals, many specialistsrisk leaving thousands of dollarson the table in unrealized income andlost revenue.Client service, especially exceptionalclient service, builds positivereputation and long-term relationshipsthat lead to increased market shareand revenue growth. Your banker,accountant and lawyer all understandthis. You should, too. Below are sixclient service keys that will help buildstronger physician-to-physician (p2p)relationships that achieve breakthroughgrowth.Relationships are everything.Remember this: getting patients isa relationship business. Treatmentsand services are commonly viewed ascommodities that any board certifiedspecialist can provide. Relationships,however, carry an intangible value thatyou can’t put a price on. Positive relationshipsbuild trust and reinforce thephysician’s decision to send patientsto you for care. As much as you thinkso, you’re not the only game in town.So guard your physician relationshipsor those patients (and revenue) willhead out your door to the specialistup the street.Be accessible. Lack of accessibilityis a top complaint about specialists.Make sure you give physicians acomplete list of all your contact information,including direct line and cellphone, and set the expectation up fronton when their calls will be returned;60- to 90-minutes is reasonable. Alsogive physicians your home telephonenumber. Many will bristle at this suggestion,but a respectable physicianwon’t take this unlimited access lightlyand will view it as a sign of your trust.It’s doubtful the privilege will everbe used, but the payoff is tremendousbecause it reinforces the valueof the relationship.See patients promptly. It’s aggravatingwhen a physician refers a patientfor care only to find the specialistcan’t see the patient for another threemonths. This delays care of the patient,which could result in the physiciansending his patient elsewhere. Beflexible by seeing another physician’spatients as soon as possible.Keep them involved. Nothingdraws a physician’s ire faster than thespecialist who moves ahead with treatingthe patient without first touchingbase; ditto for the specialist whoseeks a consult with another specialistwithout consulting the patient’soriginal physician. Always make surethe original physician is up-to-date andmeaningfully involved.Always communicate. Lack ofprompt communication also rankshigh on the list of all time gripesabout specialists. A physician shouldnever have to call your practice toask the status of their patient. Makesure to call the original physiciandirectly to keep them updated; thenfollow-up in writing.Send the patient back. I was aconsultant to a medical center thatlocal physicians termed the ‘blackhole’ because they would refer patientsthere for care but would never seethem again. When you don’t return apatient to the original physician, youare effectively stealing that patient.Word will then spread quickly aroundthe medical staff lounges that you’rea poacher. You may have gained onepatient, but forget access to future patientsand revenue when the physiciansends his patients elsewhere.In today’s highly competitive marketplace,specialists must recognizethat physicians have more choices thanever in where they send patients forspecialty care. Building relationshipsrequires patience and persistence. Butthese client service keys will help buildstronger, more positive and loyal p2prelationships that keep your patientpipeline filled in the future.Lito Ramirez is principal of gravit|eSMP, a strategic health care consultancybased in Columbus OH whichhelps physician practices and hospitalsincrease and manage revenue from theirphysician relationships. ■Copyright 2008 by gravit|e SMP, LLC. All rightsreserved. Reprinted with permission.GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 29
Federal Government Gets Failing Gradeson Tobacco Control from ALAThe American Lung Association’s State ofTobacco Control 2007 report, an annual reportcard on federal and state tobacco controllegislation and policies, assigns only Ds andFs to the federal government, but says 2008presents an historic opportunity for Congressto make a dramatic impact on tobacco controlacross America by authorizing the U.S. Foodand Drug Administration (FDA) to regulatetobacco products. Strong, bipartisan legislationis pending in both the U.S. Senate and U.S.House of Representatives that would give theFDA authority over the manufacture, distribution,marketing and use of tobacco products.The report can be accessed online at www.stateoftobaccocontrol.org.“The Congress has an unprecedentedopportunity in 2008 to pass this life-savinglegislation,” said Bernadette Toomey, Presidentand CEO of the American Lung Association.Tobacco-related diseases remain the No. 1preventable cause of death in America, killingmore than 438,000 Americans each year.The American Lung Association’s State ofTobacco Control 2007 report tracks progressmade, ground lost, and issues that havestalled throughout 2007, during which timetwo major public health reports — from thePresident’s Cancer Panel and the Institute ofMedicine — heralded the need for the federaland state governments to take urgent actionto reduce America’s tobacco epidemic. TheLung Association’s report card grades eachof the 50 states, the District of Columbia andPuerto Rico on their tobacco control policiesin smokefree air, cigarette tax, tobacco preventionspending, and youth access to tobaccoproducts. The report grades federal tobaccocontrol efforts on cigarette tax, giving theFDA authority over manufactured tobaccoproducts, cessation and ratification of theinternational tobacco control treaty.Grades for federal issues — FDA regulationof tobacco products, cigarette tax, cessationpolicies, and the international tobacco controltreaty — still score only Ds and Fs. Congress,however, is poised to pass the Family SmokingPrevention and Tobacco Control Act to givethe Food and Drug Administration oversightover tobacco products, legislation that will3 0 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008curb the marketing of cigarettes to childrenand teens.“Now is the time for leaders at the federal,state and local levels to summon the politicalwill to do what’s right and finally shut the dooron this country’s tobacco epidemic,” said Ms.Toomey. “There’s no excuse for America notto make major progress on this vital issue,because we know what changes need to bemade to protect health and save lives. Halfheartedresponses and weak policies from alllevels of government will not put an end tothe tragedy of tobacco addiction, disease anddeath in America.”In the United States, the FrameworkConvention on Tobacco Control, the world’sfirst tobacco control treaty, again saw no actionin 2007. As of December 2007, 151 nations,not including the U.S., have ratified the treaty,yet the document has languished since 2004 in“interagency review.”Twenty-one states, the District of Columbiaand Puerto Rico have answered the AmericanLung Association’s Smokefree Air 2010Challenge by passing comprehensive smokefreeair laws that protect almost all workers fromexposure to secondhand smoke. However, 18states continue to receive an F in this category,leaving millions of Americans exposed topotentially lethal secondhand smoke in restaurants,workplaces, and other public places.The Smokefree Air 2010 Challenge calls forall 50 states, the District of Columbia andPuerto Rico to be 100 percent smokefree nolater than 2010.Despite repeated studies proving that wellfundedstate tobacco prevention and cessationprograms keep youth from starting to smokeand motivate smokers to quit, only six statesfund these programs at the levels recommendedby the Centers for Disease Controland Prevention (CDC). Nine states scored anA for funding their programs at 90 percent ormore of the CDC’s minimum recommendedfunding level. Thirty-two states, the Districtof Columbia and Puerto Rico received an F fortobacco prevention and control funding.Raising cigarette taxes have motivatedthousands of Americans to quit smoking andprevented thousands of kids from starting.national newsTwenty-five states, the District of Columbia,and Puerto Rico have cigarette tax rates of $1or higher, and nine states will be at or above$2.00 per pack. Currently, the average statecigarette tax is $1.11 per pack, an increase ofabout 11 cents from last year. New Jersey leadsthe country with the highest cigarette tax at$2.575 per pack. Twelve states received anF in cigarette taxes in 2007, down from lastyear’s 13 Fs.“As coalitions all across America fight toothand nail to tighten laws to protect youth, inparticular, tobacco companies are launchingnew products clearly targeted toward younggirls and teens, selling candy-flavored cigarettes,and promoting buy-one-get-one freedeals that undermine states’ efforts to increasethe cost of cigarettes by raising cigarette taxes,”Ms. Toomey explained.Data released in 2007 detailed the tobaccoindustry’s spending, including approximately$36 million a day ($13.1 billion annually)in marketing, in addition to $1.7 million indirect contributions to federal candidates and$96 million supplied to state-level candidates,committees and ballot measure campaignsduring the 2005 and 2006 election cycle.Despite signing a settlement agreement withstate Attorneys General in October 2006prohibiting the marketing of candy, fruit,and alcohol-flavored cigarettes, RJ Reynoldsviolated the spirit of the agreement by introducinga new line of flavored cigarettes barelyseven months later; survey data has shownthat these products are favored by smokersaged 17 to 19.“The tobacco companies aren’t letting up,but we’re not letting up either,” Ms. Toomeysaid. “The American Lung Association willcontinue to fight to save lives by reducing theterrible burden caused by tobacco.”The American Lung Association has helpedmillions of Americans quit smoking throughour Lung HelpLine (1-800-LUNG-USA),and through our smoking cessation programs,including Freedom From Smoking, consideredto be the “gold standard” of group-setting,smoking cessation programs and Not onTobacco, or N-O-T, a nationally recognizedsmoking cessation program for youth. ■
WORKING TO DEVELOPA GENE REPLACEMENTTHERAPY FOR PREMATUREOVARIAN FAILUREThe gene mutation believed to be a possiblecause of premature ovarian failuremay be corrected when an adenoviruscompensating for the mutated gene isintroduced, discovered a team of researchersfrom the Meharry Center for Women’sHealth Research, the University of TexasMedical Branch and the University ofSaskatchewan. Findings were reportedin the recent issue of Molecular HumanReproduction.Premature ovarian failure affects 1% ofwomen worldwide and occurs in youngwomen between the ages of 15 and 25.When a woman has premature ovarianfailure, her ovaries stop producing eggsand estrogen resulting in infertility andearly menopause.Dr. Ayman Al-Hendy, who is also a professorand Vice Chair of the Departmentof Obstetrics and Gynecology at MeharryMedical College, said, “The objective ofour study is to develop a gene therapy approachfor the treatment of this type ofinfertility. This is the first published worksince the discovery of the Finnish C566Tmutation that examines what happens atthe cellular level when an adenovirus expressingthe normal gene is introduced inthe presence of the gene mutation.”Dr. Al-Hendy said he and his team areencouraged by the findings and hope thatfuture studies will show that once themutation is corrected with the replacementof a healthy gene, the ovaries canbe restored to normal functioning levelsincluding ovulation and the productionof estrogen.First discovered in 1995, the gene mutationknown as the C566T blocks thenormal function of the follicle stimulatinghormone receptor and prevents thenormal development of ovarian folliclesand eggs in females. Women who havecurrent topicspremature ovarian failure usually cannotbecome pregnant with their ownbiological children. They often receivehormone replacement therapy to alleviatemenopausal symptoms.“You can imagine how devastating thiscondition is for the young woman whohas it. While a cure or treatment optionis several years away, findings like the onein our study are encouraging and promising,”said Dr. Al-Hendy.More research is still needed and workis currently underway to confirm the invitro data in appropriate animal modelsbefore clinical trials in women begin. ■Reference:Meharry Medical College.Ghadami M, Salama SA, Khatoon N, ChilversR, Nagamani M, Chedrese PJ, Al-HendyA. Toward gene therapy of primary ovarianfailure: Adenovirus expressing human FSHreceptor corrects the Finnish C566T mutation.Mol Hum Reprod 2008 Jan;14(1):9-15.Summa’s GeriatricFellowship Program AccreditedSumma Health System’s GeriatricMedicine Fellowship program receivedaccreditation from the AmericanCollege of Graduate Medical Education(ACGME). The fellowship program,which begins this year in July, will traindoctors to become leaders in the fieldof geriatrics through one year of clinicaltraining and specialized educationfocused specifically on the medical careof older adults.Medical students studying to becomegeriatricians must first complete aresidency program in either InternalMedicine or Family Practice. Fellowshiptraining is advanced training beyondresidency training in a concentrated areaof patient care.During each rotation, two fellows willhave the opportunity to use the AcuteCare for Elders (ACE) unit, the Centerfor Senior Health, gero-psychiatricunit, and other clinical programs as the“teaching classroom” sites.At the same time the “baby boomer”generation is aging, the country isfacing a shortage of geriatricians. In2005, there was only one geriatricianfor every 5,000 Americans 65and older. The American GeriatricsSociety (AGS) estimates that at least36,000 geriatricians will be needed inthe next 20 years.In addition to the Geriatric MedicineFellowsh ip, Summa also offers aPalliative Care Fellowship program,which includes extensive trainingin both hospice and palliative medicine.T he palliative care fellowswork closely with Summa’s geriatricians,advanced practice nursesand social workers enabling them tounderstand the aging process, complexityof illnesses and the importance ofcoordinated care. ■GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 31
Happy 5th Birthday, HIPAA!By Joseph J. FeltesThis year marks the 5th anniversary ofHIPAA’s Privacy Rule, which went intoeffect on April 14, 2003. It seems likeonly yesterday that physician practicesWHAT GOODIS WEA LTH ifyou don’t havetime to enjoy it?were counting the days toward the biggestdoomsday scare since Y-2-K. (Now, if youbelieve public service announcements bombardingthe airways, the next doomsday onIt’s ironic. While money is often associated with freedom, the more wealth youhave, the more time you need to manage it. At the Private Client Group, wehelp you optimize and preserve wealth so you can fully experience itsadvantages. With exceptional proprietary research, local portfolio managers andexternal money managers, we can identify customized long-term opportunitiesfor you. The result: you have more of two important assets – time and wealth.To experience the Private Client Group, call Michele Pfund, Client Advisor,at 330.375.8034.WEALTH PLANNING l PRIVATE BANKINGINVESTMENTS l TRUST & ESTATE ADMINISTRATIONManaging wealth for over 160 yearsNationalCity.com/wealth©2007, National City Corporation®CS-28817the horizon is February 2009, when theswitch from analogue to digital tv broadcastswill occur, which I doubt qualifies asthe “big one.”)I am happy to report that, after 5 years,no physician has been killed or seriouslyinjured because of HIPAA.Not that there haven’t been casualtiescaused by this product of the (first?)Clinton administration. Recently, severalUCLA Medical Center employees werefired for improperly accessing confidentialmedical records in two separate incidents:one involving role model BritneySpears and the other involving fallen angelFarrah Fawcett.Independent frolics by curious employees,who cannot suppress the urge to snoop,is not confined to the medical records of therich and famous. Hospitals and physicianpractices have had to discipline employeeswho improperly accessed paper and electronicmedical records.The healthcare industry has done a goodjob over the past 5 years safeguarding theconfidentiality of patient medical information.Self-policing may account, in part, forwhy there have been relatively few complaintsof HIPAA violations to the Officefor Civil Rights of DHHS which, along withthe Department of Justice, are charged withenforcing HIPAA’s Privacy Rule.The OCR reports that it has received atotal of 33,277 complaints from April 14,2003 to January 31, 2008. Of those, mostwere dismissed without investigation.Only 8,405 complaints were investigated,of which 5,653 led to corrective action.When we consider the millions of medicalrecords created, used, and disclosedover the past 5 years, this number isstatistically infinitesimal.The only criminal verdict recorded overthe 5 years in which HIPAA has been inexistence came in January 2007. A former3 2 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
Florida Cleveland Clinic employee wasindicted ( the Clinic was not indicted) whoimproperly downloaded medical records of1,100 patients, which she sold to her cousin,who owned a medical claims business. Thecousin used the stolen information to submit$7 million in fraudulent claims (like,that was going to work).Does that mean that HIPAA’s PrivacyRule has been a failure, or that it has notimpacted the health care industry — fromlarge systems to sole practitioners? On thecontrary, HIPAA has raised the conscientiousnessof those who handle patientinformation. Virtually every day, HIPAA’sPrivacy Rule is invoked by hospitals andphysician offices.Most of the time, those relying onHIPAA get it right, when, for example,they require signed Authorizationsbefore releasing records for purposesother than treatment or payment ofclaims. But, there are times, when peoplestill cite HIPAA incorrectly, whether outof confusion, or because saying “HIPAAdoesn’t allow t his” convenientlyexcuses performance.It’s time for physician practices to conducta HIPAA refresher. We can start witha relatively simply prescription: “HIPAA’sPrivacy Rule applies to the Use andDisclosure of Protected Health Informationby Covered Entities.”“Covered Entities” include health careproviders and payers. “Protected HealthInformation” (PHI) means informationabout a patient’s medical condition, treatmentof that condition, and payment oftreatment for that condition. “Use” meansinternal sharing of “PHI” within the physician’soffice or hospital. “Disclosure” meansrelease of “PHI” to a third party. Physicians,as “Covered Entities,” may “Use” and“Disclose” patient “PHI” to other CoveredEntities,” without a patient’s Authorization,for treatment or payment purposes.Physician offices must get a signed patientAuthorization if “PHI” is “Disclosed”to a non-covered entity (e.g., patient’semployer or life insurance company), orif the intended “Use” or “Disclosure” is forpurposes other than treatment and payment.A simple mantra office personnel canrecite, which can guide them through mostHIPAA situations, is: “Who is getting this“PHI” and why?” It is a matter of commonsense and the “Golden Rule.”Now is also an appropriate time for physiciansto review their offices’ Notice ofPrivacy Practices, which HIPAA requiresmust be given to patients, so they may understandwhat safeguards a practice employswhen “Using” or “Disclosing” “PHI.” DoNotices of Privacy Practices accurately describewhat, in reality, is being done? Havethere been changes over the past five years,such as the creation of a practice website,the use of e-mail to communicate with patients,or other means to contact patients?If so, the Notice of Privacy Practice needto be amended.This brief retrospective of HIPAA’sPrivacy Rule provides us with the opportunityto prognosticate what its impactmight be in the next five years. Regardlessof who occupies the White House after thenext presidential election, the chances aregood that HIPAA, bolstered by the public’sconcern for safeguarding privacy, may playa more prominent role.Joe Feltes is an attorney with Buckingham,Doolittle & Burroughs, LLP in Akronand Canton. ■GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 33
Local Docs in National NewsPaul William Jones,DO, MHA, FAOCAPaul WilliamJone s , DO,MHA, FAOCAw a s e l e c t e dP resident ofThe AmericanO s t e o p a t h i cC o l l e g e o fAnesthesiologistsfor 2007-2008.Dr. Jones received his medical degree fromThe University of New England College ofOsteopathic Medicine in Maine and was conferredthe Degree of Fellow by The AmericanOsteopathic College of Anesthesiologistsin 2000. Dr. Jones is the chairman of theDepartment of Anesthesiology and directorof Anesthesia Services at RobinsonMemorial Hospital.N i h a dB o u t r o s ,<strong>MD</strong>, receiveda PresidentialCitation fromthe Society ofCritical CareM e d i c i n eNihad Boutros, <strong>MD</strong> (SCCM) at the20 08 AnnualCritical Care Conference. The PresidentialCitation was created to honor memberswho have contributed to the SCCM in avery meaningful way. Dr. Boutros wasnominated for supporting the developmentefforts of SCCM’s Membership Committeethrough service as voluntary membershipliaisons. Dr. Boutros is an intensivist atAultman Hospital. He is board certified inInternal Medicine, Pulmonary Diseases,Critical Care and Sleep Medicine.Murli Manohar, <strong>MD</strong>, MPH, PhD,was recently honored by American MedicalAssociation Foundation with its prestigiousPride in the Profession Award. The awardwas given in recognition of his dedication tothe practice of medicine, devotion to healthcareadvocacy and passion for communityservice. Dr. Manohar is a solo practitionerand co-founder of the Canton CommunityClinic, a free clinic for the uninsured. Hehelped develop legislation in Ohio that givesmalpractice immunity to physicians workingin free clinics. He was also instrumentalin creating the Ohio legislation that allowspeople to donate unused, unexpired medicationsin their original sealed packages to Ohiofree clinics. Dr. Manohar was appointed tothe Ohio State Commission on MinorityHealth, shaping many laws and ideas.PUBLICATIONS ANDPRESENTATIONSFosnight, S, Zafirau, W, Hazelett,S. Vitamin D Supplementation to PreventFalls in the Elderly: Evidence and PracticalConsiderations. Pharmacotherapy. 200828(2):225-234.Hall BJ, Hobfoll SE, Palmieri PA,Canetti-Nisim D, Shapira O, JohnsonRJ, Galea S. The psychological impact ofimpending forced settler disengagement inGaza: Trauma and posttraumatic growth. JTrauma Stress. 2008 Feb;21(1):22-9.Hobfoll SE, Canetti-Nisim D,Johnson RJ, Palmieri PA, Varley JD,Galea S.The association of exposure, risk,and resiliency factors with PTSD amongJews and Arabs exposed to repeated acts ofterrorism in Israel. J Trauma Stress. 2008Feb;21(1):9-21.Kovacik MW, Gradisar IA, TokashJC, Stojilovic N, Ehrman JD, BenderET, Ramsier RD. An introduction ofvarious spectroscopic methods to identifyin vivo metal wear in total knee arthroplasty.J Biomed Mater Res A. 2008 Mar15;84(4):1068-77.Allen K. The Steps Care Study:Strategies to Enhance Post Stroke Careand Recovery. Presented at: InternationalStroke Conference; February 20, 2008.New Orleans, LA.Engel J, Pethtel L, Zarconi J,Missimi S, Hines R. Narrative HealthCare in Family Medicine. Presented atAmerican Association of Medical CollegesConference, November 2-7, 2007.Washington DC.Mason H, Radwany S, Clarke S.“How to Get to 110 Consults a Month inLess Than 5 Years: Growth of a PalliativeCare Consult Service in a CommunityTeaching Hospital.” Presented at the AnnualAssembly of the American Academy ofHospice and Palliative Medicine, January30-February 2, 2008. Tampa, FL.Ng S, Davies D, Cevasco D,Radwany S. The man who refused todie: the challenges of protracted imminentdying. Presented at the Annual Assemblyof the American Academy of Hospice andPalliative Medicine, January 30-February2, 2008. Tampa, FL.Radwany S, Albanese T, SchraderJ. “Sources of Cost Savings on an AcutePalliative Care Unit as Compared to OtherHospital Inpatient Units.” Presented at theAnnual Assembly of the American Academyof Hospice and Palliative Medicine, January30-February 2, 2008. Tampa, FL.Radwany S, Albanese T, CloughL, Sims L, Richmond J, Ng S. “AConceptual Framework for ConductingFamily Meetings in an Intensive CareUnit.” Presented at the Annual Assemblyof the American Academy of Hospice andPalliative Medicine, January 30-February2, 2008. Tampa, FL.Schaaf, A., Weiner, D., Morscher,M., Dicintio, M. Fracture IncidenceFollowing Plate Removal in Legg-Calve-Perthes Disease - A 30 Year Study. Presentedat American Academy of OrthopaedicSurgeons Annual Meeting, March 5-9,2008. San Francisco, CA. ■3 4 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
hospital roundsWhat’s New at Area HospitalsAffinity Medical Center’s Wound Healing Center wasrecently recognized at the Annual National Healing Corporation(NHC) meeting for its outstanding outcomes in 2007. Affinity’soutcomes include averaging a 91 percent healing rate in 16 weeks orless for wounds during 2007. The NHC average across the countryfor the same time period was 89 percent. In addition, overall NHChealed 85 percent of all wounds in 2007, while Affinity healed 87.52percent. NHC manages over 130 centers located in 31 states.Akron Children’s Hospital and Humility of Mary HealthPartners (HMHP) have expanded their pediatric services in theMahoning Valley by developing a pediatric center for the treatmentof blood diseases and cancer. The new center features an outpatientfacility with five treatment rooms and three clinical exam rooms,and is equipped to perform outpatient chemotherapy, blood infusionsand other treatments. In addition, the center providesemotional support for the child, as well as the entire family. Thecenter is located at St. Elizabeth Health Center at 1044 BelmontAve. in Youngstown.Akron General Medical Center has opened a dedicatedclinic for the chronic medical needs of a growing population ofpatients who suffer from pulmonary hypertension, a conditionmarked by continuous high blood pressure in the pulmonary artery.The Pulmonary Hypertension Clinic at Akron General bringstogether physicians, nurses and technologists who are experiencedin diagnosing and treating this complex condition. The Clinic hasa number of specialized protocols aimed at keeping patients out ofthe hospital.Alliance Community Hospital recently entered a partnershipwith Wound Care AdvantageTM to establish an on-site outpatientwound care clinic that is owned, operated and staffed by the Hospitaland supported by WCA. The ACH Wound Care Advantage, whichopened in May, treats chronic non-healing wounds, includingthose resulting from infection, diabetes, arterial or venous disease,radiation or surgery, through a multidisciplinary approach whichincludes hyperbaric oxygen therapy (HBOT). Wound Care is justone area of growth and expansion planned for the Hospital in thecoming year.Aultman Hospital’s Cardiovascular Surgical Intensive CareUnit (CVSICU) and Medical Intensive Care Unit (MICU) receivedthe 2007-2008 Beacon Award (fall and spring, respectively) forexcellence in intensive care nursing. The award was presentedby the American Association of Critical-Care Nurses to nursingunits that met rigid criteria for excellence, exhibited high-qualitystandards and provided exceptional care for patients and families.Additionally, the Aultman Breast Care Center recently earnedthe American College of Radiology’s “Breast Imaging Center ofExcellence” designation.Barberton Citizens Hospital has earned Quality RespiratoryCare Recognition (QRCR) under a national program aimed at helpingpatients and families make informed decisions about the qualityof the respiratory care services available in hospitals. The QRCRprogram was started by the American Association for RespiratoryCare (AARC) in 2003 to help consumers identify those facilitiesusing qualified respiratory therapists to provide respiratory care.Hospitals earning the QRCR designation ensure patient safety byagreeing to adhere to a strict set of criteria governing their respiratorycare services.Cuyahoga Falls General Hospital has developed a newprogram to both screen and educate patients about Deep VeinThrombosis (DVT) in an effort to reduce DVT occurrences in patients.CFGH physicians, nurses and staff have undergone extensiveeducation regarding DVT. As a result, each patient that is admittedto the hospital is now screened for their risk of developing DVT andreceives a pamphlet about the warning signs and symptoms.Medina General Hospital has opened an Imaging Center onits Brunswick Campus on Center Road. The new center offers OpenMRI, CT, ultrasound, mammography, bone density scanning andgeneral X-ray services. All equipment is completely digital whichSIMPLIFY YOUR FINANCIAL LIFEBrookshireF i n a n c i a l G r o u p , I n c .Lifetime Wealth Strategies and SolutionsThere are hundreds of aspects to managing yourfinancial life. By partnering with a wealthmanagement expert, you can:Create a customized planPursue your financial goalsFind financial confidenceContact us today at 330.453.3991to learn how we can help you simplifythe complexities of your financial life andmanage your wealth for the long term.THE MILLENIUM CENTRE 200 MARKET AVENUE NORTH CANTON, OH 44702info@brookshirefinancial.com www.brookshirefinancial.comBrookshire Financial Group, Inc., is a Registered Investment Adviser.Securities offered through Commonwealth Financial Network, ® Member FINRA/SIPC.GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008 | 35
hospital roundsreportedly gives the radiologist a closer and more precise viewfrom which to make a diagnosis. Digital files can also be transferredquickly from the Imaging Center to the referring physician within24 hours. General X-ray is offered on a walk-in basis. For otherimaging services, same-day or next day appointments are availablepending pre-certification.Mercy Medical Center will open a new health center inTuscarawas County at the Lewis Center Regional Medical Parkin New Philadelphia. Mercy will be joined by Akron Children’sHospital in the new facility, which is a project of developer DanaLewis, through his Investment Realty Properties Ltd. of NewPhiladelphia. Mercy anticipates opening its health center this fall,offering radiology and lab services, and a STATCARE immediatecare center for treatment of minor illnesses and injuries. MercyHealth Center of Tuscarawas County will be open extended hoursto meet the needs of the community.Robinson Memorial Hospital (RMH) was re-verified asa Level III Trauma Center after a site visit from the AmericanCollege of Surgeons in December. Level III verification indicatesthat certain personnel and systems are in place to provide optimumemergency care for patients with life-threatening injuries. Physiciansand staff at level III centers coordinate care delivery and facilitatepatient transfers when necessary. EMS squads notify the hospitalwhen a patient with life-threatening injuries is on the way, and atrauma team of physicians, nurses, surgeons, technicians, anesthesiologistsand respiratory therapists is usually ready before theambulance arrives.Summa Health System’s Center for Stroke Care at Akron CityHospital has earned the Gold Seal of ApprovalTM from The JointCommission for Primary Stroke Centers. The Center earned thisdistinction after The Joint Commission conducted an on-site reviewin November 2007. The Joint Commission’s Primary Stroke CenterCertification is based on the recommendations for primary strokecenters published by the Brain Attack Coalition and the AmericanStroke Association’s statements/guidelines for stroke care, whichcan significantly improve outcomes for stroke patients The JointCommission launched the program in 2003.Union Hospital has announced plans to open an InpatientRehabilitation Facility on the hospital’s third floor. The newunit will provide inpatient rehab services following a stroke,fracture of the femur, severe osteoarthritis, and certain neurologicaldisorders. The IRF will include ten inpatient beds and isexpected to serve patients from Tuscarawas County and manyof the surrounding counties. The project cost is estimated at$1.75 million. The hospital hopes to have the rehab unit openby December of 2008.WRH Health System received the 2007 Commitment toQuality Award from Ohio KePRO for outstanding clinical performancein patient care. This statewide recognition followed ayearlong partnership in the Appropriate Care Measures project withOhio KePRO. Ohio KePRO is Medicare’s Quality ImprovementOrganization and participating hospitals worked voluntarily to increasethe percentage of patients receiving appropriate care for acutemyocardial infarction (heart attack), heart failure and pneumonia– conditions that commonly require hospitalization. Those whoachieved these goals, improved clinical performance and reducedfailure rate by at least fifty percent.Special thanks to the hospital Public Relations administrators who submittedinformation for this column. To include your hospital’s news, add us toyour press release list or e-mail information to jraabe@akroncantonmdnews.com. The editorial deadline for the July-August issue of Akron/Canton M.D.News is June 3rd. ■CorrectionsBlaise Congeni, <strong>MD</strong>, is directorof Infectious Disease for AkronChildren’s Hospital. He wasincorrectly identified in a photo inthe article “Kids’ Health Trends”which appeared in the last issue ofGreater Akron/Canton M.D. News.In the taglines for the SpecialBlaise Congeni, <strong>MD</strong> Section articles written by Dr. PaulFerraro and Dr. Jason Fried in thelast issue of Akron/Canton M.D. News, it was noted that bothare on the surgical staff of Robinson Memorial Hospital. Drs.Ferraro and Fried are on the surgical staffs of all of theseSumma Health System hospitals: St. Thomas, Akron City,Barberton and Cuyahoga Falls General, as well as Robinson.Their offices are located in the latter two hospitals.advertisers’ indexAkron Children’s Hospital .........................Inside Back CoverAkron General Heart & Vascular Center .......................... 19Brookshire Financial Group, Inc. ..................................... 35Buckingham Doolittle & Burroughs, LLP ......................... 27CBIZ ................................................................................. 9Cleveland Clinic ............................................................... 10Drs. Hill & Thomas Co. .................................................... 21Hanger Prosthetics & Orthotics ......................................... 8Krugliak Wilkins Griffiths & <strong>Dougherty</strong> Co., L.P.A. .......... 11National City ................................................................... 32Northside Lofts ................................................................. 3Ogenix Corporation ............................................................ 7Regency Hospital Company ......................Inside Front CoverSirak-Moore Insurance, Inc. ............................................ 33Summa Physicians ..............................................Back CoverWeidrick, Livesay, Mitchell & Burge, LLC ........................ 12WRH Health System ........................................................ 133 6 | GREATER AKRON/CANTON M.D. NEWS MAY-JUNE 2008
The Division of Maternal Fetal Medicine offers basic and specialtyservices involving every facet of preconception care, reproductivegenetics and prenatal diagnosis and care.+ Well-coordinated care throughout pregnancy+ Accessibility to other specialists as needed+ Case managers assigned to guide each patient throughout process+ Staffed by board-certified perinatologists with advanced trainingand clinical experience in high-risk cases+ Targeted ultrasonography, fetal echocardiology, fetal MRI+ Genetic disease screening and counseling*Centers for Disease Control and Preventionwww.akronchildrens.orgRefer a patient at 330-543-4500.
Look who is part ofSumma Physicians Inc.Summa Physicians Inc. (SPI) is a Summa HealthSystem entity of multi-specialty physicians andpractices. Currently SPI employs over 150 physiciansin 20 specialties, including cardiology, colorectal surgery,dermatology, endocrinology, family medicine,gastroenterology, general surgery, geriatrics, gynecologyoncology, hematology/oncology, infectious disease, internalmedicine, obstetrics and gynecology, ophthalmology,orthopaedics and sports medicine, palliative care, plasticsurgery, psychiatry, sleep medicine, transplant surgery,urogynecology and vascular surgery. The mission of SPIis to promote stronger affiliation and employment ofphysicians in order to ensure that the health system meetscommunity and hospital needs for physician services nowand in the future, as well as to develop physician coveragein new markets.As a SPI physician, the benefits include:• A more predictable and stable compensation plan,regardless of the status of a patient. Physicians arecompensated for all clinical activity, compensation isnot based on profit/loss.• Stabilization of malpractice expenses• Management of physician office expenses andcorporate overhead• Professional management team skilled in practiceoperations, management and marketingTo learn more about SummaPhysicians Inc., visitwww.spi.summahealth.org.CardiologyMichael Bage, M.D.William B. Bauman, M.D.Kenneth E. Berkovitz, M.D.Roger B. Chaffee, M.D.David A. Cutler, M.D.Brian J. Donelan, M.D.Philip M. Dorfman, M.D.Stephen W. Fannin, M.D.Stephen M. Heupler, M.D.Michael M. Hughes, M.D.Mark A. Iler, M.D.Philip H. Keyser, M.D.Stephen A. Klautky, M.D.Daniel J. Newton, M.D.Otfried N. Niedermaier, M.D.Michael A. Pelini, M.D.Joseph F. Pietrolungo, D.O.Cynthia M. Pordon, D.O.Joseph D. Redle, M.D.Joseph M. Restivo, M.D.Joseph Rinaldi, M.D.David N. Rubin, M.D.Ted Shaub, M.D.Kevin H. Silver, M.D.Khaled Sleik, M.D.Jason K. Smith, M.D.A. Roger Tsai, M.D.Colorectal SurgeryJoel Porter, M.D.Frederick Slezak, M.D.DermatologyJulie A. R. Mark, M.D.Endocrinology<strong>James</strong> Salem, M.D.Family MedicineLisa Esterle, D.O.Michael Grimes, M.D.Jim Grow, M.D.Patrick Janovick, M.D.Patty Kitson, M.D.Suzanne Morgan, D.O.Rafael Osoteo, M.D.Demond Scott, M.D.Kathleen Scroggins, M.D.Douglas Wenger, M.D.GastroenterologyStephen Verbeck, M.D.General SurgeryThomas D. Bica, M.D.Nicholas Bisconti, Jr., M.D.Michael Cullado, M.D.Arthur Dalton, M.D.Adrian Dan, M.D.Kristen Dawson, M.D.William Fallon, M.D.Susan Goodrich, M.D.Dean J. Mayors, M.D.Warren Rose, M.D.Vicki Van Fossen, M.D.Gary Williams, M.D.John G. Zografakis, M.D.GeriatricsKyle Allen, D.O.Elizabeth Baum, M.D.Mary Jo Cleveland, M.D.Nancy Istenes, D.O.Natalie Kayani, M.D.Catherine Maxwell, M.D.Bill Zafirau, M.D.Hematology/OncologyDrew Abramovich, M.D.Joseph Koenig, M.D.Mehool Patel, M.D.Jennifer Payne, M.D.R. Douglas Trochelman, M.D.Infectious DiseaseShanu Agarwal, M.D.Hector F. Bonilla, M.D.Thomas M. File, Jr., M.D.Amy Hite, M.D.Anthony K. Leung, D.O.Joseph P. Myers, M.D.Jose E. Poblete, M.D.Michael J. Tan, M.D.Internal MedicineDonald Albainy, M.D.Troy Bishop, M.D.Irene Chenowith, M.D.M. Jeannette Cho, M.D.Matthew S. Chung, M.D.Leo Clavecilla, M.D.Dean Frate, M.D.Meredith D. Girard, M.D.- hospitalistLinda Ha, D.O.Michael F. Hill, M.D.Garimah Jones, M.D.Ron R. Jones, M.D.Teresa Koenig, M.D.George D. Laikos, M.D.Magaly Lopez, D.O.Michael J. Maggio, M.D.Neal R. Manning, M.D.Mark R. McRoberts, M.D.Dale Murphy, M.D.Hoai-Nghia Nguyen, M.D.Melodie Phillips, M.D.Julia Radwany, M.D.Steven Radwany, M.D.Michael Rich, M.D.Frederick Specht, M.D.Daniel Steidl, M.D.Diana Stewart, M.D.David Sweet, M.D.Stephanie Tan, M.D.Rex Wilford, D.O.Obstetrics and GynecologyAbbass Bagheri, M.D.Anita M. Bellante, M.D.T. Clifford Deveny, M.D.Timothy Drake, M.D.<strong>James</strong> Fanning, D.O.Bradford Fenton, M.D.Robert Flora, M.D.Meghan Foote, D.O.Steven Gaich, M.D.Gregory Kovacevich, M.D.Patrick Naples, M.D.Alexander Ormond, III, M.D.Christopher M. Rooney, M.D.Shannan C. Ross, M.D.Linda Upp, M.D.OphthalmologyNancy Awender, M.D.Deepak Edward, M.D.Orthopaedics andSports MedicineIan Alexander, M.D.Jeffrey Junko, M.D.Nilesh Shah, M.D.Scott Weiner, M.D.Palliative CareR. Daniel Cevasco, Jr., M.D.Kelly Letsinger, M.D.Plastic Surgery<strong>James</strong> Lewis, M.D.PsychiatryDavid Deckert, M.D.Christopher Durner, M.D.Gina Glenn, M.D.Amy Huddleston, Ph.D.Todd Ivan, M.D.John Kasper, M.D.Lynn Klimo, M.D.Rodney Myerscough, Ph.D.Nykolai Pidhorodeckyj, M.D.Thomas Robb, D.O.Roger Sparhawk, M.D.Joseph Varley, M.D.Bradly Winkhart, M.D.Sleep MedicineBen P. Graef, D.O.Transplant SurgerySantosh Potdar, M.D.Vascular SurgeryJohn A. Fink, M.D.Joseph McShannic, M.D.John Moawad, M.D.Drazen Petrinec, M.D.