The Genetic Mysteries of the Corneal Dystrophies The Genetic ...
The Genetic Mysteries of the Corneal Dystrophies The Genetic ...
The Genetic Mysteries of the Corneal Dystrophies The Genetic ...
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
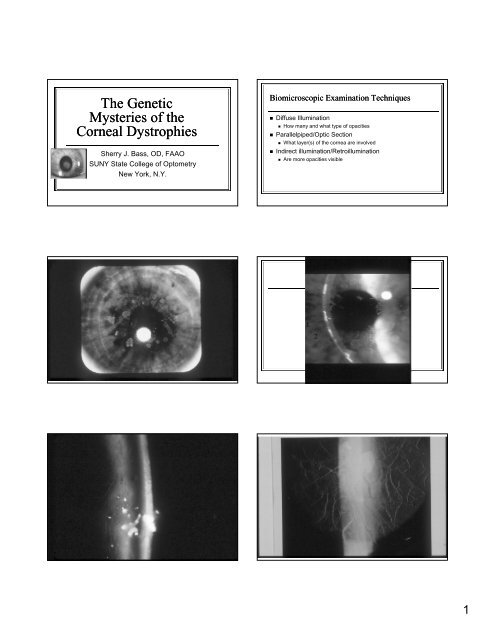
<strong>The</strong> <strong>Genetic</strong><strong>Mysteries</strong> <strong>of</strong> <strong>the</strong><strong>Corneal</strong> <strong>Dystrophies</strong>Sherry J. Bass, OD, FAAOSUNY State College <strong>of</strong> OptometryNew York, N.Y.Biomicroscopic Examination Techniques• Diffuse Illumination• How many and what type <strong>of</strong> opacities• Parallelpiped/Optic Section• What layer(s) <strong>of</strong> <strong>the</strong> cornea are involved• Indirect illumination/Retroillumination• Are more opacities visible1
Features <strong>of</strong> <strong>Corneal</strong> <strong>Dystrophies</strong> andDegenerations<strong>Corneal</strong> Degenerations (Examples)Feature Dystrophy DegenerationAge <strong>of</strong> Onset Early LateFamilial Yes NoSymmetry Symmetric AsymmetricInvolved Eye Bilateral UnilateralLocation Central PeripheralVascularity No YesInflammation No YesAssoc. disorders Rarely More frequent• Arcus senilis• Vogt’s limbal girdle• Marginal furrowdegeneration• Terrien’s degeneration• Pterygium• Salzmann’s nodulardegeneration• White ring <strong>of</strong> Coats• Band keratopathy• <strong>Corneal</strong> ectasias• Keratoconus• Non-hereditary• Pellucid MarginalDegenerationKeratoconus: Degeneration or Dystrophy?• Ectasia or thinning <strong>of</strong> <strong>the</strong> cornea-usually inferior/temporally• Hereditary in some cases• Autosomal dominant• Defective genes on chromosome 21 (SOD1 and VSX genes)• Etiology not known in non-hereditary cases-suspected causes:• eye rubbing• CL wear• Hormonal• Exacerbated by pregnancyClassification <strong>of</strong> <strong>the</strong> <strong>Corneal</strong> <strong>Dystrophies</strong>• Traditionally, classified by <strong>the</strong> affected corneal layer• Molecular genetics are changing this classification• Chromosome 1 Chromosome 4• Chromosome 5 Chromosome 9• Chromosome 12 Chromosome 16• Chromosome 17 Chromosome 20• Chromosome 21 X-chromosomeIC3D-2008 Classification <strong>of</strong> <strong>Corneal</strong><strong>Dystrophies</strong>• Category 1: well-defined; gene mapped;mutations known• Category 2: well-defined; mapped to specificchromosomal loci but gene not yet identified• Category 3: well-defined; not mapped to anychromosomal locus• Category 4: suspected corneal dystrophyEpi<strong>the</strong>lial <strong>Dystrophies</strong>• Epi<strong>the</strong>lial Basement Membrane Dystrophy(EBMD) –Map/Dot/Fingerprint or Cogan’s• Meesman’s Dystrophy• Anterior Membrane Dystrophy• Band-shaped/Whorled Microcystic Dystrophy(Lisch dystrophy)• Recurrent <strong>Corneal</strong> Erosion Dystrophy2
Epi<strong>the</strong>lial Basement Membrane Dystrophy(Map-Dot-Fingerprint Dystrophy)• Most common anterior dystrophy• Not always a true dystrophy (may be aquired asopposed to inherited)• <strong>Corneal</strong> opacities:• Maps• dots (microcysts)• Fingerprint (swirls)• bleb (putty) opacities• Painful recurrent epi<strong>the</strong>lial erosions after 3rd decadeDifferentiate from o<strong>the</strong>r etiologies <strong>of</strong>corneal whorling…• Fabry disease• X-linked recessive; 1:40,000 males ; 2:40,000 females• Enzyme deficiency=accumulation <strong>of</strong> glycosphingolipids• Systemic problems• Renal, cardiac, strokes, pain• Diagnosed with genetic testing (Genzyme)• Amiodarone <strong>the</strong>rapy• Treatment for atrial fibrillation (rapid heart beat)FABRY DISEASEAMIODARONE THERAPY3
RECURRENT CORNEAL EROSION (RCE)Meesman’s Dystrophy1. Opacities consist <strong>of</strong> epi<strong>the</strong>lial uniform grey-whitemicrocysts seen early in life2. Increase in number over time3. Relatively rare dystrophy4. Microcysts contain intracellular keratin5. RCEs are rare-may occur early in adult life whenmicrocysts rupture6. Linkage studies identify mutations in two corneaspecificgenes:K3 (chrom. 12)K12 (chrom. 17)4
Autosomal Dominant Recurrent <strong>Corneal</strong>Erosion Dystrophy• Autosomal dominant; genetic locus unknown• Attacks <strong>of</strong> RCEs usually by age 5• Subside by 30-40 years• Attacks last for a few days to months• Can be triggered by URI, dry air, lack <strong>of</strong> sleep, trauma, smoke• Subepi<strong>the</strong>lial fibrotic opacities (keloids)• Thickened subepi<strong>the</strong>lium with chondroitin and dermatan sulfate• Hudson-Stahli line• Treatment: Problematic- ointments and PTK=marginallysuccessful; rest in dark rooms during attacksBowman’s Layer <strong>Dystrophies</strong>:Reis-Buckler’s DystrophyThiel-Behnke Dystrophy• Rod or ring-shaped opacities confined to Bowman’smembrane=honey-comb or fish-net appearance• Made up <strong>of</strong> collagen fibrils;• Thickened epi<strong>the</strong>lium• Irregular astigmatism, less corneal sensation, RCEs• Vision good until later decades• PTK beneficial• Mutation maps to <strong>the</strong> Transforming Growth Factor Beta- inducedTGFBI) gene on chromosome 5 (5q31)• TGFB1 plays a role in corneal development and healing; it also interactswith collagen and o<strong>the</strong>r structural elements; it is expressed in <strong>the</strong> corneaand in o<strong>the</strong>r parts <strong>of</strong> <strong>the</strong> body.• TGFB1 mutations cause some <strong>of</strong> <strong>the</strong> stromal dystrophies as well6
Stromal <strong>Corneal</strong> <strong>Dystrophies</strong>Granular Dystrophy• Granular Dystrophy I• Lattice Dystrophy• Type I (typical)• Type II (lattice-like)• Type III, IIIA, IIIB• Type IV, V, VI, VII• Granular Dystrophy II-Avellino Dystrophy(granular + lattice)• Macular Dystrophy• Central CrystallineDystrophy <strong>of</strong> Schnyder• Fleck Dystrophy• Central Cloudy Dystrophy• Pre-Descemet’sdystrophy• Common stromal dystrophy• Opacities consist <strong>of</strong> white, round, crumb-like spotsand/or rings• Stroma in between opacities is clear early on• Good visual acuity until 7th or 8th decade when spotscoalesce and stroma between <strong>the</strong> spots is affected• Mutuation localized to <strong>the</strong> TGFBI gene on chromosome5(5q31)7
Granular Dystrophy• Opacities consist <strong>of</strong> an eosiniphilic hyaline typedeposition in <strong>the</strong> anterior stroma• Do well with PTK when VA deteriorates8
Lattice Dystrophy Type I• Opacities consist <strong>of</strong> thin, translucent lines composed <strong>of</strong>amyloid; deposits in mid-stroma• Good vision until later in life-may need PK or DALK• Changes are central but extend to <strong>the</strong> periphery overtime• Is bilateral, but can be asymmetric and unilateral• Epi<strong>the</strong>lial erosions can occur• Mutation localized to <strong>the</strong> TGFBI gene (5q31)9
Lattice Dystrophy Type II• Associated with systemic amyloidosis• Deposition <strong>of</strong> amyloid in many tissues <strong>of</strong> <strong>the</strong> body• skin• arteries• sclera• peripheral nerves• <strong>Corneal</strong> changes occur later in life• Mutation localized to <strong>the</strong> gelsolin (GSN) gene onchromosome 9 (9q34)Lattice Dystrophy Type III and IIIALater Onset Lattice <strong>Dystrophies</strong>• Type III• Thick lattice lines extendingto <strong>the</strong> periphery• Occurs later in life• Inheritance pattern isautosomal recessive• No recurrent epi<strong>the</strong>lialerosions• Mutation is on <strong>the</strong> TGFBIgene on chromosome 5-same site (5q31)• Type IIIA• Autosomal dominant• Recurrent epi<strong>the</strong>lial erosions• Same phenotypicpresentation as Type III butdifferent mode <strong>of</strong> inheritanceand corneal erosionsProminent amyloid deposition posterior to Bowmans layerLattice Dystrophy Type IV• Ano<strong>the</strong>r late-onset lattice dystrophy• Deep stromal opacities made <strong>of</strong> amyloid• Mutation localized to <strong>the</strong> TGFBI gene on chromosome 5(5q31)• <strong>The</strong> list <strong>of</strong> late-onset lattice dystrophies goes on and onand on…• Types V, VI and VII have been described, based on• <strong>the</strong> pattern <strong>of</strong> lattice lines• mutation sites and defective genes• pedigree11
Combined Granular and Lattice Dystrophy(Avellino Dystrophy)• Granular and lattice type changes in <strong>the</strong> same eye• Hyaline and amyloid deposits in stroma• Granular changes early onset; lattice changes occurlater• Good vision in early stages• Both granular and lattice mutations are on <strong>the</strong> samegene (TGFBI), so is not surprising to find bothphenotypic presentations in one individualMacular Dystrophy• Autosomal recessive• Early onset• Vision more severelyaffected than in o<strong>the</strong>rstromal dystrophies• Characterized by stromalhaze, and milky whiteopacities(glucosaminoglycans)• Progresses to cornealperiphery by ages 20-30• By age 40, PK may berequired• Mutation localized to <strong>the</strong>carbohydratesulfotransferase (CHST6)gene on chromosome 16(16q22)12
Central “Crystalline” Dystrophy <strong>of</strong>Schnyder• Characterized by centralstromal cholesterol andphospholipid deposits,sometimes with an arcus• Only 50% have “crystals”• Visual acuity onlyreduced if opacities aredense and central• Ano<strong>the</strong>r rare dystrophyassociated with asystemic disorder• Rule out hyperlipidemia• Mutation (N102S) onshort arm <strong>of</strong> chromosome1 (1p34-36) <strong>the</strong> UBIAD1gene• Plays a role in cholesterolmetabolism13
Fleck Dystrophy• Subtle grey opacities consist <strong>of</strong> small, wreath-likeopacities in <strong>the</strong> stroma• Represent engorged keratocytes• Usually asymptomatic• Cases with photophobia , ocular surface irritation andblepharospasm have been recently reported• Opacities extend to <strong>the</strong> periphery• Visual acuity good throughout life since stroma betweenflecks remains clear• Maps to chromosome 2 (2q35)14
Pre-Descemets Dystrophy• Fine, deep white posterior stromal opacities• Lie anterior to Descemets membrane• Autosomal dominant• No effect on visual acuityCentral Cloudy Dystrophy <strong>of</strong> Francois• Central opacity in stroma looks like cracked-iceor crocodile skin; glycosaminoglycan deposition• Visual acuity is usually normal• Appearance similar to crocodile shagreen, anage-related corneal change resulting in posteriorstromal deposition• Difficult to differentiate from crocodile shagreenin <strong>the</strong> late course <strong>of</strong> disease, especially ifbilateral15
Endo<strong>the</strong>lial <strong>Dystrophies</strong>• Fuch’s Dystrophy• Posterior Polymorphous Dystrophy• Congenital Hereditary Endo<strong>the</strong>lial Dystrophy(CHED)Fuch’s Endo<strong>the</strong>lial Dystrophy• Characterized by threestages• guttata- localizedexcresences or thickeningsin Descemet’s membrane• stromal and epi<strong>the</strong>lialedema• corneal fibrosis or scarring• Results in corneal edema,usually greatest uponawakening• Women affected morefrequently than men• Affects older individuals,greater than 40 years• Early onset Fuch’sdystrophy mapped tochromosome 116
Treatment <strong>of</strong> Fuch’s Dystrophy• Monitor• If edema is present, treat with hyperosmoticagents, e.g. Muro 128• Hair dryer may be helpful in <strong>the</strong> AM• Watch <strong>the</strong> ocular hypertensive• If IOPs elevated, treat to lower IOP to reduce edema• In later stages, PK or DSAEK may be required• What about Fuch’s dystrophy and cataract?17
Posterior Polymorphous Dystrophy• Isolated and coalesced posterior vesicles• Wide areas <strong>of</strong> thickening <strong>of</strong> Descemet’smembrane• bandlike figures and lines• Diffuse stromal and epi<strong>the</strong>lial edema• Peripheral anterior synechiae18
Posterior Polymorphous Dystrophy• Treatment similar to Fuch’s dystrophy• Mutation is in <strong>the</strong> COL8A gene in <strong>the</strong> 20q11locus (long arm <strong>of</strong> chromosome 20) in somecases• O<strong>the</strong>r cases have mutations in chromosome 1Congenital Hereditary Endo<strong>the</strong>lialDystrophy (CHED 1)• Autosomal dominant• Manifests as diffuse corneal edema a few years afterbirth• May be associated with hearing loss• Photophobia, tearing• Is progressive• Mutation for CHED1 has also been mapped to 20p11-20q11 on chromosome 20-overlaps <strong>the</strong> location <strong>of</strong> <strong>the</strong>mutation causing PPD!Congenital Hereditary <strong>Corneal</strong>Dystrophy (CHED 2)• Autosomal recessive• Central corneal edema from birth• Nystagmus• Non-progressive but more severe edema thanCHED119
Summary <strong>of</strong> <strong>the</strong> Molecular <strong>Genetic</strong>s <strong>of</strong> <strong>the</strong><strong>Corneal</strong> <strong>Dystrophies</strong>• Meesmann’s• KRT 3, KRT 12 genes onchromosomes 12, 17• Lisch (Whorled)• Unidentified gene on Xchromosome• Reis-Buckler’s Granular Type III)• TGFBI gene on chromosome 5• Granular Dystrophy• TGFBI chromosome 5• Lattice I,III,IV, V, VI, etc.• TGFBI,chromosome 5• Lattice II• GSN,chromosome 9• Macular Dystrophy• CHST6 gene,chromosome 16• Crystalline Dystrophy• Gene ? chromosome 1• Fuch’s Dystrophy• PPD and CHED• COL8A gene on chromosome20• Chromosome 1Courtesy: Redatlas.orgConsider Classification by AffectedChromosomeImplications <strong>of</strong> Molecular <strong>Genetic</strong>sfor <strong>the</strong> Future• Chromosome 1 <strong>Dystrophies</strong>• Central crystalline dystrophy• Early onset Fuch’s dystrophy• Posterior polymorophous dyst• Chromosome 2 <strong>Dystrophies</strong>• Fleck dystrophy• Chromosome 5 <strong>Dystrophies</strong>• Lattice dystrophy (Types 1 andIIIA)• Granular dystrophy• Avellino dystrophy (GCDII)• Reis-Buckler’s dystrophy (GCDIII)• Chromosome 9 <strong>Dystrophies</strong>• Lattice dystrophy Type II• Chromosome 12 <strong>Dystrophies</strong>• Meesman dystrophy (and 17)• Chromosome 16 <strong>Dystrophies</strong>• Macular corneal dystrophy• Chromosome 20 <strong>Dystrophies</strong>• Congenital Hereditary Endo<strong>the</strong>lialDystrophy Types I and II• Posterior Polymorphous Dyst• Chromosome 21 <strong>Dystrophies</strong>• A/D Keratoconus• X-chromosome <strong>Dystrophies</strong>• Lisch corneal dystrophy• Knowledge <strong>of</strong> mutations enables researchers toidentify <strong>the</strong> pathways that syn<strong>the</strong>size abnormalproteins which are deposited in <strong>the</strong> cornea• This knowledge can lead to <strong>the</strong> development <strong>of</strong>new drugs designed to interfere with <strong>the</strong>sepathways to decrease abnormal proteinsyn<strong>the</strong>sis• Less deposition = less affect on vision = less Tx20