John C. Andrefsky, MD - AkronCantonMDNews
John C. Andrefsky, MD - AkronCantonMDNews
John C. Andrefsky, MD - AkronCantonMDNews
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Greater Akron/Canton Edition | March-April 2008 VOL. 12, NO. 2www.akroncantonmdnews.comNeonatal IntensiveCare at Akron Children’sLawrence Singerman, <strong>MD</strong>,and Retina Associatesof ClevelandSpecial SectionChronic DiseaseManagement<strong>John</strong> C. <strong>Andrefsky</strong>, <strong>MD</strong>Surviving Stroke
from the publisherI’ve never understood why people smoke. It doesn’t look good, it doesn’t smell good, andit’s a proven health hazard. Last year 438,000 Americans died from smoking, according to theAmerican Lung Association (ALA). At the same time, tobacco companies spent $13 billionon promotions and advertising, much of which seemed to be aimed at kids.In a letter I received from Bernadette Toomey, the president of the ALA, she said, “Despitepromises to stop, Big Tobacco is courting new teen smokers to become its replacement generation.Just look at the marketing for Camel’s new No. 9 cigarette – pink packaging, advertisingin magazines popular with girls, and promotional giveaways including berry lip balm and cellphone jewelry. It’s the latest in Big Tobacco’s teen girl recruitment drive.“And when teens just give smoking a try, they’re getting addicted quicker and finding itharder to stop. Big Tobacco has increased the amount of nicotine in cigarettes — it is theirway to hook those they lure in.”The ALA is fighting back to protect our children. In addition to very active teen educationand cessation programs, the ALA is pushing Congress to give the FDA authority over tobaccoproducts. This would restrict tobacco companies’ marketing efforts to target teenagers.Since one of the best ways to prevent kids from smoking is to increase the price of cigarettes,the ALA is also working hard to convince Congress to pass a bill to increase cigarette taxesand use these revenues to fund health care for children.Of course, the ALA does not have a $13 billion advertising fund. But it does have somethingmuch more important — dedicated supporters like you and me. Please help the ALA pushback against the tobacco companies’ onslaught of marketing to youth. A $50 tax-deductibledonation will help protect teens from what Toomey refers to as “Big Tobacco” and will fostera tobacco-free future for them.For more information, or to make a donation, please visit www.lungusa.org/teens.Here’s to your health and to the health of our kids.Jan Raabe, PublisherGreater Akron/Canton M.D. Newsjan@akroncantonmdnews.comGreater Akron/Canton EditionPublisher: Jan RaabePhotographer: Joe Smithberger of SmithbergerPhotography, North Canton; Michael Lichterman ofClifford Norton Studio, ClevelandWriters: Liz Meszaros, Alex Strauss, RichardWeidrick, Paul Guerra, Marianne Lorini, NatalieMacLean, Tom Gotzy, Joseph Feltes, Collyn Floyd,Scott Zurakowski, Edward Murray, Joy Kosiewicz,Mary Link, Lee Ann O’Brien, Paul Ferraro, DO, JasonFried, DO, <strong>John</strong> Moawad, <strong>MD</strong>, Denise Signs, <strong>MD</strong>,Laurie Mooney, <strong>MD</strong>, James Prebis, <strong>MD</strong>, Joseph Coney,<strong>MD</strong>, Michael Novak, <strong>MD</strong>, Hernando Zegarra, <strong>MD</strong>M.D. News is published by Sunshine Media, Inc.8283 N. Hayden Rd., Ste 220Scottsdale, AZ 85258(480) 522-2900 | sunshinemedia.comPresident/CEO: Jim MartinFounder: Robert J. BrennanEditor-in-Chief: Liz MeszarosVice President of Marketing: Andrea HoodVice President of Recruiting &Publisher Development: Ken MinnitiMarketing Specialist: Kristine AldrinDirector of Publisher Development: Howard LaGraffeRecruiting Specialists: Teri Burke, Jennifer Young,Megan McCabeManager of Sales Administration: Cindy MaestasVice President of Creative Services: Tyler HardekopfProduction Director/Managing Editor: Keli QuinnCreative Services: Josh Bergmann, Rob Bonilla, DavidDrew, Gerry Dunlap, Breanna Fellows, Joanna Galuszka,Kristen Gantler, Amelia Gates, Brenda Holzworth, TessKane, Tanna Kempe, Lana May, Ryan Mills, Jodi Nielsen,Shannon WisbonDirector of Finance: Nick CranzFinancial Services: Malia Collins, Lori Elliott,Allison Jeffrey, Sharon Lardeo, Christian Williams,Cheng Wan ZhengCirculation Director: Holly CarnahanCirculation Manager: Beth LalimManager of Human Resources: Carrie HildrethManager of Information Technology: Eric HibbsPrinted by Sunshine Media PrintingWilliam H. Hibbs, Vice President & General ManagerSubscription rates: $18.00 per year; $36.00 two years;$3.50 single copy. Advertising rates on request. Bulk thirdclass mail paid in Tucson, AZ.Advertise in M.D. NewsFor more information about advertising in theM.D. News Greater Akron/Canton edition,call 330-499-5332or fax 330-497-0570or visit us at www.akroncantonmdnews.comContact InformationGreater Akron/Canton M.D. News6864 Mapleridge NWCanton, OH 44718jan@akroncantonmdnews.comAbout our mailing list: Akron/Canton M.D. News is mailed directly to 4,000 physicians and hospitalexecutives in 6 counties: Summit, Stark, Portage, Medina, Wayne and Tuscarawas.Although every precaution is taken to ensureaccuracy of published materials, M.D. News cannotbe held responsible for opinions expressed or factssupplied by its authors. Copyright 2008, SunshineMedia, Inc. All rights reserved. Reproduction inwhole or in part without written permission isprohibited.Postmaster: Please send notices on Form 3579 to P.O.Box 27427, Tucson, AZ 85726.05-737
contents VOL.12, NO. 2MARCH-APRIL 20084 COVER STORYJOHN C. ANDREFSKY,<strong>MD</strong>, FAHASurviving a stroke depends heavily onthe type of care a patient receives withinthe first few hours after the event. AtAultman Hospital, where Dr. <strong>Andrefsky</strong> isthe Medical Director of CerebrovascularServices, a team approach to stroke care ismaking a measurable difference. The proofis in Aultman’s certification as a PrimaryStroke Center by the Joint Commission.11 HOSPITAL FEATURENEONATAL INTENSIVECARE AT AKRONCHILDREN’S HOSPITALEach year, about 600 babies are admittedto the Level III Neonatal Intensive CareUnit (NICU) at Akron Children’s Hospitalwhere seven neonatologists, 22 pediatricsub-specialists, more than 100 nurses,and dozens of ancillary professionals aredevoting their lives to giving these infants afighting chance.19 PHYSICIAN FEATURELAWRENCE J. SINGERMAN,<strong>MD</strong>, RETINA ASSOCIATESOF CLEVELANDMore than 3 million Americans are blindor facing the threat of blindness from agerelatedeye disease. Specialists in retinalvascular and macular disease, Dr. LarrySingerman and his six physician partnersare focused on saving sight.DEPARTMENTS44 the sommelier45 sporting life47 hospital rounds1911ON THE COVER<strong>John</strong> C. <strong>Andrefsky</strong>, <strong>MD</strong>, FAHA4PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTON23 SPECIAL SECTIONChronic Disease Management2 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
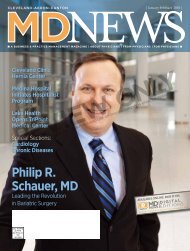
coverstory<strong>John</strong> C. <strong>Andrefsky</strong>, <strong>MD</strong>, FAHASurviving StrokeBy Alex StraussEvery 40 seconds, on average, someone in the United States hasa stroke. Among adults aged 20 and older, the estimated prevalenceof stroke in 2005 was 5,800,000 according to Heart Disease andStroke Statistics — 2008 Update published by the American HeartAssociation (AHA).The chance of surviving a stroke depends heavily on the type ofcare a patient receives within the first few hours after the event.Recognition of subtle symptoms, speedy high-tech imaging to confirmthe diagnosis, and access to skilled professionals and appropriate treatmentscan all make the difference — not only between life and deathbut also between a full, healthy life and a life of disability.Timely, high-quality stroke care is the ongoing goal of neurologistand stroke medicine specialist <strong>John</strong> <strong>Andrefsky</strong>, <strong>MD</strong>. The Section Chiefof Neurology and Medical Director of Cerebrovascular Services atAultman Hospital, Dr. <strong>Andrefsky</strong> was instrumental in helping Aultmanto achieve the coveted Joint Commission’s Certificate of Distinctionas a Primary Stroke Center in 2005 and 2007. Achievement of certificationsignifies that the stroke services provided have the criticalelements to achieve long-term success in improving outcomes.“Stroke is just behind heart disease and cancer as the top causeof disability and death in America. In 2004, it accounted for aboutone of every 16 deaths,” said Dr. <strong>Andrefsky</strong>, who is a Stroke Council<strong>John</strong> <strong>Andrefsky</strong>, <strong>MD</strong>, (right) is Medical Director of Cerebrovascular Services and Akhil Saklecha, <strong>MD</strong>, (left) is Chairman of Emergency Medicineat Aultman Hospital. Both were instrumental in helping Aultman to achieve the coveted Joint Commission’s Certificate of Distinction as a PrimaryStroke Center in 2005 and again in 2007.PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTON4 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
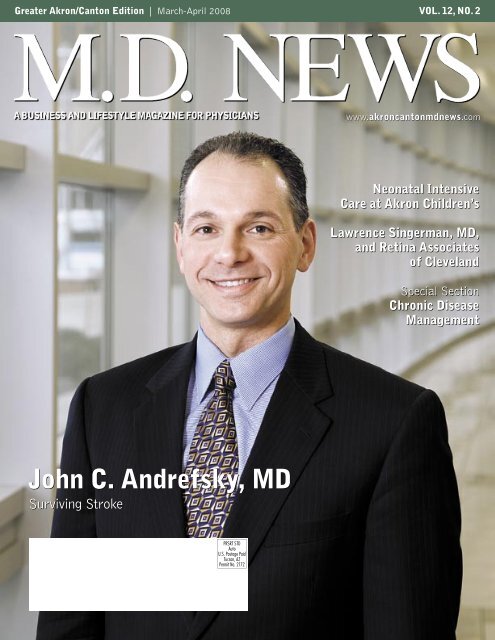
PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTONDr. <strong>Andrefsky</strong> leads quality improvement in the delivery of stroke care through the ongoingcollection and review of statistical data and through continuing education efforts. He is shownhere (far left) with family medicine resident Dr. Kevin McDaniel and Stroke Unit Director StacyIrwin.Fellow of the AHA. “But that statistic is a little misleading. Whilemore people tend to die of heart disease or cancer, many people canlive on for years with the devastating effects of a stroke. They may bealive, but they are not living fully.”Dr. <strong>Andrefsky</strong> believes the number of lives affected by strokes maybe much higher than statistics suggest, since every stroke patient’strauma extends to his or her family and loved ones. Not only has heseen this impact in his own practice at NeuroCare Center in Cantonand at Aultman, but he has also experienced it first hand with familymembers who suffered from hemorrhagic brain events.“When I was in college, I came home one day to find ambulancesoutside my house,” he recalled. “My grandmother had had a cardiacarrest and had just stopped breathing. She was in a coma for eightweeks before she died.”Dr. <strong>Andrefsky</strong>’s grandmother and aunt, with whom he was alsoclose, died of a subarachnoid hemorrhage. Although he is not certainwhether these early experiences directly influenced his decision topursue neurology and stroke medicine professionally, he believes theyhad an impact.“Subconsciously it may have driven me toward this profession,although I knew since third grade that I wanted to be a doctor,”said Dr. <strong>Andrefsky</strong>, who mentioned his hometown (Hazleton,Pennsylvania) pediatrician as another possible influence.“I did not know until much later what branch of medicine I wouldpursue. I looked at Intensive Care and atOrthopedics. But when I did a Neurologyrotation, I knew I had found it. The nervoussystem controls everything, every bodysystem, and what happens in the brain effectsyour whole body. It even forms yourpersonality. I just find it fascinating.”<strong>Andrefsky</strong> pursued residencies in InternalMedicine and Neurology in Pennsylvaniaand went on to fellowship training inNeuroIntensive Care at the Cleveland ClinicFoundation, where he later (for 6 years)directed Neuromedical/NeurosurgicalIntensive Care and won a Teacher of the YearAward in the Department of Neurology.Since 2003, he has been an associate professorat NEOUCOM, where he also won aTeacher of the Year Award, and has directedAultman’s Cerebrovascular Services.“We are proud of our Primary StrokeCenter certification. It is the result of agreat deal of effort on the part of everyoneinvolved with the stroke program,” said Dr.<strong>Andrefsky</strong>.Designation as a Joint Commission PrimaryStroke Center required that Aultman initiatean interdisciplinary team approach to strokecare across the continuum. Delivery of care had to be standardizedwith established, written clinical practice guidelines and protocolsalong with a system for ensuring compliance.Now, Dr. <strong>Andrefsky</strong> must continue to lead quality improvementin the delivery of stroke care at Aultman through the ongoing collectionand review of statistical data. And Aultman must keep itspractitioners and staff members on the cutting edge of stroke carewith continuing education, a service it also extends to EmergencyMedical Services (EMS) personnel and to the community, as well.However, as Dr. <strong>Andrefsky</strong> pointed out, Aultman’s Stroke Centercan only be of help if patients can access it.“Right now there is a huge discrepancy between the kind of strokecare you can get at a smaller hospital and the care you can get at alarger facility like Aultman,” Dr. <strong>Andrefsky</strong> said. “In a small hospital,they often don’t have the tools or people to adequately treat patientswith stroke, and there is not always a good system in place to get thosepeople where they need to go. I believe that there needs to be somekind of regionalization of stroke care so that it is clear which patientsshould be transferred to Aultman and which to another facility, sothat the transfer can happen very quickly.”Dr. <strong>Andrefsky</strong> helped establish such a system at Aultman whereimaging technologies like CT angiograms can quickly determine thetype of stroke and the extent of stroke damage. If treatments suchas intra-arterial treatments for the removal of clots are needed, theGREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 5
local docs in national newsDR. NICK JOURILESPRESIDENT-ELECT OF ACEPThe American Collegeof Emergency Physicians(ACEP) announced thatNicholas J. Jouriles, <strong>MD</strong>,FACEP, an Akron GeneralMedical Center physician,was elected president-electduring the organization’sannual meeting in Seattle.Dr. Jouriles was elected byACEP’s Council to serve aone-year term, and he willDr. Nick Jourilesassume ACEP’s presidencyat the organization’s annualmeeting in Chicago.Dr. Jouriles is an attending physician at Akron General’s Departmentof Emergency Medicine and core faculty for the hospital’s EmergencyMedicine residency program. He also is professor of EmergencyMedicine at Northeast Ohio Universities College of Medicine.Dr. Jouriles has served in many ACEP leadership roles, includingvice president in 2006-2007. He also chaired several committees,including Educational Meetings and Bylaws. He received the ACEPCouncil’s Meritorious Service Award in 2002 for his outstandingcontributions to the specialty of emergency medicine. Inaddition, Dr. Jouriles chaired ACEP’s 2003 Scientific Assemblyprogram, the world’s largest emergency medicine meeting. Healso served as president of Ohio ACEP in 1997 and was appointedchair of the International Federation of Emergency MedicineEducation Committee.A graduate of University of Pennsylvania, Dr. Jouriles obtained hismedical degree from Case Western University and completed residencyin Internal Medicine at Dartmouth Hitchcock Medical Centerand in Emergency Medicine at Denver General Hospital.ACEP is a national medical specialty society representing emergencymedicine with more than 25,000 members in 53 chapters representingeach state, as well as Puerto Rico and the District of Columbia.A Government Services Chapter represents emergency physiciansemployed by military branches and other government agencies.DR. KYLE ALLEN CHOSEN FORNCOA LEADERSHIP COUNCILKyle Allen, DO, AGSF,has been appointed to theNational Council on Aging(NCOA) Leadership Council.The National Council onAging works to improve thelives of older Americans.NCOA programs help olderpeople remain healthy andindependent, find jobs, accessbenefits programs, anddiscover meaningful waysto continue contributing tosociety.Dr. Kyle AllenDr. Allen was nominatedand selected by the NCOA’sBoard of Directors. As a member of the Council, he has the opportunityto influence not only the mission and strategy of NCOA but thedirection of aging policy and services throughout the nation.Dr. Allen serves as chief of the Division of Geriatric Medicineand medical director of Post-Acute and Senior Services at SummaHealth System. In addition to his role on the NCOA LeadershipCouncil, Dr. Allen is a Practice Change Fellow, a program sponsoredby Atlantic Philanthropies and the <strong>John</strong> A. Hartford Foundationthat works to develop leaders who can effectively promote high qualitycare for people as they age. Additionally, in 2007, Dr. Allen was namedthe Physician of the Year by the Ohio Association of Gerontologyand Education. ■8 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
Affinity to Consolidate to the Massillon CampusThe Board of Trustees of Affinity Medical Center has approveda consolidation plan that will move all the acute care services presentlylocated on the Doctors campus to the Massillon campus inthe second quarter of 2008.“Since implementing our short-term service model this pastyear, which included providing general acute services at theDoctors campus (the former Doctors Hospital) and specialcare services at the Massillon campus (the former MassillonCommunity Hospital), the hospital has continued to carefullystudy and assess our community’s healthcare needs and thestrategic direction of the hospital,” said Ray Martinez, AffinityMedical Center’s Board Chairman. “We are confident this decisionwill benefit our community by keeping healthcare local andcreating a stronger, more comprehensive healthcare provider inour community.”The decision to consolidate to the Massillon campus was reachedfollowing an extensive study that included an architectural reviewof the two campus structures, interviews with physicians and amarket analysis.The consolidation plan is designed with an emphasis on providingbetter efficiencies for staff and physicians so they can focus theirattention on providing patient care at one location, convenient tothe communities the hospital serves.Affinity’s two Emergency Departments (ED) treat close to35,000 patients per year. Both EDs will remain open while therenovation project is underway. Future plans for the Doctors campusED and hospital building are still being considered. For the timebeing, both facilities will maintain their current services.Some details about individual services that will be transitioningto the Massillon campus are still being developed. As thesechanges take place, Affinity plans to keep physicians, patients andmembers of the community informed through paid advertising, itswebsite, newsletters and written materials that will be distributedto physicians’ offices.RONALD L. BIERMANNAMED CEO AT AFFINITY MEDICAL CENTERAffinity Medical Center announced theappointment of Ronald L. Bierman as thehospital’s new CEO, effective January28, 2008.Bierman comes to Affinity Medical Centerfrom Hialeah Hospital in Hialeah, FL, wherehe served as the hospital’s CEO. Prior tojoining Hialeah, he held CEO positions atseveral hospitals, including Parkway Regional Ronald L. BiermanMedical Center in North Miami Beach,FL; Carlisle Regional Medical Center in Carlisle, PA; Lower KeysMedical Center in Key West, FL; HealthSouth Northern KentuckyRehabilitation Hospital in Edgewood, KY; and St. Francis HealthcareSystem in Miami Beach, FL.Bierman holds a Bachelor of Science degree in HealthcareAdministration and a Master of Science degree in Adult Educationfrom Florida International University in Miami and a Master ofBusiness Administration degree from the University of Miami. ■Correction NoticeThe following listing was omitted fromthe Weight Loss Surgery category ofthe 2008 M.D. News Annual Directoryin the January-February issue:Akron General Medical CenterBariatric Center400 Wabash Ave, Akron330-344-1100www.akrongeneral.orgGREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 9
Changes in Anti-Markup RulesBy Joy Kosiewicz and Mary T. LinkIn the 2008 Medicare physician feeschedule, CMS substantially expandedthe scope of the anti-markup provisions.The revised anti-markup provisions applyif a physician, physician organizationor other supplier bills for the technicalcomponent (TC) or the professionalcomponent (PC) of a diagnostic test,the test was ordered by the billing physicianor other supplier or a party relatedby common ownership or control, andthe test is either: (1) purchased from anoutside supplier, or (2) performed at asite other than the office of the billingphysician or other supplier.EFFECTIVE DATE ANDAPPLICABILITY DATEThe rule changes are effective as ofJanuary 1, 2008. However, as of January1, 2008, the revised anti-markup provisionsonly apply to: (1) the TC ofany purchased diagnostic test, and (2)anatomic pathology diagnostic testingservices furnished in space that is utilizedby a physician group practice as a “centralizedbuilding” for purposes of complyingwith the self-referral rules; and does notqualify as a “same building.”The revised anti-markup provisionswill not apply to the PC of a diagnostictest until January 1, 2009. The reasonfor the delay is to clarify what constitutesan “office of the billing physicianor other supplier.” CMS intends to issueguidance, propose additional rulemakingor both.KEY CHANGES TO RULESSite of Service. The rules will nowapply to tests ordered and billed by a physicianin a group practice, but performedat a location other than the “office” of thebilling practice. However, CMS receivedcomments which raised concerns that“office of the billing physician or othersupplier” may not be entirely clear andcould have unintended consequences.Specifically, some commenters indicatedthe definition is unclear with respect towhether certain space arrangements areincluded. Others were concerned thatif office space which satisfies the “samebuilding” test or otherwise complies withthe physician self-referral rules is nowsubject to the anti-markup provisions,physician groups will not be able to renderservices cost-effectively and patient accesswill be disrupted. Thus, CMS has decidedto study these issues further.Until CMS issues further guidanceor additional rules, the following newdefinitions are applicable to TCs andanatomic pathology diagnostic testingservices:• “Office of the billing physician orother supplier” means “space where thephysician or other supplier regularlyfurnishes patient care.”• The “office” of a group practice meansspace in which the organization furnishes“substantially the full range ofpatient care services” that the practiceprovides generally. This new “office”test differs from the “same building”test used in the Stark in-office ancillaryservices exception. In order to meetthe “office” location standard, the PCor TC must be furnished in the sameoffice suite where physician servicesare furnished.Purchased from Outside Supplier.The anti-markup provisions continue toapply to services furnished by “outsidesuppliers,” but this term now meansanyone who is not a full or part-timeemployee of the billing practice and whodoes not furnish the PC or TC to the billingpractice under a reassignment.Expansion to TC. The anti-markupprovisions will now apply to both the PC(except the rule changes will not applyuntil January 1, 2009) and the TC (therule changes apply as of January 1, 2008)of diagnostic tests (other than diagnosticclinical laboratory tests).Focus on Ordering. There will be anew focus on who ordered the test. Whena test is ordered by a physician outsidethe billing physician practice, the testwill not be subject to the anti-markupprovisions. However, the “related party”rules must be considered when determiningwhether an ordering physicianis outside the billing practice.Net Charge. A supplier’s “net charge”now must be determined without regardto the cost of equipment or space leasedto the performing supplier by or throughthe billing physician. Furthermore, thebilling physician may not include billingor other overhead costs when calculatingthe net charge.Other Suppliers. The rules willapply not only to physicians, but alsophysician organizations and other suppliers,such as IDTFs.Joy Kosiewicz and Mary Link are attorneysin the Health Care Group at BrouseMcDowell. Ms. Kosiewicz practices in theareas of Health Care and Real EstateLaw, representing health systems, physiciangroups and health plans in a variety ofregulatory, real estate and corporate matters.Ms. Link counsels hospitals, physicians, homehealth agencies, hospices, dialysis facilitiesand other providers on the full spectrum ofhealth care issues. ■1 0 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
Neonatal Intensive Care atAkron Children’s HospitalGiving Fragile Lives a Fighting ChanceBy Alex Strausshospital featureEach year, about 600 babies are admitted to the Level IIINeonatal Intensive Care Unit (NICU) at Akron Children’sHospital. While almost all are small, about one-fourth of theseinfants have been in utero for fewer than 32 weeks, five weeksless than what is considered necessary for full gestation. Someof these tiny babies are as young as 24 or 25 weeks and weigh inat less than a kilogram.At this age and size, life is precarious at best. But seven neonatologists,22 pediatric sub-specialists, more than 100 nurses, and dozensof ancillary professionals at Akron Children’s are devoting their livesevery day to giving these children a fighting chance.“The most common diagnostic condition that we see here ispremature birth and associated medical problems,” said AkronChildren’s Director of Neonatology Anand Kantak, <strong>MD</strong>. “TheAkron Children’s multidisciplinary NICU team includes seven neonatologists, 22 pediatric sub-specialists, more than 100 nurses, and dozens ofancillary professionals.PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTON1 1 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 11
On any given day, there are typically 45 to 50 babies receiving care in Akron Children’s 59-bed NICU.PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTONtwo most common medical problems are pulmonary because ofunderdeveloped lungs, or neurological, affecting their brains,nerves, mental development or movement. The third most commonproblem that brings them here is some type of congenitalabnormality. Near-term babies do not usually come here unlessthey have some other problem.”FULL SERVICEOn any given day, there are typically 45 to 50 babies receiving carein Akron Children’s 59-bed NICU. Some of these children are fightingfor their lives, while others have survived their battles and are close tobeing ready to go home. To ensure the appropriate level of attentionfor each little patient, they are categorized as needing either intensivecare or sub-intensive care.“Although these are not geographically distinct areas withinthe unit, we use these categories to help determine staffing needswhile the babies are here and to coordinate the care these patientsare going to need as they transition into a home environment,”explained Dr. Kantak.For those needing intensive care, Akron Children’s multidisciplinaryteam is led by the neonatologists who coordinate day-to-daycare. On a rotating basis, one is physically present in the unit 24/7.At all times there are also 20 to 25 specialized neonatal nurses and atleast one of nine neonatal nurse practitioners on hand. Four pediatricsurgeons and pediatric sub-specialists in cardiology, pulmonology,orthopedics, infectious diseases, genetics, neurology, ENT and othershelp ensure that every fragile patient has access to the very bestmedical care available.“There is no absence of any subspecialty at Akron Children’s,” saidDr. Kantak. “That is why we are able to call ourselves a ‘full service’NICU. It is like a very large symphony orchestra of care providerswith the neonatologist acting as the conductor.”For babies who have transitioned into the sub-intensive carecategory, there is also a whole team of ancillary support specialists,ready to help them and their families prepare for life outsidethe hospital.“There are a number of specialists involved in not only caring forthese babies here in the unit, but also getting them and their familiesready to go home,” explained Dr. Kantak. “For example, we havespecialists in nutrition and respiratory care, lactation consultants,social workers, and case managers who help to coordinate the carethat will be required at home and beyond.”HIGH TECH, LOW KEYAlthough Dr. Kantak is quick to point out that technology alonedoes not make a great NICU, he is proud of the high-end therapiesavailable to Akron Children’s littlest patients. Among them is extracorporealmembrane oxygenation (ECMO), a technique for providingboth cardiac and respiratory support oxygen to patients who cannotyet get enough on their own.1 2 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 12
“This is a therapy that is very cutting edge and requires an extremelyhigh level of skill,” said Dr. Kantak. “Only a few centers in the entirestate are equipped with this kind of technology and expertise.”Akron Children’s was the first medical facility in Ohio tomake Cool-Cap available to newborns diagnosed with hypoxicischemicencephalopathy, an interruption in blood flow andoxygen to the brain at birth. This head-cooling cap has beenproven to ameliorate brain damage by lowering the infant’s headand body temperature.Perhaps just as important as the high-tech treatments offered inAkron Children’s NICU are the low-lighting, low-noise policies inplace so the infant patients are not unnecessarily exposed to brightlights or high levels of noise or confusion. According to Dr. Kantak,such stimulation can impede brain development and slow recoveryand growth.He also believes it is important for families to be a vital part of thecare delivery team in the NICU, rather than sitting in waiting areas.Families are encouraged to be on hand, helping and engaging in skinto-skincontact with their babies.“We make an effort to engage them in all aspects of care, includingthings like setting up tube feeding,” said Dr. Kantak. “This is one of thethings that puts us at the highest level of family-centered care.”Families whose children have “graduated” from the NICU areinvited to participate in on-going efforts to refine and improve carefor future babies and families. This “feed forward” (as opposedto feedback) method of evaluating care is just one example of theself-assessment efforts Dr. Kantak believes sets Akron Children’sHospital apart from most other NICUs in the country.IMPROVING OUTCOMES“What you can see happening, in terms of care delivery in ourNICU, is really just the tip of the iceberg of what we do,” Dr. Kantakexplained. “We are constantly engaging in education, training,prevention efforts, collaboration and data monitoring with a viewtoward constantly improving our level of care.”Just as each baby’s vital signs are monitored, Akron Children’sNICU constantly monitors patient outcomes and compiles andevaluates the data with a view toward improving those outcomes.In addition, Dr. Kantak explained, his team collaborates with morethan a dozen other NICUs around the country to share informationand knowledge and to develop evidence-based action plans.“We are constantly changing our action plan based on the evidenceavailable to us through our own data and through the data we getfrom our collaborative efforts,” said Dr. Kantak. “We are constantlyasking ‘How are we doing compared to the best in the world?’ As aresult of our efforts, our outcomes continue to improve.”Although their focus is on delivering care to sick babies, Dr. Kantakpoints out that the underlying mission of Akron Children’s Hospitaland its NICU is prevention.“Primary prevention means keeping babies from having a problemin the first place. You do this through community education andthrough primary care providers. Secondary prevention means that,if there is a problem, you deal with it in a prompt, safe, and effectiveway and resolve it quickly. And tertiary prevention means asking, inlight of the problems that exist, how we can create the best outcomeand quality of life for this child and family.”In light of the NICU’s efforts at preventive care, the March of DimesAkron Children’s recently opened the 6,000-square-foot Reinberger Family Center adjacent to the NICU for families who want to remain near theirbabies. Here, families will find comfortably furnished living rooms with televisions, a play room for siblings, a kitchen/dining room with vendingmachines, computers with internet connections, bedrooms with attached bathrooms, laundry facilities, and private lactation rooms with rocking chairs.PHOTO © SMITHBERGER PHOTOGRAPHY, NORTH CANTON1 3 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 13
Random Thoughts for 2008By Richard Weidrick, CPARather than devote this space to a singulartheme I would like to provoke some thought bytouching on a variety of topics.Tax rebates. Does the President andCongress really think a rebate of $400 - $600per person will stimulate the economy? Whatwill $400 buy anyway? The last time rebateswere handed out they ended up to be tax refundsissued a year in advance. The national savings rateis currently at a negative one-half percent. Thelast time this country had a negative savings ratefor an entire year was 1933. Should we reallybe encouraging people to spend more? Whynot increase the incentives to save by raising thelimits for IRA contributions?Electronic check transmission. Remotecapture allows you to scan checks at your officeand transmit electronically to your bank.Basically it turns a check into an ACH item.Recently we have seen the cost of remote capturecome down. Ask your banker if it makessense for your practice and save time and tripsto the bank.Mortgage pay-off. Often clients ask if theyshould pay off a mortgage or invest additionalmonies in the stock market. Given the phasedout benefit of the mortgage interest deductionconsider eliminating debt. The psychologicalbenefit is huge.Segregation of office duties. Rethinkyour office design and who controls which responsibilities.Challenge yourself on the propersegregation of duties. Is the same person responsiblefor crediting patient accounts also takingdeposits to the bank?Password maintenance. Is your practicelike most where passwords are required to accessevery computer application? Who maintainsthese passwords? At least two people in youroffice should know them at any given time.Reduce the risk that a disgruntled employeecan shut down your practice by locking up yourcomputer applications.Long-term care insurance. Many havenot gotten around to purchasing long-term careinsurance. Long-term care insurance will helpprotect your accumulated savings in the event youneed extended care either in-home or at a facility.A popular strategy is to insure for a limited benefitutilizing the coverage as a stop gap and not fullyfunding this particular need. You should reviewthe shared care options which would cover you andyour spouse and should qualify for a discountedprice. Remember … long term care may betax deductible.Rich Weidrick is a CPA and principal of Weidrick,Livesay, Mitchell & Burge, LLP, in Akron. ■We Can KeepYour Practice HealthyGrow your business your way with Physician-based accounting.Weidrick, Livesay, Mitchell & Burge’s is staffed with experienced accountingprofessionals with a focus on physician practices. We specialize in physician-basedbusiness accounting to help doctors achieve their potential and remain successful.Controlling overhead, managing collections, personal taxes and retirement planningfor our clients means you are free to concentrate on your specialties...your patients, your practice, your family.Call us today to find out what we can do for you!WEIDRICK, LIVESAY,MITCHELL & BURGE, LLCC E R T I F I E D P U B L I C A C C O U N T A N T S2150 North Cleveland-Massillon Road • Akron, Ohio Akron: 330-659-5985 Medina: 330-722-5249GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 15
legal-easeOhio Supreme Court Limits PublicPolicy Wrongful Discharge ClaimsBy Scott M. Zurakowski, Esq., and Edward D. Murray, Esq.Recently, the Ohio Supreme Court determinedthat at-will employees in Ohiodo not have a common law action forwrongful discharge merely because theywere discharged while receiving workers’compensation benefits. See Bickers v.W & S Life Insurance Company, 2007 Ohio6751 (Ohio 2007). This decision clarifiesthe Court’s 2003 decision in Coolidge v.Riverdale Local School District, in which theCourt held an employee may sue an employerfor wrongful discharge in violation of publicpolicy where the employee is discharged fornonretaliatory reasons while receiving workers’compensation benefits. As a result of theBickers decision, at-will employees are limitedto filing claims for retaliatory discharge underOhio’s Workers’ Compensation Act.Bickers was an at-will employee who, atthe time of her discharge, was receivingtemporary total disability benefits. Bickers’suit claimed, among other things, that shewas discharged while receiving temporarytotal disability benefits in violation of publicpolicy. In support of her position, Bickersrelied expressly on the Supreme Court’searlier decision in Coolidge.Coolidge involved a discharge of a publicschool teacher who was also receivingtemporary total disability benefits at thetime. Coolidge was employed under a contractgoverned by state law relating to theemployment of teachers, which requiredgood and just cause for termination. Thecourt, in Coolidge, held “An employee whois receiving temporary total disabilitycompensation pursuant to Revised Code §4123.56 may not be discharged solely on thebasis of absenteeism or inability to work,when the absence or inability to work isdirectly related to an allowed condition.” Asa result, some courts interpreted Coolidgeto expand the public policy exception tothe state’s employment-at-will doctrine.As a result of the Supreme Court’s decisionin Bickers, the Coolidge decision is limitedto considerations of whether “good andjust cause” supports the termination of1 6 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
financial planningStock Market Ups and DownsBy Paul D. Guerra, AIFIt has often been said that there are onlytwo certainties in life: death and taxes. Asinvestors, we face a third, and sometimesunnerving, reality in that financial marketsdo not move in only one direction.They rise and fall - sometimes sharply - inresponse to changes in the overall healthof our economy. We can easily forget thatfact during good economic times, but themarket always stands ready to offer us agentle reminder. So far, that’s just what2008 has done.It’s nearly impossible to read the paperor watch the news without hearing direwarnings about the subprime “meltdown,”the housing market “collapse,” and “dismal”job growth, which are hampering oureconomy. These, and other concerns, havemany prognosticators calling for a U.S.recession in 2008. We certainly don’t takethese concerns lightly, and we are monitoringconditions carefully.But such attention-grabbing language,while currently in vogue, runs the risk ofmisdirecting our attention from the biggerpicture and the ultimate goal. As investmentprofessionals, we construct portfoliosaround the important concepts of diversification,time horizon, and risk tolerance. In*Hypothetical cumulative return for period indicatedtimes of uncertainty, you should reflect ontwo important questions:1. What is your investment time horizon?(How long will your money be invested?)2. Are you comfortable riding out themarket fluctuations that your portfolioexperiences?The period from 2000 to 2002 is widelyregarded as one of the worst bear marketsin U.S. stock market history. Stocks, asmeasured by the S&P 500 Index, lost 38percent of their value during those threeyears. Yet, a diversified portfolio of 50 percentstocks/50 percent bonds would havesuffered only a 6-percent decline.Of course, that balanced portfolio wouldalso have appreciated less from 2003 to2000 - 2002* 2003 - 2007*100% stocks - S&P 500 - 38% + 83%100% bonds -Lehman Aggregate Bond+ 33% + 24%50% stocks, 50% bonds - 6% + 52%2007, when stocks rocketed ahead by 83percent. The table below shows the impactthat portfolio diversification can have in upand down markets.After five consecutive years of strongstock market returns, a pullback shouldnot be unexpected or cause us to drasticallychange course. It is simply part ofthe normal economic cycle. The key isto appropriately diversify your portfolioto align with your investment goals,time horizon, and risk tolerance. Thatis what should be done in both good anddifficult times - and that is what we shouldcontinue to do now.Paul D. Guerra is an Accredited InvestmentFiduciary (AIF) and the president of BrookshireFinancial Group, Inc. in Canton. ■an employee protected by the state’s lawgoverning the employment of public schoolteachers. Most importantly, the court inBickers specifically determined that “theconstitutionally sanctioned, and legislativelycreated, compromise of employerand employee interests reflected in theworkers’ compensation system precludes acommon law claim of wrongful discharge inviolation of public policy when an employeefiles a workers’ compensation claim and isdischarged for nonretaliatory reasons.”For employers, the decision clarifiesthat an employee who believes he or shehas been discharged in retaliation for filinga workers’ compensation claim mustfollow the requirements for filing a retaliatorydischarge claim as set forth in theWorkers’ Compensation Act. Accordingto the Supreme Court’s decision in Bickers,legal-easeemployees may no longer claim a violationof public policy.NOTE: This general summary of thelaw should not be used to solve individualproblems since slight changes in the factsituation may require a material variance inthe applicable legal advice.Scott Zurakowski and Edward Murray are attorneyswith the law firm of Krugliak, Wilkins, Griffiths& Dougherty Co., LPA, in Canton, Ohio. ■GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 17
Lawrence J. Singerman, <strong>MD</strong>, founder/president,Retina Associates of Cleveland2 0 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
on saving sight. A researcher, as well as a clinician, he’s worked hard to fi nd newtechnologies and treatments for eye diseases that impair or threaten to destroy vision.In fact, Dr. Singerman has participated in more than 90 clinical trials, 24 ofwhich were funded by the National Institutes of Health (NIH). The results of thatresearch have been published in more than 275 peer-reviewed journal articles andabstracts and presented at over 200 meetings and symposia around the world.Throughout his career, Dr. Singerman has been an active participant in numerousmedical associations and organizations. He currently serves as a medical advisor tofour national organizations and is an editor or scientific referee for 13 professionaljournals including Retina, New England Journal of Medicine, and Archives of Ophthalmology.He’s also the executive secretary of The Macula Society, which he founded 30 yearsago as a forum for the most prominent vitreo-retinal specialists in the world topresent and critique new research in retinal vascular and macular disease.“We currently have 340 members,” said Dr. Singerman. “The fi rst president wasmy mentor in retinal disease at <strong>John</strong>s Hopkins University, Dr. Arnall Patz. Helater became the chairman of the Department of Ophthalmology there. He wasperhaps the most respected and leading ophthalmologist in the world for at leasta decade and ended up receiving the Presidential Medal of Freedom, the highestcivilian award in the country.”Dr. Singerman has won several awards, as well, including two Honor Awardsfrom the American Academy of Ophthalmology. Recently he also received twoLife Achievement Awards—one from the American Academy of Ophthalmologyand one from the Dietrich Diabetes Research Institute of the Diabetes Associationof Greater Cleveland.When asked how he felt about his career to date, Dr. Singerman replied, “Veryfortunate. I’ve been fortunate throughout my entire career—to get the specialtytraining that I did, to be involved in the clinical trials that I have, and to be partof the team of professionals I’m associated with.”A self-described hard worker, Dr. Singerman decided to become a physician ata relatively young age because he thought it would be a gratifying career. Afterreceiving his <strong>MD</strong> degree from Wayne State University in Detroit, he completedan internship and residency at Mt. Sinai Medical Center, where he won the UlmerAward for Outstanding Research in Ophthalmology. Afterward, he sought fellowshiptraining in Retina at The Wilmer Ophthalmological Institute of <strong>John</strong>s HopkinsUniversity because “it was clearly the best program in the country.” While there,Dr. Singerman became committed to clinical trials.“When I was in my retinal fellowship at <strong>John</strong>s Hopkins in 1973 and 1974, wewere involved in the original Diabetic Retinopathy Study. This was an NIHsponsoredstudy that proved conclusively that laser therapy is very effective forproliferative diabetic retinopathy,” he said. “Before that it was considered a verycontroversial treatment.”That study, he explained, turned out to be a landmark NIH-sponsoredstudy—not only because it proved the effectiveness of laser therapy for diabeticretinopathy, but also because it set a new standard for clinical trials in all branchesof medicine. According to Dr. Singerman, NIH was very pleased with the resultsof this study.“Within a year or two of the publication of the results in 1976, the incidence ofblindness from diabetic retinopathy plummeted around the world. It really hadan impact. And when I saw the impact that it had, I decided that I would devote alot of my professional time to clinical trials,” said Dr. Singerman.IMAGES COURTESY OF LAWRENCESINGERMAN, <strong>MD</strong>GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 21
Retina Associates includes seven ophthalmologists subspecialty trained in Retina, four certified physician assistants/surgical assistants, and morethan 100 employees. Most are shown in this photo.PHOTO © 2007 MICHAEL LICHTERMAN, CLIFFORD NORTON STUDIO, CLEVELANDAnd he does, along with his six physician partners; 12clinical trial coordinators, including 3 clinical trial nurses;12 ophthalmic photographers; a research liaison; and anIT specialist. Retina Associates is part of the DiabeticRetinopathy Clinical Research (DRCR) network which isan NIH affiliate.“I’m really proud of the team we have here. All of thedoctors are subspecialty trained in retina, and they’re reallyquite talented.”They are Drs. Michael A. Novak, Hernando Zegarra,Z. Nicholas Zakov, Scott D. Pendergast, David G. Millerand Joseph M. Coney. Retina Associates offices are locatedthroughout Northeast Ohio in Beachwood, Lakewood,Lorain, Middleburg Heights, Youngstown, Warren, Mentor,Salem, and Akron.“All of our doctors participate in clinical trials and they allparticipate in teaching, as well,” said Dr. Singerman. “But inaddition to the physicians, we have four physician assistants/surgical assistants certified by the state and more than 100 employees,many of whom are highly trained in their disciplines.We’ve sort of spoiled ourselves with an excellent staff.”Currently, Retina Associates is involved in 24 clinicaltrials, most of which are for A<strong>MD</strong> and diabetic retinopathyand most of which are directed at drug therapy, also knownas pharmacotherapy.“Pharmacotherapy is clearly the treatment for retinal diseasestoday. And we’ve been involved in the clinical trials forevery one of the retinal drugs, the most important to datebeing anti-vascular endothelial growth factor (anti-VEGF)drugs,” said Dr. Singerman.He explained that anti-VEGF therapies block new bloodvessel formation. They also have an anti-permeability effect.“When we inject the drug into the vitreous, the retinagets thinner, and patients often experience an immediateimprovement in vision,” he said. “This probably has beensignificant in generating greater patient compliance inreturning for regular injections.”Dr. Singerman is hopeful that new pharmacotherapies willreduce the incidence of blindness, despite the continued agingof the population.“Certainly much work has yet to be done, but the futurefor treating retinal diseases has never been more optimistic,”he said. ■For more information or to refer a patient, call 216-831-5700or visit Retina Associates’ web site at www.retina-doctors.com2 2 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
An Update on Managementof Aortic AneurysmsBy <strong>John</strong> Moawad, <strong>MD</strong>Abdominal aortic aneurysm (AAA)is the thirteenth leading cause of deathand accounts for 15,000 deaths per year,more than many malignancies. Roughly200,000 new AAA’s are diagnosed eachyear in the United States leading to40,000 elective AAA repairs per year.The highest incidence of AAA occursin men who have ever been smokers.Recently, the U.S. Preventive ServicesTask Force has recommended screeningof high risk patients for AAA,and Medicare has approved one-timescreening ultrasound of men over age65 who have ever smoked, as well asmen or women who have a family historyof AAA. The management of thesepatients with asymptomatic abdominalaortic aneurysm has shifted over thepast decade.Ideally, patients are referred for repairof AAA prior to rupture as the mortalityof a ruptured AAA is as high as 80%.As aneurysms grow in diameter, therisk of rupture increases. Thus, AAA’sless than 5 cm in diameter have a verylow risk of rupture and generally donot warrant repair. Nevertheless, thesepatients need to be followed every six totwelve months to check for aneurysmgrowth. Aneurysms greater than 5 cmshould be referred to a vascular surgeonfor repair. Open surgical repair has beenwidely used for the past fifty years withproven long-term durability, but, despiteimprovements, open AAA repair stillcarries significant morbidity and mortality.In fact, many elderly patients surviveopen AAA repair, but spend six monthsor more before resuming their preoperativeactivity level.By avoiding a laparotomy and aorticspecial section: chronic diseasesIdeally, patients are referred for repair of AAA priorto rupture as the mortality of a ruptured AAA is ashigh as 80%. As aneurysms grow in diameter, the riskof rupture increases.cross clamp, endovascular AAA repair(EVAR) is a less invasive method of repair,leading to lower perioperative mortalityand morbidity as demonstrated in threerandomized trials. An aortic stent graftis inserted via the femoral arteries in thegroin and then opened within the aorta,essentially reinforcing the aortic wall andpreventing rupture. Since their initialintroduction, aortic stent grafts haveundergone numerous improvements,and the current devices are able to treata wider range of aortic anatomy thanwas initially feasible. Patients generallyare discharged from the hospital in 24to 48 hours and often return to normalactivity within two weeks. Nevertheless,it is important to realize that not allpatients are candidates for EVAR due tocomplicated anatomy and other factors.Additionally, long-term complications ofstent migration, occlusion, and persistentflow within the aneurysm sac are notuncommon and mandate close follow-upand sometimes additional procedures.As such, the importance of life-longsurveillance, most commonly with CTscan, must be emphasized to the patientin the preoperative discussions. Patientswhose anatomy does not fit the availablestent graft devices still require open AAArepair. Additionally, younger, healthierpatients should review the pros and consof both approaches with their vascularsurgeon when deciding between openvs. endovascular AAA repair.More recently, endovascular stentgrafting has been applied to repair ofdescending thoracic aortic aneurysms.While less common than AAA, thoracicaortic aneurysms pose similar risks ofrupture and death when larger than 5.5to 6 cm in diameter. Endovascular repairof descending thoracic aorta is nowavailable as long as major branch vesselsare not involved. Early experience withthese devices reveals an improvementin mortality and morbidity over opensurgical repair which is likely morepronounced than with the abdominalaneurysms. Moreover, there is intenseongoing investigation both to improvethese devices, as well as to extend theirindication to include aneurysm thatinvolve either the brachiocephalic orvisceral branches. At the current time,patients with an aneurysm of the thoracicaorta which is limited to the descendingportion and does not involve the majorbranches may be considered for anendovascular approach.Patients diagnosed with AAA shouldconsult with a vascular surgeon whocan best advise them about appropriatesurveillance and the latest treatmentoptions. With the increased detectionof aortic aneurysms and safer therapy,it is anticipated that fewer patients willsuffer a ruptured aneurysm with its highassociated mortality.Dr. <strong>John</strong> Moawad is a member of SummaPhysicians and Akron Vascular Associates. ■2 4 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
special section: chronic diseasesTreatment and Challengesof Chronic WoundsBy Denise Signs, <strong>MD</strong>, MS, and Lee Ann O’BrienThe skin provides an all-important barrierto the outside world. From a wound healingperspective, skin is the first line of defensefrom invading organisms. Breaks in this barrierfrom the microscopic alterations associatedwith dermatophyte infections to widespreadacute skin loss due to burns or drug reactions[e.g., toxic epidermal necrolysis] have beenassociated with invasion of microorganisms.One of the major goals of healing is to restorethe functional integrity of the skin, in part toprevent opportunities for microorganisms togain a substantial foothold.Wounds that fail to heal are often linkedto the interaction of a complicated series ofabnormalities in the wound bed and the host’sresponses to tissue injury. Factors such as infection,any condition that produces abnormalblood flow and hypoxia, cellular failure andtrauma can contribute to a chronic woundnot healing.The majority of chronic wounds — evenclean surgical wounds — are contaminated andcolonized by bacteria. Although not necessarilya problem, it is often difficult to tell when thebacterial load is acceptable or if the healing ofthe wound may become impaired due to anundesirable shift in the bacterial balance. Sincebacteria are present in all chronic wounds,a balance must be maintained between hostresistance and the quantity and virulence ofbacteria for wound healing to occur.Chronic wounds do not always behave likeacute wounds, especially when an increasedbacterial burden is present. In fact, traditionalsigns and symptoms need not be present for achronic wound to have a local infection. In thecase where 36 chronic wounds were assessedfor signs and symptoms of wound infection,investigators found that the positive correlationbetween the presence of the culture-demonstratedinfection were friable granulationtissue, an increase in odor or abnormal color,increased pain at the wound site, and woundbreakdown.Properly diagnosing the infection by takinga tissue culture from the wound or a bloodculture in patients where there is systemicinvolvement is recommended. Most studiesindicate that a tissue biopsy is the best way toWHAT GOODIS WEALTH ifyou don’t havetime to enjoy it?determine the amount of the causative organismsof a wound infection. However, diagnosisIt’s ironic. While money is often associated with freedom, the more wealth youhave, the more time you need to manage it. At the Private Client Group, wehelp you optimize and preserve wealth so you can fully experience itsadvantages. With exceptional proprietary research, local portfolio managers andexternal money managers, we can identify customized long-term opportunitiesfor you. The result: you have more of two important assets – time and wealth.To experience the Private Client Group, call Michele Pfund, Client Advisor,at 330.375.8034.WEALTH PLANNING l PRIVATE BANKINGINVESTMENTS l TRUST & ESTATE ADMINISTRATIONManaging wealth for over 160 yearsNationalCity.com/wealth©2007, National City Corporation®CS-28817See Page 34GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 25
special section: chronic diseasesDiagnosing andTreating Sleep DisordersBy Laurie Mooney, <strong>MD</strong>Sleep disorders are a topic in the publicforum fairly often these days. Patients mayeven present with specific questions aboutsleep apnea, restless legs syndrome, or othersleep disorders they have read about or seenin the news. We know much more aboutsleep disorders now than we did even a fewyears ago, and sleep disorders are now veryeasy to diagnose with sleep labs located nearmost medical facilities. The diagnostic testfor most sleep disorders is a sleep study, orpolysomnogram (PSG), where the patientspends the night at a sleep lab, sleeping in aprivate bedroom while being monitored forbreathing, snoring, sleep quality, movements,heart rhythm and oxygen levels. A sleepspecialist then makes a formal interpretationof the results, which is reported back to theprimary physician, and a follow up plan ismade. There are currently over 80 distinctsleep disorders recognized by the AmericanAcademy of Sleep Medicine (AASM)! Thesecan be as simple (but common) as inadequatehours of sleep, to as serious as stopping breathingduring sleep (sleep apnea).Sleep disorders affect 1 in 4 Americansat any given time. The more common sleepdisorders include insomnia (difficulty fallingasleep, staying asleep, or waking up tooearly), insufficient sleep syndrome, snoring,sleep apnea, restless legs syndrome, periodiclimb movements in sleep and narcolepsy.There is even a sleep disorder called “environmentalsleep disorder” in which noises,light or other external factors disrupt sleep,including a spouse’s snoring! The NationalSleep Foundation’s “Sleepiness in AmericaPoll” revealed that a snoring spouse causedan average loss of 49 minutes of sleep pernight for the non-snorer!The end result of most sleep disorders issleep deprivation. Sleep deprivation causesmany difficulties in daytime functioningsuch as poor memory, judgment and concentration,longer reaction times, accidents,depression and irritability. More recently,studies have linked sleep deprivation toweight gain through complex mechanismsinvolving hunger and fullness, cravings andglucose regulation. Sleep deprivation canalso cause headaches and worsening of painfrom all causes. Fibromyalgia, for example,is known to be exacerbated by lack of sleepor poor quality sleep.Sleep apnea, a disorder where the airwaycollapses and obstructs breathing in sleep,has been shown to have serious adversehealth consequences if untreated. Theseinclude four times increased risk of hypertensionand stroke, three times increasedrisk of heart attack, and an increased riskof arrhythmia and congestive heart failurecompared to people without sleep apnea.Untreated sleep apnea can also cause headaches,difficult to control hypertension,elevated blood glucose levels in diabetics,peripheral edema, erectile dysfunction,insomnia and nocturia.Sleep disorders affect 1 in 4 Americans at any giventime. The more common sleep disorders includeinsomnia (difficulty falling asleep, staying asleep, orwaking up too early), insufficient sleep syndrome,snoring, sleep apnea, restless legs syndrome, periodiclimb movements in sleep and narcolepsy.One of the biggest challenges in the fieldof sleep medicine is recognition of sleepdisorders. Up to 95% of sleep disordersmay be undiagnosed. People often havevague symptoms that could be explainedby other health problems or medications,or attributed to “getting older.” Symptomslike daytime sleepiness may come on verygradually, allowing a person to compensatefor it over time and therefore not notice anacute change. Some sleep disorders such assnoring, sleep apnea and leg movements insleep may only be known if there is an observer.A final, but not insignificant, obstacleto getting a diagnosis of a sleep disorderand moving on with treatment, is simply,patient acceptance. I have not infrequentlyhad patients who will openly admit that theyhave sleep apnea, but won’t agree to have thetesting done! Getting that patient buy-in fora sleep study can be very difficult. Educatingpatients about the procedure can alleviatesome of their concerns. Patients can also bedirected to your local sleep lab for specificquestions about the procedure, the cost ofthe testing and treatment, and questionsabout insurance coverage. The most importantpoint, however, should be a discussionof the long term health effects of untreatedsleep apnea and other sleep disorders.Contrary to past experience, sleep testingis now widely available in most areas of thecountry without long waiting times. Let’skeep after our patients, keep asking thosequestions about sleep, keep educating on theimportance of sleep disorders, and we willall sleep better at night!Dr. Laurie Mooney is a board-certified specialistin Internal Medicine, Pulmonary Medicine,and Sleep Medicine. She is the medical director ofthe Sleep Disorders Laboratory at WRH HealthSystem, an affiliate of Summa Health System. ■2 6 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
special section: chronic diseasesHypertension in ChildrenBy James Prebis, <strong>MD</strong>In adults, hypertension is often referredto as the “silent killer” as it is aleading cause of heart attack, stroke andchronic kidney disease. In children andadolescents, it’s better described as the“silent thief.”Pediatric hypertension won’t kill, butit will rob children of their future healthand well being. It is almost always asymptomatic.If left undiagnosed and untreated,these children and adolescents, estimatedto be between 2 and 5 percent of the pediatricpopulation, will almost certainlybecome hypertensive adults.“The Fourth Report on the Diagnosis,Evaluation and Treatment of High BloodPressure in Children and Adolescents”(Pediatrics, 2004) gives primary care physiciansclear guidelines for the measurementand interpretation of pediatric blood pressure(BP) by taking into account factors suchas age, gender and height. BP readings shouldbe taken at every well-child visit beginningat age 3. It is essential to use the correct cuffsize and get an accurate manual reading;24-hour-ambulatory BP monitoring may beneeded to rule out “white coat” hypertensionand evaluate the response to antihypertensivemedications.Patients identified as pre-hypertensive(BP=90-95 percent) should begin lifestylechanges that include weight loss,a limit on sedentary activities (“screen”time), and a low salt diet ( > 2,500 milligramsper day). It may be necessary torefer the family to supportive services,such as a pediatric weight loss programand dietitian. For example, many parentsmay assume a low-salt diet means avoidingthe salt shaker, not knowing that aone cup serving of packaged macaroniand cheese contains 1,086 milligrams ofIf left undiagnosed and untreated, these children andadolescents, estimated to be between 2 and 5 percentof the pediatric population, will almost certainly becomehypertensive adults.sodium. Other processed foods containeven more sodium.Pediatric patients diagnosed as hypertensive(BP > 95) should be referred to apediatric nephrologist, whose goals will beto determine if the patient has essential orsecondary hypertension, identify any cardiovascularrisk factors, and determine ifthere is any early end organ changes, suchas left ventricular hypertrophy.Essential hypertension is multifactoralin origin, including diet, lifestyle andgenetics. The childhood obesity epidemiccorrelates with the finding that the prevalenceof pediatric hypertension doubledbetween 1989 and 2002.Secondary hypertension results from aspecific cause, with renal disease being themost common. Other etiologies includecardiac problems, regular use of certainmedications such as steroids for asthma,oral contraceptives, over-the-counterdecongestants and illegal drugs. Childrenwho spent time in the NICU tend to be atrisk as well.Generally speaking, there is a higherrisk for secondary hypertension whenpresented with a child younger than 10years old who is thin or of average weightand has a negative family history, or whenthere is an acute rise in BP, or the patienthas stage 2 hypertension. Family history,the physical exam, lab studies, fastinglipid profiles, and echocardiograms willaid in diagnosis and the development ofa treatment plan. Less than 20 percent ofpatients with essential hypertension willrequire pharmacologic treatment.Since pediatric hypertensive patientsare rarely symptomatic we don’t alwaysappreciate the “existing” consequences.A 2006 study found that 40 to 45 percentof pediatric patients with asymptomaticessential hypertension had left-ventricularhypertrophy. Other studies have found increasedfatty streaks and fibrous plaques inthe aorta and coronary arteries of childrenwith hypertension, as well as increasedarterial stiffness, thickening of carotidintima media and arterial calcifications.Hypertension is a key factor in the“metabolic syndrome,” which puts a childat substantial risk for premature cardiovasculardisease and Type 2 diabetes. Anestimated 29 percent of U.S. adolescentswho are obese meet the definition for thissyndrome, that is, in addition to beingobese, they have two or more of the followingrisk factors: hypertension, elevatedtriglycerides, low HDL, or impaired glucosetolerance.Educating parents, children and adolescentsabout the importance of a healthylifestyle can make an impact in taming this“silent thief.” We can also reverse the tideby encouraging parents to keep up withtheir well-child visits, even throughoutthe teen years, and making sure each ofthose visits includes an accurate manualBP measurement.Dr. James Prebis is a pediatric nephrologistat Akron Children’s Hospital. ■2 8 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
special section: chronic diseasesManagement of Breast CancerBy Paul M. Ferraro, DOBreast cancer affects one in eight women.It is one of the most researched topics inmedicine treatment modalities, stimulatingconstant change in care. Current screeningguidelines state that annual mammogramsshould begin when the woman reaches 40years of age. If a patient has a family historyof breast cancer, screening should start 10years prior to the age of diagnosis of the affectedrelative.Digital mammography shows benefit inwomen greater than 50 years of age, andwith women with dense breasts who are premenopausalor perimenopausal. Ultrasoundis normally used as an adjunct to mammography.Magnetic resonance imaging (MRI)is increasing in popularity for both screeningand as adjunctive therapy, though it is moreexpensive and time consuming. Indicationsfor an MRI include additional screening inhigh risk women, women with dense breasttissue, for the evaluation of pre- and posttreatmentneo-adjunctive therapy, and forpatients with breast implants.The standard of care for biopsying bothpalpable and non-palpable breast masses haschanged from excisional biopsy to core needlebiopsy. Core needle biopsy provides an accuratehistological profile (i.e., invasive vs. insitu disease), estrogen receptor/progesteronereceptor (ER/PR) status, and HER2-NEUstatus. Attaining this information allows formore appropriate staging of breast cancer, allowingthe surgeon to discuss with the patientall available treatment options.Excisional biopsy has multiple disadvantagesover core needle biopsy. The biggestdrawback to excisional biopsy is the transactionof lymphatics compromising theaccuracy of a sentinel lymph node biopsy, ifrequired. Excisional biopsy is also associatedwith a higher rate of re-excision due to closeBreast cancer affects one in eight women. It is oneof the most researched topics in medicine treatmentmodalities, stimulating constant change in care.or transected margins. Core needle biopsycan also avoid a large scar and large volumedecrease in breast tissue for benign disease.When a biopsy comes back as cancer,staging becomes the next important task indeveloping a treatment plan for the patient.Sentinel lymph node along with possibleaxillary lymph node dissection are usedto determine how far along the cancer hasprogressed. Breast conservation therapy andmodified radical mastectomy are treatmentoptions depending on the patient’s biopsyresults and the patient’s history.Further growth in the medical communityfor the management of breast cancershould be achieved through treatment witha multi-physician approach. Genetic testingand counseling should be considered forpatients less than 40-years-old at diagnosisof breast cancer when there is a lack of familyhistory, and patients with a first degreerelative with breast or ovarian cancer. Thesurgeon should consider sending the patientto see an oncologist and/or plastic surgeonprior to surgery, helping to reduce thepatient’s anxiety and aiding in the treatmentdecision-making process. Through this collaborativeapproach, the patient can makean informed decision regarding the besttreatment plan.Dr. Paul Ferraro is a board-certified general surgeonwith a special interest in laparoscopic surgery.He is a member of the surgical staff at RobinsonMemorial Hospital. ■GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 29
special section: chronic diseasesDiagnosis and Treatment ofPeripheral Arterial DiseaseBy Jason A. Fried, DOPeripheral arterial disease (PAD) isthe manifestation of atherosclerosis.Unfortunately, atherosclerosis is a systemiccondition that not only affects the peripheralcirculation but also the coronary and cerebralcirculations. PAD is one of the most underdiagnosedmedical conditions, although itshould receive closer clinical attention due toits prevalence. Epidemiologically, peripheralarterial disease affects approximately 12% ofthe general population and 20% of patientsover 70 years of age. Special considerationshould be made in the diabetic populationbecause of the incidence reaching as high as20-25% in patients over age 50. 1Regrettably, there is no formal screeningprogram for PAD. The clinician must havea high clinical index of suspicion in order torecognize the risk factors associated withPAD. The risk factors include age over 70, diabetesmellitus, tobacco use, hyperlipidemia,hypertension, and elevated homocysteine.Peripheral arterial disease manifestsmost commonly as intermittent claudication(IC). Unfortunately, claudication maybe a very subjective complaint. A majorityof the population base with IC should beappropriately managed with conservativemedical management. But, patients whohave lifestyle inhibiting claudication, trophicchanges, and tissue loss/gangrene will mostlikely require some type of endovascular orsurgical intervention.PAD is diagnosed by the clinician whoperforms a thorough history and physicalexam. The primary screening test is an anklebrachial index. As referenced in the 2001Partners Program which screened roughly6400 patients by measurement of theirankle brachial indices, 29% of the patientswere identified with PAD. 2 If the diagnosisof PAD is made, further evaluation withnoninvasive vascular examinationwill be able to identify the arterialsegment affected. Specific evolvingtechnologies that are gainingwidespread popularity include CTangiography and MR angiography.Ultimately, the gold standard todiagnosing specific arterial segmentsis arteriography.The therapy for PAD includesan active walking program forintermittent claudication as wellas lifestyle modifications and bestmedical therapy for the risk factorsinvolved. When best medicaltherapy fails, endovascular or surgicaltherapy may be necessary. Inthe endovascular arena, multipleoptions are available. Balloonangioplasty of focal segments ofstenosis, or occlusions, is still avery viable option. Fortunately,in the armamentarium of theendovascular specialist, angioplastynow includes cryoplasty,atherectomy, covered stents, andsubintimal angioplasty for longlesions. 3In conclusion, PAD is a systemicmarker that is best screened byidentifying risk factors. Treatmentis tailored to best suit the conditionwhich the patient exhibits.When interventional therapy is required,endovascular therapy is becoming the mostcommonly offered modality by the vascularsurgeon.Dr. Jason Fried is a board-certified general surgeon,fellowship-trained in vascular surgery withspecial interests in laparoscopic and endovascularsurgery. He is a member of the surgical staff atRobinson Memorial Hospital. ■Case Study. A 68-year-old male, with hypertension,coronary artery disease, and 40-pack-per-year historyof cigarette smoking, presents with lifestyle inhibitingclaudication. His maximum walking distance was oneblock before his claudication required him to rest beforeambulating again. His ankle brachial index was 0.5. Hispre-intervention arteriogram revealed a mid-superficialfemoral artery occlusion (Figure 1). Post-angioplastyarteriogram (Figure 2) reveals a perfect angiographicresult. On clinical follow-up his claudication symptomscompletely resolved. He was continued on clopidogreltherapy and encouraged to continue a walking program.References1. Criqui MH, Fronek A, Barrett-Connor E, etal. The prevalence of peripheral arterial diseasein a defined population. Circulation 71:510-515,1985.2. Hirsch AT, Criqi MH, Treat-Jacobson D, et al.Peripheral arterial detection, awareness, andtreatment in primary care. JAMA 286:1317-1324,2001.3. Rutherford RB. Vascular Surgery 6 th Edition.Philadelphia, Elsevier Saunders, 2005.3 0 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
We’ve beenserving the areafor morethan 40 years!Come to Klein’s for AllYour Diabetes NeedsSee Our Large Selection ofDiabetic ShoesProper diabetic footwearhelps prevent sores andulcers. An active lifestyleis essential to managingdiabetes. Our therapeuticshoes are designed forboth comfort AND style.Therapeutic shoes areavailable by prescriptionthrough your doctor.Medicare and most healthinsurance plans willcover diabetic shoes andinsoles. Call us for moreinformation or to makean appointment for your special fitting!Visit our store at State Rd. and Broad Blvd. inCuyahoga Falls, or see our newest store in the Park Westbuilding, conveniently located just off I-77 at White Pond,minutes from the East, West or South.Stop in today! We have an outstanding selectionof merchandise to meet all your needs!Klein’s OrthopedicMedical Equipment2015 State Road,Cuyahoga Falls, OH 44223330.928.3720Klein’s Medical WestOne Park West Blvd.Suite 140Akron, OH 44320330.865.9000NewestLocation
special section: chronic diseasesNew Treatments forDiabetic Macular EdemaBy Joseph M. Coney, <strong>MD</strong>; Michael A. Novak, <strong>MD</strong>; and Hernando Zegarra, <strong>MD</strong>As the primary cause of serious vision lossin patients with diabetic retinopathy, diabeticmacular edema has been the nemesis of cliniciansand researchers for some time. Since thepublication of the results of the Early Treatmentof Diabetic Retinopathy Study, the only treatmentfor diabetic macular edema has been laserphotocoagulation. This treatment, however,mainly slows loss of vision, rather than restoringit. Unsatisfactory outcomes in some eyeshave prompted interest in other treatments.In efforts to find a more effective therapy,pharmacological agents such as oral proteinkinase C inhibitors, intravitreal injectionsof antibodies targeting vascular endothelialgrowth factor (VEGF), and delivery ofcorticosteroids into the vitreous cavity areunder investigation.It has been the off-label use of drugsinjected intravitreally that has been mostpromising in improving vision and possiblyretarding disease progression in patients withdiabetic retinopathy.Recently, intravitreal corticosteroid treatmentfor diabetic macular edema has generated significantinterest. The delivery route may be via eithersustained release, surgically placed intravitrealimplants or injections of corticosteroids.Although injection of intraocular steroids isnot a treatment that has been proven in largescaleclinical trials, it has become a standardtreatment option for many patients with diabeticmacular edema who have not respondedto laser treatment. In some patients who havediffuse macular edema, a steroid injection,rather than focal laser photocoagulation, maybe the first choice of treatment. In this procedure,a small amount of steroid is injecteddirectly into the eye with a tiny needle. Theoffice procedure takes about one minute toperform and is essentially painless.The rationale for the use of corticosteroidsin the treatment of diabetic macular edemastems from the observation that steroids influencemultiple pathways that contribute to thebreakdown of the blood-retinal barrier andsubsequent edema. Corticosteroids inhibitVEGF and other cytokines and growth factorsthat regulate endothelial tight cell junctions.They also reduce the synthesis of prostaglandinsand leukotrienes, two local potentinflammatory mediators.Injections of steroids into the eye have beenfound to result in very rapid resolution of themacular edema in most patients. Depending onhow long the macular edema has been present,steroid injections may result in improvement invision in some patients. Once the steroid medicationwears off (approximately 2-4 months),the macular edema may return, requiring arepeat injection or some other therapy.Case report:A 45-year-old male with a 10-year historyof non-insulin dependent diabetes mellituspresented with nonproliferative diabetic retinopathycomplicated by diffuse, clinicallysignificant macular edema without any responseto focal laser treatment. Despite havingadequate laser treatment, he continued to losevision. He was offered intravitreal triamcinoloneinjection in both eyes. Within one month,visual acuity (VA) improved from 20/40 in theright eye and 20/50 in the left eye to 20/20bilaterally. Optical coherence tomography(OCT), a noninvasive, noncontact, transpupillarytechnology that provides images ofretinal structures with resolution between 10to 17 microns, was obtained to capture thisimprovement. Foveal thickness, which is normallyabout 200 microns, improved from 881microns in the right eye and 879 microns in theleft eye to 265 microns and 288 microns, respectively,in the same interval (see figure).Similar responses have been noted withintraocular injections of anti-angiogenic drugsthat prevent blood vessels from growing andleaking. Promising results in the control of retinalneovascularization and retinal edema havebeen demonstrated. These treatments have notyet been assessed in prospective clinical trialsfor diabetic retinopathy but are being used onan off-label, non-FDA-approved basis.One particular medication that has beenincreasingly utilized for this purpose is bevacizumab(Avastin), a drug that is FDA-approvedfor the intravenous treatment of colon cancer.An intravitreal formulation was first used forthe treatment of age-related macular degeneration.Bevacizumab is a recombinant humanizedSee Page 343 2 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
New Telemonitoring ProgramMonitors Patients at HomeBy Michelle M. Morse, MSN, RNspecial section: chronic diseasesA home-based healthcare telemonitoringprogram can ideally prevent the need forcostly emergency room visits and hospitaladmissions. Remote patient monitoring alsosupports better-informed clinical decisionmaking,and actively involves patients withtheir own care. Excellent outcomes havebeen reported from home-based telemonitoringprograms.Patients enrolled in comprehensive telemonitoringprograms with equipment such asthe Philips Telemonitoring Solutions model,pictured here, spend a few minutes everyday taking one or more of their vital signmeasurements — including blood pressure,weight, oxygen saturation, pulse, and bloodglucose — using simple wireless devices inthe comfort of their own homes. Resultsare then automatically transmitted by thepatient’s “TeleStation” to a secure serverwhere registered nurses regularly reviewpatient information each day on a ClinicalReview Application.The application also allows individualizedclinician-directed health and risk assessmentsurvey questions to be sent to the patient’sTeleStation. If a patient’s vital sign measurementsare outside of parameters set by thepatient’s physician, the application triggers analert and the nurse will then call the patient tosee what is happening. For example, did theytake their medications, what is different intheir regimen, what did they eat, etc. Basedon the answers to these questions, the nursemay call the patient’s physician to get a changein a medication order or other instruction, orsend a nurse to the home for a visit.The majority of patients enrolled in ourtelemonitoring program have cardiac disease,with the leading diagnosis of heart failure.About one-third of the patients also have adiagnosis of diabetes. The interventions thathave occurred primarily stem from cardiacissues. Nearly every patient has had at leastone intervention, and one patient has hadnearly daily interventions based on the monitoringsystem results.Some of the interventions taken include:• Additional doses of diuretics for patientswith weight gain.• Additional diuretic doses for patients withincreased lower extremity edema.• Additional diuretic doses for patients whoexperienced increased shortness of breath.• Referral to their physician’s office for lowerblood oxygen level, cough and shortnessof breath. (This patient was immediatelystarted on antibiotics for bronchitis.)In most of these situations the patientswould likely have ultimately gone to theemergency room, since their symptomswould not have been treated until they deterioratedmuch further and caused even biggerproblems for the patient.This innovative technology creates awin-win situation for the patient, thefamily, and health care providers. Patientsbenefit by the early intervention of problems,thus allowing them to remain intheir homes. Physicians benefit from thetimely, regular feedback on their patient’scondition, and also the objective data uponwhich they can make better-informed interventiondecisions. The family benefitsfrom the additional reassurance that ahealth care professional is “looking after”their family member every day. The homehealth provider benefits by being able to bemore proactive in scheduling patient visitsand being in the home when needed most.This is especially critical consideringthe current and expected future nursingworkforce shortage.Michelle Morse is the Director of VisitingNurse Service and Affiliates’ (VNSA) Center forProgram Development and Education. VNSA’stelemonitoring program was funded withgrants from the GAR Foundation, the KnightFoundation and AT&T. ■PHOTO COURTESY OF PHILIPS TELEMONITORING SOLUTIONS, © 2008GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 33
Continued from Page 25is practically made by clinical examination ofthe wound’s physical and clinical characteristicsand treatment is determined by a swab cultureor biopsy.Wound bed preparation also is key to reducingthe bacterial burden of the wound. Necrotictissue, which harbors bacteria and services as aphysical barrier to wound healing, should be removed.Saline is often recommended to cleansethe wound surface. Antiseptic agents, however,are not routinely recommended [slow-releaseantiseptics such as slow-release iodine areappropriate in cases where controlling the bacterialburden is top priority] are consideredcontroversial because of concerns of toxicityto tissues. Also, systemic antibiotics maybe useful in heavily contaminated or infectedwounds.Dr. Denise Signs is board certified in InfectiousDisease and Internal Medicine and is a panel physicianat The Hyperbaric Medicine & Wound HealingCenter and an assistant professor at NortheasternOhio Universities College of Medicine (NEOUCOM).Lee Ann O’Brien is the program director at TheHyperbaric Medicine & Wound Healing Center,a National Healing Wound Center, at WoosterCommunity Hospital. ■Continued from Page 32monoclonal antibody directed against VEGF.Intraocular injections of bevacizumab haveshown promising early results, as well as anexcellent safety profile, in the control of retinalswelling and neovascularization due to a varietyof retinal conditions, including diabetic eyedisease. Bevacizumab lasts about 6 weeks in theeye after a single injection; the injection mayneed to be repeated if the disease reactivates.Intravitreal steroids and anti-VEGF drugscan be used as monotherapy, combinationtherapy, or adjunctive therapy with laser orvitreous surgery.As a result of the potential for improvementin visual acuity in an ocular condition that hasserious sight-threatening complications and fewgood treatment options, several randomizedclinical trials are underway to better define theefficacy and safety profiles of new therapies.Drs. Coney, Novak, and Zegarra are vitreoretinalspecialists with Retina Associates of Cleveland. Theiroffices are located at One Park West Boulevard inAkron, and they have privileges at Akron GeneralMedical Center. ■3 4 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
Want to increase patient referrals?Gain the attention of 4,000 local physicians through M.D. NEWS!Published every other month, M.D. NEWS offers the opportunity to• Promote your services through display advertising, and• Show your expertise through editorial.Call us today at 330-499-5332 to learn how you can gain the attention(and the patient referrals) you want.Coming up in the May-June issue of M.D. NEWS:Two Special Sections of ads and articles focused on1. Women’s Health Problems (including infertility; breast, ovarianand other cancers; women’s heart disease; obesity; etc.)2. Pain Management (including management of migraines, backpain, fibromyalgia, and other conditions).If you have expertise in one of these areas, you’ll want to be included.For information, call 330-499-5332or e-mail jan@akroncantonmdnews.com
Discovery of ElectronicallyStored InformationHow Ohio’s Proposed Civil Rules Might Affect Physician PracticesBy Joseph J. FeltesPhysicians soon may need to implementsafeguards, including modern record retentionpolicies and “Litigation Holds,” intheir offices for preserving electronicallystored records, such as emails and voicemail, as soon as a lawsuit is filed againstthem, or when they are placed on noticethat litigation or governmental investigationis likely or imminent.Approximately one year ago, newprovisions of the Federal Rules of CivilProcedure, which apply to a party’sobligation to preserve and disclose electronically-storedrecords and information,went into effect. These changes, however,applied only to litigation filed in FederalCourt. Physicians, for the most part, werenot directly affected, unless they were unluckyenough to be named as a defendantin cases alleging discrimination, antitrust,or other Federal cause of action.That is expected to change in less thansix months, when proposed amendmentsto Ohio’s Civil Rules of Procedure,which would apply to malpractice cases,are scheduled to go into effect onJuly 1, 2008.Summarizing the Proposed NewRules. The proposed new Rules aim atthe preservation and production of informationthat is electronically kept. Whilehospitals and other large institutionsundoubtedly will feel the immediate impactof these new Rules the most, at leastinitially, the aftershocks eventually willreach nearly every physician’s practice,especially as electronic medical records,emails, and Internet usage becomemore prevalent.Rule 16, as proposed, will requireattorneys representing physicians to addressat pretrial, the timing, methods ofsearch, production, and limitations (ifany) for the discovery of documents andinformation electronically stored by thephysician’s office.Consequently, physicians must be preparedto respond to an inquiry by counselabout where relevant electronically storedinformation may be kept, including networks,personal computers, laptops andsmart phones.Proposed amendments to Rule 26 expresslystate that electronically storedinformation now is fair game for discoverythrough interrogatories (Rule 33) andproduction requests (Rule 34). The Rulefurther provides that a party does notneed to produce discovery of electronicallystored information when productionimposes an undue burden or cost.It is not enough simply to claim that itwill be time-consuming or inconvenientto search for electronically stored information.The physician, through counsel,bears the burden of demonstrating, tothe court’s satisfaction, that the cost isprohibitive, compared to the potentialresults, which may be cumulative or duplicativeor whether information can beobtained through other sources that areless burdensome.In the absence of good cause, failure byphysicians to produce electronically-storedinformation in response to discovery requestspotentially could expose them tosanctions under proposed Rule 37, includingmonetary penalties, an unfavorablejury instruction, or (in extreme cases) anadverse judgment.Sp ol i at ion a nd “ L it i g at ionHolds”—Terms You Need to Know.The most severe sanctions are reservedfor cases where spoliation of evidence hasoccurred. Spoliation means the intentional,wanton, or reckless destructionof records containing relevant evidenceto litigation.A person’s duty to preserve evidence istriggered after litigation (or a governmentalinvestigation) has been commenced,or when the party is on notice thatlitigation (or governmental investigation)is imminent.In cases involving physicians, thatduty arises when the physician receivesthe summons and complaint, or (in thecontext of governmental investigations)when the physician receives a letter fromthe Office of Inspector General, theMedicare/Medicaid carrier, or from theState of Ohio Medical Board.The duty extends further to when thephysician receives a 180-day letter, whichplaces him or her on notice that a partyis contemplating filing an action arisingout of a medical claim. Some courts haveextended the duty even further, by proclaimingthat a party has a duty to preserveevidence at the moment a reasonable beliefoccurs that a person might sue. That seemsto be particularly nebulous and vague,since it seemingly would dictate that aphysician would need to preserve all electronicrecords, including emails and voicemails, whenever he or she encountered aproblem patient. Hopefully, reason andsanity will militate against imposing thatextended duty in Ohio.Rule 37 provides some hope. It statesthat a court may not impose sanctions, absentexceptional circumstances, if a partyfails to provide electronically stored informationas a result of routine, good-faithoperation of an electronic informationsystem. The Rule further states that a3 6 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
court may take into consideration the followingfactors in determining whether toimpose sanctions: (1) whether and whenany obligation to preserve information wastriggered; (2) whether the informationwas lost as a result of routine alterationor deletion of information through theordinary use of the system; (3) whetherthe party intervened in a timely fashion toprevent loss of information; (4) any stepstaken to comply with any court order orparty agreement requiring preservationof specific information; and (5) any otherfacts relevant.P r e v e n t i v e M e d i c i n e :Implementing an Effective RecordsRetention and Disposition Policy.To avoid running afoul of the new CivilRules and risking potential sanctions,physicians (from sole practitioners tolarge groups) need to implement updatedrecord retention and disposition policiesthat address, not only traditional paperrecords, but are broad enough to handleelectronically-stored information. Thesepolicies must apply to all personnel inthe office who have access to records andwho potentially could delete or otherwisedestroy them.If litigation or an investigation hascommenced, or the physician (directlyor through office personnel) is on noticethat a lawsuit or investigation may be imminent,it is necessary for the office toput into effect a “Litigation Hold,” whichinstructs all personnel not to delete ordestroy any paper or electronically-storeddocument, including emails or voicemails, that could constitute relevant evidencein the actual or pending litigationor investigation.Physicians should consult with legalcounsel to determine what kind of recordsretention and disposition policy best fitsthe practice, while assuring compliancewith Ohio’s Civil Rules.Joe Feltes is an attorney with Buckingham,Doolittle & Burroughs, LLP in Akronand Canton. ■Hyperbaric Medicine & Wound Healing CenterWooster Community Hospital1761 Beall Avenue, AnnexWooster OH 44691330-263-8750 phone • 330-263-8752 faxwww.woosterhospital.orgWooster Community HospitalYour Community, Your Hospital, Your ChoiceH E A L I N G W O U N D SI S O U R S P E C I A LT YGREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 37
3 8 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
When your patients are in needof surgical services, look to yourneighbors, Dr. Jason Fried andDr. Paul Ferraro. State-of-the-art general,laparoscopic and vascular surgical proceduresare available through five Summit andPortage County hospitals, making Dr. Friedand Dr. Ferraro convenient and accessibleto you. And, your patients will find a pleasantenvironment staffed with courteous andattentive health care professionals at bothour Akron-area and new RobinsonMemorial location in Ravenna.Join us in providing better health together.Dr. Fried and Dr. Ferraro – we’re in yourneighborhood.CONTACT INFORMATION1900 23rd StreetCuyahoga Falls, OH 442236847 North Chestnut StreetRavenna, OH 44266For Appointments, please call:(330) 926-0618Fax: (330) 926-1565
from the arhaVolunteers Needed forMedical Reserve Corps.By Marianne LoriniWith all the natural disasters and the probabilityof a biological or chemical event, we needto know we have as many medical/clinical volunteersavailable as possible. During the Akron61 N. Cleveland Massillon Rd, Suite CAkron 330-670-826333 North Ave, Suite 201Tallmadge 330-633-98077981 Hills & Dales Rd.Massillon 330-833-9411Regional Hospital Association’s PandemicFlu planning, we have become aware of thelikeliness of a large deficit of medical/clinicalhuman resources in our community. We need3812 W. Tuscarawas St.Canton 330-479-00201220 W. State Rd.Alliance 330-821-4918physicians and other clinical staff that would beable to assist with patient triage, staff palliativecare sites, and/or provide other medical needsto the homebound and others during this typeof event. Please consider volunteering for theMedical Reserve Corps (MRC).The MRC is a national, state, and local levelvolunteer group that brings health care professionalsand others together to support localpublic health, emergency and medical (hospital)services. This volunteer group is trainedand organized to assist in times of need.In the State of Ohio, there are currently78 MRC units with over 4,300 volunteersincluding physicians, physician assistants,nurse practitioners, registered nurses, LPNs,dentists, veterinarians, pharmacists, mentalhealth professionals, EMS professionals, epidemiologists,health educators, public healthprofessionals and other community membersand medical professionals.Because the Medical Reserve Corps. is notreliant on state and national resources, it meetsthe identified health needs and fills in the gaps.In order to strengthen public health and emergencyresponse infrastructures in our region,we are asking you to consider being a MedicalReserve Corps volunteer. If deployed throughthe MRC, please note that liability issues arecovered through this program.During an emergency, typical MRC dutiesinclude the augmenting of medical and supportstaff shortages at medical or shelter facilities;assisting with the distribution or dispensing ofequipment, supplies and or medication; andproviding administrative support services.When there is no emergency present, MRCduties include staffing first aid areas and communityevents, providing health care education,assisting at immunization clinics, recruitingand training volunteers, and participating invarious disaster drills and exercises.MRC needs those who have receivedmedical training, who are active in theirpractice, or those who have been retired.The need for medical, non-medical andall types of public health professionals is a4 0 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
Search Engine Optimization: Is YourWebsite Attractive to Google?By Collyn FloydemarketingWith over 100 million websites on theInternet, it may seem futile to try marketingyour website online. You may be thinking, “Isit really possible for prospective patients to findmy website?”Virtually all Internet users use a search enginelike Google or Yahoo! to find what they’relooking for. If your site is missing from the topsearch results, then you may not be maximizingyour ability to add new patients and revenue toyour practice.It may seem as if the websites appearing onthe first page of a Google search are productsof chance, but nothing could be further fromthe truth. Websites on the first page or twoof the search engine results are there becausethey are “attractive” to the search engines. Inother words, this means they were most likelyoptimized for the search engines, otherwiseknown as Search Engine Optimization.Search Engine Optimization (SEO) is theart of increasing a website’s rankings — orplacement — in the search engines. SEO makesthe pages within your site more attractive tothe search engines by adjusting their structure,programming, content, and links.The higher your website’s rankings in thesearch engine results pages, the more likelyusers will visit your site. Obviously, a site witha result on Page 1 of Google is going to get a lotmore traffic than a site on Page 8.must. Persons with no health experiencethat can help with communications, administration,logistics, and other essentialfunctions are necessary as well. Training,credentialing and services are provided.Everyone can help!To become a Medical Reserve Corps. volunteerand/or for more information, please visit www.serveohio.org.Marianne Lorini is President and CEO of theAkron Regional Hospital Association (ARHA).Member hospitals include Affinity MedicalThrough SEO, you have an entirely newchannel to reach out to potential patients andincrease the size of your practice.LOCAL SEARCHAs a physician, chances are your patientscome from a limited geographical region.That’s good news when it comes to Webmarketing. Instead of trying to compete ona national level, you can focus your efforts ona more local area. To start, there are a fewpopular sites where you’ll want to make sureyou have your practice information listed.Note that some of these sites charge a fee forinclusion:• superpages.com• Yahoo! Local• Google Local/Google Maps• yellowpages.com• local.com• citysearch.comI ALREADY HAVE AWEBSITE. WHY ISN’TIT AT THE TOP OF GOOGLE?You may have a website that’s been developedproperly. But if the site is not strategically marketed,the search engines may not be able tofind and rank the site. You may want to considerhaving your site evaluated by marketing professionalswho specialize in the online medium.from the arhaCenter; Akron Children’s Hospital; AkronGeneral Health System: Akron General MedicalCenter, Edwin Shaw Rehab, and Lodi CommunityHospital; Aultman Hospital; Medina GeneralHospital; Mercy Medical Center; RegencyHospitals (Barberton and Ravenna); RobinsonMemorial Hospital; Select Specialty Hospitalsof Akron; Select Specialty Hospital – SHS;Summa Health System: Akron City Hospital,Barberton Hospital, Cuyahoga Falls GeneralHospital, and St. Thomas Hospital; and WRHHealth System. ■A good search engine optimization firmshould target the top three search engines(Google, Yahoo! and MSN) for optimization.Together, these engines provide more than 95percent of Web traffic.They can do everything from little tweakshere and there to all-out battles for first placerankings through custom-made online marketingcampaigns. It just depends on yourbudget and how aggressive you and yourcompetition are.HOW MUCH DOES THIS COST?The good news is that SEO is incrediblyaffordable when compared to yellow pagesor print advertising. Consider also that whilea print ad confines your message to a smallspace, SEO allows you to market yourselfusing an entire website that can be updatedat any time.That’s why you should consider SEO just asimportant than your offline marketing initiatives.And like any investment, SEO will payfor itself in the end. What other marketingtool offers an average cost per lead of $0.29?(source: Entrepreneur Magazine)FINAL THOUGHTSTo give your site the Web presence itdeserves, SEO is your must-have marketingmethod. Through SEO, your site will bemade search-engine friendly so that engineslike Google and Yahoo! can find, index,and rank your site at the top. And whenthe search engines rank your site at the top,your website is exposed to throngs of searchengine users.The Karcher Group is an award-winningWeb Development, Marketing and Hosting firmlocated in North Canton. Since 1997, they’veworked with over 500 clients, from small businessesto Fortune 500 companies. For moreinformation on how Search Engine Optimizationcan help your practice, please contact PatrickQuicci at 330-493-6141 or patq @ thekarchergroup.com, or visit their website atwww.thekarchergroup.com. ■GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 41
Kids’ Health TrendsFew issues are closer to our hearts thanthe health of children. Akron Children’sHospital and its online partner, KidsHealth.org, sifted through developments affectingkids and families to identify importanttrends to watch. Below are three of them.OBESITY: BEYOND THE BODYObesity is linked to such medical conditionsas diabetes, asthma, high bloodpressure, and cancer, but its psychologicaland social consequences took center stagein 2007.One study showed that overweight kidsand teens might be the target of bias andstereotyping by their peers and teachers,and even their parents. Another showedthat obese girls were less likely to attendcollege than their peers. As these socialand psychological aspects become betterunderstood, treatment options are likely tolook beyond diet and exercise and addressthe mental components of obesity.“We need toreach k ids byage 6 or 7,” saidTroy Smurawa,M D, a spor t smedicine doctorwho workswith overweightTroy Smurawa, <strong>MD</strong>and obese childrenreferred toAkron Children’s Future Fitness Clinic.“Children who are obese by the age of 13are more than 75 percent more likely tobe obese as adults.”The fight against childhood obesity willfocus on prevention through fitness andhealthy eating strategies that are integratedinto home, school and communities. Theseefforts will take into account the psychological,social and emotional issues that playa role in obesity.BATTLING THE SUPERBUGMethicillin-resistant Staphylococcusaureus (MRSA) made frequent headlinesas the so-called “superbug” and put thespotlight on the growing threat posed bydrug-resistant bacteria.The Centers for Disease Control andPrevention has for years called antibioticresistance one of the world’s most pressingpublic health problems. Overuse ofantibiotics is a major reason bacteria haveevolved and developed resistance to drugs.The virulent strain of bacteria that resistsmany antibiotics has long been a seriousissue in hospital settings, which is stillwhere the vast majority of cases appear.But when MRSA started to show up morefrequently in the community, it becamefront-page news.Nearly a dozen Northeast Ohio schoolsports teams had outbreaks of communityacquiredMRSA (CA-MRSA) in the lastyear, but even those who do not participatein team sports arevulnerable.“ M R S A i n -fections occurmost frequentlyamong patientswith weakenedi m m u n e s y s -Blaise Congeni, <strong>MD</strong>tems,” said BlaiseCongeni, <strong>MD</strong>,director of Infectious Disease for AkronChildren’s Hospital. “During the flu season,we frequently see severe MRSA infections.Because their resistance is down due to theflu, kids can’t fight off the bacteria, whichcan sometimes lead to potentially fatalpneumonia.”Factors associated with the spread ofCA-MRSA include skin-to-skin contact,open wounds, contaminated items andsurfaces, crowded living conditions andpoor hygiene.This past year, kids and athletes across thecountry were given a crash course on loweringtheir risk of contracting MRSA, such askeeping cuts and other skin lesions coveredwith clean bandages, not sharing personalitems in the locker room, frequently washinghands, and taking a shower immediately afterpractices and games.The push to promote better hygienewill continue in 2008. What’s not clearis whether the new precautions will stickonce the headlines about a “superbug”fade. Perhaps the bigger question is, willpeople show more care in the use of antibiotics?And, if they don’t, will even morepersistent virulent bacteria appear onthe horizon?RETHINKING APILL FOR EVERY ILLNew questions about the safety and effectivenessof cough and cold medicinesmarketed for kids uncovered a truth: thefact that many of these medications havenot been tested on children.In October, drug makers pulled 14popular over-the-counter (OTC) coughand cold medicines labeled for babies andtoddlers from the market to keep parentsfrom misusing them and accidentallyoverdosing their children. One week later,a U.S. Food and Drug Administrationadvisory panel said children under 6years old should not use cough and coldmedicine such as decongestants and antihistaminesbecause their effectivenesshas not been studied in kids and the risksoutweigh the benefits.Some pediatricians see a bright side tothe development. With new questionsabout OTC drugs, parents might be alittle more reluctant to reach for a pillfor every ill, and more willing to handleeveryday sicknesses with remedies thatare always within reach — patience, restand a little tender care. The large scale ofthis recall may also prompt a louder callfor more testing of drugs on kids beforethey’re marketed for them.More kids’ health trends can be found onthis Akron Children’s Hospital Web pagehttps://www.akronchildrens.org/cms/news/83a415c56403e0f0/index.html. ■4 2 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
ACS HelpsWomenwith Cancer‘Look Good,Feel Better’Chemotherapy, radiation and otherforms of cancer treatment may change theway a woman looks and, consequently,how she feels about herself. Look GoodFeel Better is a free program offered bythe American Cancer Society (ACS),in cooperation with the Personal CareProducts Council and the NationalCosmetology Association, for womenwho are concerned about their appearancewhile undergoing cancer treatment.The program includes instructionand materials to help women regainthe confidence they had before cancertreatment began by teaching them howto improve their physical appearance.Licensed and trained cosmetologistsprovide two-hour classes on helpfultechniques related to hair, complexionand nails. All cosmetology volunteersattend a four-hour certification class tobecome program instructors.Participants receive a complimentarykit of cosmetics and beauty suppliesvalued between $250 and $300 fromreputable, well-known companies. Inall, more than 20 companies donate theirproducts to this program. Hospitals andmedical centers throughout Ohio alsosupport the program by providing a roomor area for these classes.Look Good Feel Better programs are offeredfrequently throughout the area. Registrationis required. For information about upcomingsessions, call the American Cancer Society tollfree at 1-888-227-6446, ext. 2102. ■PHOTO COURTESY OF PHILIPS TELEMONITORING SOLUTIONS, (c) 2008GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 43
the sommelierHeart of DarknessBy Natalie MacLeanWe love chocolate not just for its taste, butalso for its sensual texture. Cocoa butter, oneof its main ingredients, melts close to bodytemperature, so sliding a piece into yourmouth and feeling it seep out to coat yourtongue can almost be orgasmic. Maybe thatwhy’s the 18th century Venetian womanizerGiacomo Casanova drank chocolate daily asan aphrodisiac. Sadly, scientists have sinceproven no link between chocolate and sexualprowess, but they have discovered that itcontains phenylethylamine, a compound thatproduces a high in the brain that’s similar tothe feeling of falling in love. Is it any wonderthat women crave chocolate more than anyother food? (Men, those hopeless romantics,crave pizza.)Many oenophiles don’t even try to combinewine and chocolate, feeling that therich sweetness of chocolate is too much forany wine. But I usually buck conventionalwisdom (and I like to layer my vices), so I’mdetermined to find some good pairings. Inmatching wine with any dessert, the overarchingprinciple is that the wine must be thesweeter of the two — otherwise it’ll tastebitter or dull. That’s why chocolate, withits concentrated and creamy flavors, usuallygoes best with sweet, full-bodied, high-alcoholwines. Alcohol gives the impression ofrichness and sweetness. But there are mayshades and intensities of chocolate, so hereare a few ideas for sweetening its marriagewith wine.DARKER IS BETTERThe best partners for dark chocolateare fortified wines, such as the vin douxnaturels, banyuls and maury, both fromsouthern France. They’re made from latepickedred Grenache grapes that grow onsteep, terraced hillsides. These wines areaged up to 30 months in oak to create rich,dark fruit flavors. Banyuls is a bit sweeterand more acidic than maury, and therefore abetter match for chocolate. One of the mostfamous banyuls is Domaine du Mas Blanc,while maury is best known for Mas Amiel.Both remind me a little of California’s lateharvestzinfandel, which can also work withchocolate.Semisweet to sweet sherries have thebonus of a nutty character, which goes wellwith chocolate. Sadly, though, dry Madeirafrom the Portuguese island is a disappointment,even though it’s often grouped withsherry in the dishes it complements. Thesweet versions of this wine, such as Bual,Verdelho and malmsey, are a better matchfor chocolate.You’ll have better luck with Australianliqueur muscat and liqueur Tokay, madefrom Muscat or muscadelle grapes. They’redried to a semiraisined state on the vine,then fortified during fermentation. The wineis then heated while it’s aging in barrels,which gives it intriguing aromas of prune,fig, raisin, smoke, tar, coffee and nuts. Allgo well with chocolate. Beaumes-de-Venisemuscat from southern France has similararomas with the addition of lovely orangeblossomnotes.My favorite match for chocolate is port.Vintage port pairs well enough, with itsplum-like, grapey notes, but young rubyport is better with its aromas of blackberriesand raspberries. Best of all is tawny port,since its aromas have a natural affinity withchocolate: caramel, coffee, nuts, dried figs,cinnamon, vanilla and spice. These ports aredivine with pralines, a decadent mixture ofsugar and ground hazelnuts.Tawny ports are well-aged wines, oftenmaturing for 10, 20 or even 30 years. Asyou’d expect, the oldest variety is therichest. My favorites are Graham’s, Dow’sand Taylor Fladgate. Although colheita is avintage port because it comes from a singleyear, it’s aged in wood for at least seven years,though some are matured for more than 30years, and therefore has more tawny aromas.(Vintage port only spends two-and-a-halfyears in wood and then ages in the bottle.)Slightly less complex partners for chocolateare fruit-based dessert wines, such asframboise (raspberry) and cassis (blackcurrant).Their fruit is often macerated(soaked in alcohol) before fermentation forextra concentration. Served with chocolatecombination desserts, they complement thefruit flavors. The tannins in these wines areusually so soft that they don’t compete withchocolate, and their natural acidity workswell alongside it. I’m fond of fruit wines fromSouthbrook Winery, Ontario; and BonnyDoon Vineyards and Andrew Quady, bothfrom California. Surprisingly, apple ice wineis also lovely. Try Neige from Quebec.MILKING WINE’SPOSSIBILITIESPairing milk chocolate is a tougher challengebecause of its high dairy content, justas milky desserts such as ice cream andcheesecake also clash. Some people pair milkchocolate mousse or pudding with sparklingwine on the theory that effervescence cutsthrough the fat. But that doesn’t work forme, even with sweet bubblies like Asti orMoscato d’Asti. I find their texture too lightfor the chocolate, and the wine just tasteslike acidic metal.The best match for milk chocolate isHungarian Tokaji, with its aromas of butter,honey, apricot and citrus. Tokaji is aSee Page 464 4 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
Hang Gliding: Soaring with BirdsBy Tom Gotzysporting lifeFor those of us who have always had anaffinity for flight, who have been thrilledby the story of Icharus’ ill-fated yet fantasticalflight to the sun, hang glidingmay be the one adventure sport that mayeventually become a requirement.If just the thought of strapping on a setof wings and launching yourself into flightsends chills up your spine and adrenalinecoursing through your body … well, youowe it to yourself to try hang gliding.Hang gliding is one of the simplestforms of human flight. A hang glider is anonmotorized, foot-launched wing (kite).It is comprised of a rigid aluminum framein the shape of a triangular wing coveredwith rip-stop nylon or mylar, from whichthe pilot is suspended in a prone positionvia harness.A BIT OF HISTORYThe first recorded controlled flight ina hang glider was by a German engineer,Otto Lilienthal, who published all of hisresearch in 1889, and influenced laterdesigners. A few years later, the hangglider lost its importance to the introductionof “wing warping” by the Wrightbrothers in 1902 and the aileron controlby the French. But in 1948, an aeronauticalengineer, Francis Rogallo, invented aself-inflating wing that he later patented(1951). NASA took an interest in Rogalloinvention and tested this flexible wing asa steerable parachute for space capsulesreturning to earth.It was Barry Palmer, another aeronauticalengineer who used the “RogalloWing” to pioneer the modern day hangglider that is used commercially today. Hebuilt several versions of a foot-launchedglider utilizing different control methods,including the swing seat and control bar,which are both still in use today. Thefoot-launched idea of gliding appealed tothe freewheeling culture in the late 1960shere in America more as an expression offreedom, but its sudden commercial availabilityin the early 1970s revolutionizedhang gliding into a popular sport.ARE YOU INTERESTED?Let’s say you’re interested. The best wayto start is locating the nearest U.S. HangGliders Association (USHGA) school andenrolling in a tandem introductory flightto give you a taste of what it’s all about.Once you see what’s involved, you can signup for an introductory course. With thiselementary course, you will learn basictechniques of launching, turning and landingfrom a training hill in a matter of twodays. The length of the course is designedto compensate for weather constraints anddifferent learning curves.If after your introductory lessons, youstill want to continue, it’s best to enroll ina novice certification course, which willteach you different launching and flyingtechniques, safety procedures, etc.Typically, a student will spend five to10 lessons to obtain each of the first twoUSHGA pilot ratings (beginner and novice),a process which takes about threeto six months. At the end of the primarytraining process, the student is usuallyflying from moderate altitudes of severalhundred to a few thousand feet in relativelymild flying conditions. Progression to moredifficult flying conditions continues underthe supervision of more experienced pilots/observers and or advanced instructors.When selecting a school, first make surethat the instructors are certified by theUSHGA. Other things to look for are:• What USHGA ratings do the instructorshave? (The highest rating is calledAdvanced Tandem Instructor.)• How many instructors are at each class andwhat is the student-to-instructor ratio?• Are the flights radio supervised?• Will the training proceed gradually upprogressively higher hills?• Does the school have hills to accommodatemore than one wind direction andthus more flying days?GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 45
sporting life• What is the safety record of the schooland of the instructors?• How many students has the school taught?How many students receive certificationeach year?• Does the school operate full time to fityour schedule?WHO CAN HANG GLIDE?As the pilot of a hang glider, you controlyour aircraft via a bar. Shifting yourweight will alter the center of gravityand set you in different directions. Asyou push the bar forward, the nose ofthe hang glider is pushed up and you willgain altitude. If you pull the bar to yourchest, the nose is lowered and you willbegin to descend.Hang gliding requires a certain degree ofupper body strength and endurance. If youcan jog with a 50- to 70-lb. weight on yourshoulders, you can learn to fly. Althoughhang gliding doesn’t require great physicalstrength, on long-duration flights inturbulent weather, upper body enduranceis necessary. This typically develops as thepilot progresses in his/her training.Training facilities are located throughoutthe United States, and indeed, the world.The thrill of hang gliding is not saved forAmericans alone. Thrill seekers in Brazil,for example, enjoy some of the most precariousand thrilling flights in the worldon the cliffs outside of Rio. Or, if you everhappen to find yourself in China’s YunnanProvince, don’t be surprised to learnthat hang gliders from all over the worldfrequent this area for it’s spectacular panoramasand consistent sun exposure. Youwill even find hang gliding schools and toursavailable in the Alps.Hang gliding is an exciting way to fulfillyour dream of free flight. Once you’re inthe air, you’ll notice how peaceful freeflight is and maybe a hawk or eagle mayjoin you.If you like to watch sunsets, hang glidingis a perfect way to capture a glimpse supportedby the buoyant evening air. ■Continued from Page 44botrytised wine: The grapes on the vineare infected by a benevolent fungus calledBotrytis cinerea (also known as noble rot).This dehydrates the grapes, concentratingtheir sugars, acidity and flavors. Otherwines made this way include Sauternes fromBordeaux in France, and beerenauslesenand trockenbeerenauslesen from Germany.These wines also work well with ganacheand buttery, velvety truffles.A WHITER SHADE OF PALEWhen it comes to this sweetest of allchocolates, I admit utter defeat. It’s just toomuch for any wine. Perhaps that’s becausewhite chocolate has just 20% cocoa ascompared to the 75% in bitter chocolate.(Purists don’t consider the former to be realchocolate because it lacks all cocoa solidsexcept cocoa butter.) Its vanilla flavors pairbest with cream liqueurs from Bailey’s orStarbucks.JUST A HINT IS ENOUGHAn excellent partner with lighter dessertsthat have only a touch of chocolate, such asdipped biscotti or nut-flavored dacquoise,is amarone’s sweet cousin recioto dellavalpolicella. The grapes for both wines aredried for several months before being fermented.Those for recioto are dried a monthlonger than amarone, which gives the winea deep, sweet taste of raisins and cookedblack fruit.Canadian and German ice wine, madefrom shriveled grapes that lose their moisturebecause they’re left on the vine wellpast the fall harvest, are picked in the chill ofJanuary. Ice wine isn’t quite rich enough forpure chocolate, but it’s great with chocolatedippedfruit or a fruit flan.CHOCOLATE BUT NOT DESSERTI’ve heard that some people pair darkchocolate with such robust, dark wines.But after several sips, the wine tastes dullto me because the chocolate overpowersit. And the natural tannins in the chocolateaccentuate the wine tannins, making thesethe sommelierwines taste bitter.Lovers of both full-bodied red wines andchocolate needn’t despair, however. Withdishes featuring just a touch of bittersweetchocolate in the sauce, such as beef daube,venison stew or Mexican mole, the jammyflavors in a zinfandel, amarone, or even aCalifornian cabernet or Australian shirazwork well.A SWEET ENDINGTo gain the dark knowledge of whichwines pairs best with chocolate, I lockedmyself in my office for several long daysfilled with sugar, cocoa and alcohol.Thinking only of my trusting readers, Iam exceedingly thorough with all of myresearch. The result was a sugar-fueledhigh tempered by alcohol. (I had alsospent earlier days surrounded by moundsof lettuce, bottles of spices, grease-stainedtakeout cartons and curling cheese rinds.)However, nothing feels better than comingup with your own discoveries of what givesyou the most pleasure. Try it.To help you with your own journeythrough the world of flavor, I’ve recentlyadded an easy-to-use, online matching toolon my website (nataliemaclean.com/matcher).You can search either by wine if you’relooking for inspiration for a meal, or by foodto find great wine suggestions. There are alsorecipes from professional cooks. I’ve tried tomake the choices as comprehensive as possible,so I’ve included everything from Cajuncatfish and beef Wellington to spaghettiBolognese and potato chips. It’s still a workin progress; I keep adding to it as readers askme questions or send their favorite pairings.Of course, the best way to find good matchesis to experiment, which happily means lotsof eating and drinking. Enjoy!Natalie MacLean is the author of Red, Whiteand Drunk All Over: A Wine-SoakedJourney from Grape to Glass. She was namedthe World’s Best Drink Writer for the articles andwine picks in her free wine newsletter, available atwww.nataliemaclean.com. ■4 6 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
What’s New at Area HospitalsAffinity Medical Center offers amonthly continuing education and supportgroup for people with diabetes. Led by anurse educator or dietitian, the diabetic supportgroup features various guest speakers onimportant health and lifestyle issues affectingindividuals with diabetes and their families.The group meets from 6 to 7 p.m. on thesecond Tuesday of every month. Family andfriends are welcome to attend. Registrationis not necessary. For more information,please contact the Affinity Medical CenterEducation Services Department.Akron Children’s Hospital recentlyopened The Reinberger Family Centerdown the hall from the Neonatal IntensiveCare Unit. The 6,000 square-foot area, featurescomfortable couches and televisions,a kitchenette, computers with Internetaccess, a play area for siblings, and privateareas for families to gather for dinner or tohave one-on-one meetings with physiciansand staff. Within the Center is the SterlingJewelers Family Area. Here families haveaccess to private sleeping rooms with attachedbathrooms, private lactation roomsand laundry services.Akron General’s Office of TechnologyTransfer, Commercialization and Innovationand the Akron Global Business Acceleratorhave signed a memorandum of understandingand cooperation aimed at supporting effortsrelated to the Akron Biomedical CorridorInitiative. Through this agreement, both partiesexpress their willingness to collaborateto attract, develop and improve companies,hospital roundsproducts and services deemed useful in thebiomedical market. The goal is to promoteregional economic development opportunitieswithin Akron’s strong biomedicalresearch and development community.Alliance Community Hospital’s(ACH) main laboratory was recently awardedre-accreditation by the Commission onLaboratory Accreditation of the College ofAmerican Pathologists (CAP). CAP accreditationis determined by inspectors who examinea lab’s records and quality control practicesover the course of a two-year term, duringwhich time its staff members, qualifications,equipment, facilities and safety program/recordare also scrutinized. ACH’s lab originallyreceived CAP accreditation 20 years ago andhas been granted renewals ever since.GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008 | 47
hospital roundsAcuteCare Specialty Hospital atAultman was recently accredited by TheJoint Commission. In 2004, the AcuteCareSpecialty was established as a long-term,acute-care healthcare facility on the fourthfloor of Aultman Hospital. Centers forMedicare & Medicaid Services also accreditedthe 30-bed, not-for-profit facilitythat operates independently from AultmanHospital.Barberton Citizens Hospital is nowSumma Health System Barberton Hospital.Barberton Hospital was purchased by Summain December. The new hospital name, whichwas changed in mid January, reflects the newownership. The hospital’s signage is beingupdated accordingly.Medina General Hospital implementeda tobacco free policy in January. Theuse of tobacco is prohibited anywhere on thehospital campus, in the medical building, oron the Brunswick Campus. This includesprivate vehicles in the hospital parking lots.Upon admission, patients are informed ofthe policy. Staff will provide education topatients who smoke and offer prescriptionnicotine replacement therapy as appropriate.advertisers’ indexMedina General has promoted a smoke-freepolicy since 1989.Mercy Medical Center Homecarewas recently named among the 500 bestperforminghome health care agencies inthe U.S., placing them in the nation’s top10 percent. The 2007 HomeCare Elite list,compiled by OCS, Inc., a leading post-acutehealthcare information company, ranks themost successful Medicare-certified homehealth care providers in the United States byperformance measures in quality outcomes,quality improvement and financial performance.Compiled from publicly availableinformation, the 2007 HomeCare Elite is theonly performance recognition of its kind inthe home health industry.In January, Robinson MemorialHospital (RMH) opened the RobinsonProfessional Center on RMH’s campus inRavenna. The $14-million, 52,000-squarefootfacility includes the hospital’s EndoscopyCenter, a Pacemaker Clinic and a ChronicHeart Failure Clinic. The new ProfessionalCenter is also home to a division of NortheastOhio Cardiovascular Specialists (NEOCS)and Portage Regional Gastroenterology.Akron General Medical Center ...................................................................................................27Brookshire Financial Group .........................................................................................................8Buckingham Doolittle & Burroughs, LLP .......................................................... Inside Front CoverCBIZ ......... 34Clifford Norton Studio .................................................................................................................9CompuData ...............................................................................................................................29Drs. Hill & Thomas Co. ..............................................................................................................23Dwight Yoder Builders, Inc. ...............................................................................Inside Back CoverHanger Orthotics & Prosthetics .................................................................................................40Hyperbaric Medicine & Wound Healing Center ..........................................................................37Klein’s ....... 31Krugliak Wilkins Griffiths & Dougherty Co, L.P.A. ....................................................................47National City Private Banking Services .....................................................................................25Premiere Medical Resources .....................................................................................................39Sirak Moore ..............................................................................................................................16Summa Health System ................................................................................................. Back CoverTesta Companies .........................................................................................................................3Visiting Nurse Service & Affiliates .............................................................................................43Weidrick, Livesay, Mitchell & Burge ..........................................................................................15WRH Health System ....................................................................................................................7Added amenities include a gourmet coffeeshop and an outdoor healing garden.Summa’s Center for Behavioral HealthCare announced the creation of the Centerfor Sexual Health to provide outpatienttherapy and consultation services. TheCenter for Sexual Health provides individual,couples, and group treatment to assist patientsin achieving optimal sexual health. TheCenter specializes in the treatment of maleand female sexual dysfunction, reproductivepsychology, sexual addiction, as well ascouples counseling.Union Hospital (UH) has made availableon its website quality information related tothe its level of patient care and services in aneffort to keep local communities informed.Information about how UH compares toother hospitals is also available on the sameweb page. This information, which willbe updated on a regular basis, is the samesubmitted to the hospital’s accrediting bodyand to Medicare. To access the information,visit www.unionhospital.org, clickon “About Union Hospital” and select “AllAbout Quality.”WRH Health System’s MammographyDepartment was re-accredited for a 3-year term as a result of a survey doneby the American College of Radiology(ACR). After peer-reviewed evaluations, theDepartment was awarded accreditation forthe achievement of high practice standards.The evaluations were conducted by boardcertifiedphysicians and medical physicistswho are experts in the field. They assessedthe qualifications of the personnel and theadequacy of facility equipment.Special thanks to the hospital public relationsadministrators who submitted information for thiscolumn. To include your hospital’s news, add usto your press release list or e-mail information tojraabe@akroncantonmdnews.com. The editorialdeadline for the May-June issue of Akron/CantonM.D. News is April 2nd. ■4 8 | GREATER AKRON/CANTON M.D. NEWS MARCH-APRIL 2008
Elegant Classic HomesMeticulously Handcrafted One at a TimePORTAGE & SUMMIT COUNTIESC U S T O M H O M E B U I L D E R SC O M M E R C I A L O F F I C E C O N S T R U C T I O N330-633-7300 Akron • 330-497-6400 Canton • www.dwightyoderbuilders.com
A health systemthat offers the precisionof robotic surgeryorone that values thehuman touch?Get both when you choose Summa.We all want the same thing.Cutting-edge medicine to heal us.Caring doctors and nurses to easeour fears. Summa’s advances inminimally invasive surgery, cancerresearch and cardiac care savelives every day, while our acutecare for elders, palliative careand critical care offer familiesthe comfort of genuine caring.Summa offers everything youwant from your health system.All so you don’t have to choose.For more information, visitwww.summahealth.org.