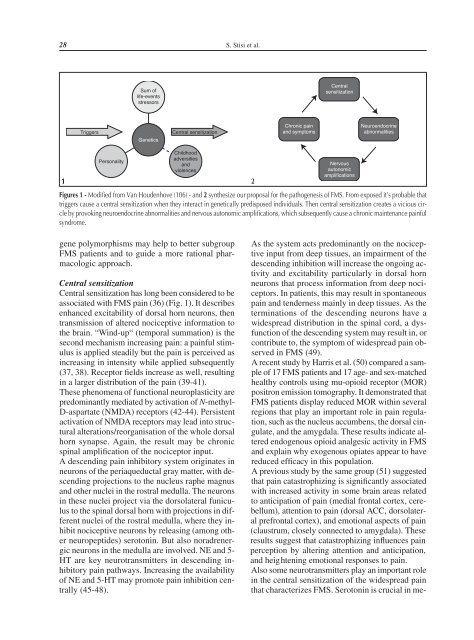
28 S. Stisi et al.Sum oflife-eventsstressorsCentralsensitizationTriggersGeneticsCentral sensitizationChronic painand symptomsNeuroendocrineabnormalitiesPersonalityChildhoodadversitiesandviolences1 2NervousautonomicamplificationsFigures 1 - Modified from Van Houdenhove (106) - and 2 synthesize our proposal for the pathogenesis of FMS. From exposed it’s probable thattriggers cause a central sensitization when they interact in genetically predisposed individuals. Then central sensitization creates a vicious circleby provoking neuroendocrine abnormalities and nervous autonomic amplifications, which subsequently cause a chronic maintenance painfulsyndrome.gene polymorphisms may help to better subgroupFMS patients and to guide a more rational pharmacologicapproach.Central sensitizationCentral sensitization has long been considered to beassociated with FMS pain (36) (Fig. 1). It describesenhanced excitability of dorsal horn neurons, thentransmission of altered nociceptive information tothe brain. “Wind-up“ (temporal summation) is thesecond mechanism increasing pain: a painful stimulusis applied steadily but the pain is perceived asincreasing in intensity while applied subsequently(37, 38). Receptor fields increase as well, resultingin a larger distribution of the pain (39-41).These phenomena of functional neuroplasticity arepredominantly mediated by activation of N-methyl-D-aspartate (NMDA) receptors (42-44). Persistentactivation of NMDA receptors may lead into structuralalterations/reorganisation of the whole dorsalhorn synapse. Again, the result may be chronicspinal amplification of the nociceptor input.A descending pain inhibitory system originates inneurons of the periaqueductal gray matter, with descendingprojections to the nucleus raphe magnusand other nuclei in the rostral medulla. The neuronsin these nuclei project via the dorsolateral funiculusto the spinal dorsal horn with projections in differentnuclei of the rostral medulla, where they inhibitnociceptive neurons by releasing (among otherneuropeptides) serotonin. But also noradrenergicneurons in the medulla are involved. NE and 5-HT are key neurotransmitters in descending inhibitorypain pathways. Increasing the availabilityof NE and 5-HT may promote pain inhibition centrally(45-48).As the system acts predominantly on the nociceptiveinput from deep tissues, an impairment of thedescending inhibition will increase the ongoing activityand excitability particularly in dorsal hornneurons that process information from deep nociceptors.In patients, this may result in spontaneouspain and tenderness mainly in deep tissues. As theterminations of the descending neurons have awidespread distribution in the spinal cord, a dysfunctionof the descending system may result in, orcontribute to, the symptom of widespread pain observedin FMS (49).A recent study by Harris et al. (50) compared a sampleof 17 FMS patients and 17 age- and sex-matchedhealthy controls using mu-opioid receptor (MOR)positron emission tomography. It demonstrated thatFMS patients display reduced MOR within severalregions that play an important role in pain regulation,such as the nucleus accumbens, the dorsal cingulate,and the amygdala. These results indicate alteredendogenous opioid analgesic activity in FMSand explain why exogenous opiates appear to havereduced efficacy in this population.A previous study by the same group (51) suggestedthat pain catastrophizing is significantly associatedwith increased activity in some brain areas relatedto anticipation of pain (medial frontal cortex, cerebellum),attention to pain (dorsal ACC, dorsolateralprefrontal cortex), and emotional aspects of pain(claustrum, closely connected to amygdala). Theseresults suggest that catastrophizing influences painperception by altering attention and anticipation,and heightening emotional responses to pain.Also some neurotransmitters play an important rolein the central sensitization of the widespread painthat characterizes FMS. Serotonin is crucial in me-
Etiopathogenetic mechanisms of Fibromyalgia Syndrome 29diating pain pathways; it was the first neuropeptideto be studied extensively in FMS and hypothesizedto be involved in abnormal pain processing (52,53). The co-morbidity of psychiatric conditions,such as depression, and the alterations of sleepwakecycles, mediated by 5-HT, seemed to support5-HT dysregulation (54).Levels of 5-HT, its precursor tryptophan, and itsmetabolites 5-HIAA and 5-HTP were measured inthe blood, in the cerebrospinal fluid (CSF), and inthe urine of FMS patients. The most consistent resultsof all attempts to confirm an abnormality in5-HT neurotransmission were derived from CSFsamples. The pioneering studies did not measure 5-HT directly but found decreased levels of 5-HIAAin FMS patients as compared to controls, includingboth pain-free and low back pain subjects (55-57). The results from studies measuring 5-HT levelsin the serum of patients with FMS were lessconsistent. One group documented higher 5-HTlevels in FMS patients versus controls (58), evenusing platelet-rich plasma for the assay, whereasanother group found lower serum 5-HT levels inFMS than in RA patients (54). The hypothesis wasthat increased platelet activation may lead to a releaseof 5-HT into the plasma fraction. FMS patientswith a high plasma-to-serum 5-HT ratio presentedwith a higher frequency of orofacial painand anxiety (59). Similarly in another study, thenumber of tender points and serum 5-HT levelssignificantly correlated inversely, comparing FMSpatients with both RA patients and healthy controls(52). Whether or not the inconsistency may beexplained by changes within the serotonin transporterhas been discussed. A polymorphism in the5-HT transporter gene regulatory region (S/S genotype)is associated with decreased 5-HT transportermessenger RNA transcription and decreased 5-HTuptake in vitro. As mentioned previously, this polymorphismhas been shown to have a significantlyhigher distribution in FMS cohort (29).To summarize, a dysregulation of 5-HT metabolismin FMS is likely but has not been proven to bethe sole cause of central sensitization of FMS.Substance P, an 11-amino-acid neuropeptide, actsas a neuromodulator via the NK1 receptor. It sensitizesthe neurons to the effects of other neuromodulators.Stimulating the release of 5-HT in thespinal cord decreases the release of substance P intothe spinal cord (60).Substance P levels in the CSF of FMS patients havebeen found to be reproducibly high in five differentstudies (61-64). A trend toward correlation ofCSF substance P levels and pain severity in FMSover time has been suggested (65). Other chronicpain states, such as low back pain and painful neuropathy,present with low levels of CSF substanceP (66-69). High CSF concentration of substance Prepresents the most prominent neurochemical abnormalityfound in FMS patients.There are significant negative correlations betweenlevels of substance P and 5-HT, its precursor tryptophan(TRP), and its primary metabolite 5-HIAAin the serum of patients with FMS. High serumconcentrations of 5-HIAA and TRP showed a significantrelation to low pain scores. Low levels of5-HIAA and high concentrations of substance Pwere both positively correlated with more severesleep disturbance (70). Nerve growth factor (NGF),which stimulates the production of substance P insmall, afferent, unmyelinated neurons, was foundto be elevated in the CSF of FMS patients with primaryFMS, but not in FMS with an associatedpainful inflammatory condition (secondary FMS)(71). This finding addresses the clinical finding ofsubgroups in FMS (72-74). Elevated CSF substanceP could be a common link between primaryand secondary FMS, but the groups differ withregard to the mechanism responsible for the elevatedsubstance P. In primary FMS, NGF seems toinduce the elevated CSF substance P from centralinterneurons. In secondary FMS, the peripheral inflammation,so characteristic of the underlyingrheumatic or infectious conditions, may be responsiblefor the elevated CSF substance P. Forthese reasons, NGF could be critical to the initiationor perpetuation of the painful symptoms ofprimary but not secondary FMS (71).Neuroendocrine abnormalitiesThe neuroendocrine system, together with the autonomicnervous system and immune system, playsa fundamental role in the maintenance of the homeostasisof the organism in a large variety of environmentalsituations, namely stressful events ofboth physical and psychological origin. FMS is frequentlyassociated with a rich history of stressful/traumaticevents (75) and is characterized by anumber of symptoms similar to those typical ofstress-related conditions, such as irritable bowelsyndrome or chronic fatigue syndrome.The hypothalamic-pituitary-adrenal axis(HPA-axis)FMS patients have been shown to present withHPA axis alterations (76-80). Compared to con-
- Page 2 and 3: 2 P. Sarzi-Puttini et al.The meetin
- Page 4 and 5: 4 M. Cazzola et al.(2). In the earl
- Page 6 and 7: 6 M. Cazzola et al.enough to meet F
- Page 8 and 9: 8 M. Cazzola et al.Table I - Charac
- Page 10 and 11: 10 M. Cazzola et al.Table IV - Cond
- Page 12 and 13: 12 M. Cazzola et al.teria, three su
- Page 14 and 15: 14 M. Cazzola et al.tients with a n
- Page 16 and 17: 16 G. Cassisi et al.The cardinal fe
- Page 18 and 19: 18 G. Cassisi et al.StiffnessIn FM
- Page 20 and 21: 20 G. Cassisi et al.Autonomic and n
- Page 22 and 23: 22 G. Cassisi et al.Associated symp
- Page 24 and 25: 24 G. Cassisi et al.46. Coleman RM,
- Page 26 and 27: 26 S. Stisi et al.sensitization,”
- Page 30 and 31: 30 S. Stisi et al.trols, they prese
- Page 32 and 33: 32 S. Stisi et al.stress, obtained,
- Page 34 and 35: 34 S. Stisi et al.50. Harris RE, Cl
- Page 36 and 37: ORIGINAL ARTICLEReumatismo, 2008; 6
- Page 38 and 39: 38 F. Atzeni et al.lalanine (17), a
- Page 40 and 41: 40 F. Atzeni et al.clearer and it m
- Page 42 and 43: 42 F. Atzeni et al.healthy control
- Page 44 and 45: 44 F. Atzeni et al.and/or verbal (e
- Page 46 and 47: 46 F. Atzeni et al.for study purpos
- Page 48 and 49: 48 F. Atzeni et al.mimics of fibrom
- Page 50 and 51: ORIGINAL ARTICLEReumatismo, 2008; 6
- Page 52 and 53: 52 P. Sarzi-Puttini et al.A larger
- Page 54 and 55: 54 P. Sarzi-Puttini et al.from 1966
- Page 56 and 57: 56 P. Sarzi-Puttini et al.rational,
- Page 58 and 59: 58 P. Sarzi-Puttini et al.49. Toffe
- Page 60 and 61: 60 R. Casale et al.cal exercise and
- Page 62 and 63: 62 R. Casale et al.definition of
- Page 64 and 65: 64 R. Casale et al.are more or less
- Page 66 and 67: 66 R. Casale et al.trol associated
- Page 68 and 69: 68 R. Casale et al.32. Lewit K. The
- Page 70 and 71: ORIGINAL ARTICLEReumatismo, 2008; 6
- Page 72 and 73: 72 L. Altomonte et al.In a clinical
- Page 74 and 75: 74 L. Altomonte et al.Table II - We
- Page 76 and 77: 76 L. Altomonte et al.treatments de