DRAFT ADA PARATRANSIT APPLICATION - Metro Transit
DRAFT ADA PARATRANSIT APPLICATION - Metro Transit
DRAFT ADA PARATRANSIT APPLICATION - Metro Transit

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
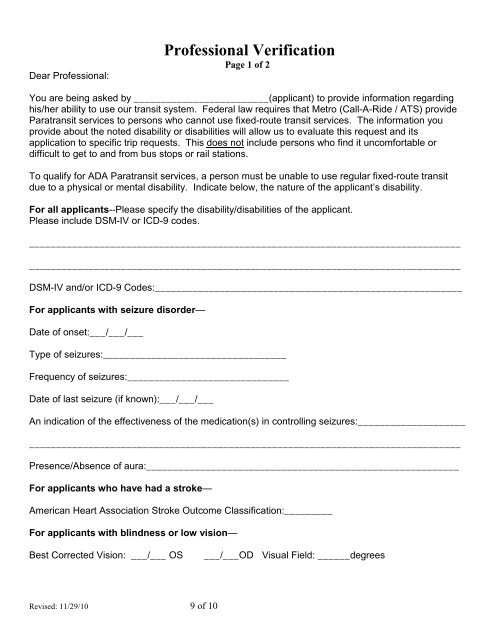
Dear Professional:Professional VerificationPage 1 of 2You are being asked by _________________________(applicant) to provide information regardinghis/her ability to use our transit system. Federal law requires that <strong>Metro</strong> (Call-A-Ride / ATS) provideParatransit services to persons who cannot use fixed-route transit services. The information youprovide about the noted disability or disabilities will allow us to evaluate this request and itsapplication to specific trip requests. This does not include persons who find it uncomfortable ordifficult to get to and from bus stops or rail stations.To qualify for <strong>ADA</strong> Paratransit services, a person must be unable to use regular fixed-route transitdue to a physical or mental disability. Indicate below, the nature of the applicant’s disability.For all applicants--Please specify the disability/disabilities of the applicant.Please include DSM-IV or ICD-9 codes.________________________________________________________________________________________________________________________________________________________________DSM-IV and/or ICD-9 Codes:_________________________________________________________For applicants with seizure disorder—Date of onset:___/___/___Type of seizures:__________________________________Frequency of seizures:______________________________Date of last seizure (if known):___/___/___An indication of the effectiveness of the medication(s) in controlling seizures:____________________________________________________________________________________________________Presence/Absence of aura:__________________________________________________________For applicants who have had a stroke—American Heart Association Stroke Outcome Classification:_________For applicants with blindness or low vision—Best Corrected Vision: ___/___ OS___/___OD Visual Field: ______degreesRevised: 11/29/10 9 of 10