

1813 01 REUMA3 Editoriale - ME/CFS Australia
1813 01 REUMA3 Editoriale - ME/CFS Australia
1813 01 REUMA3 Editoriale - ME/CFS Australia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
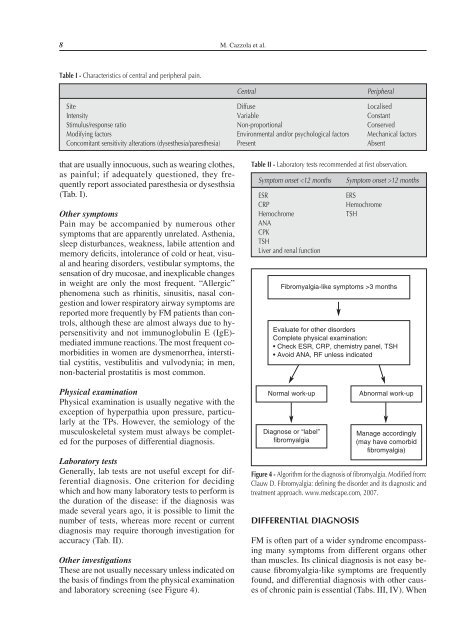
8 M. Cazzola et al.Table I - Characteristics of central and peripheral pain.CentralPeripheralSite Diffuse LocalisedIntensity Variable ConstantStimulus/response ratio Non-proportional ConservedModifying factors Environmental and/or psychological factors Mechanical factorsConcomitant sensitivity alterations (dysesthesia/paresthesia) Present Absentthat are usually innocuous, such as wearing clothes,as painful; if adequately questioned, they frequentlyreport associated paresthesia or dysesthsia(Tab. I).Other symptomsPain may be accompanied by numerous othersymptoms that are apparently unrelated. Asthenia,sleep disturbances, weakness, labile attention andmemory deficits, intolerance of cold or heat, visualand hearing disorders, vestibular symptoms, thesensation of dry mucosae, and inexplicable changesin weight are only the most frequent. “Allergic”phenomena such as rhinitis, sinusitis, nasal congestionand lower respiratory airway symptoms arereported more frequently by FM patients than controls,although these are almost always due to hypersensitivityand not immunoglobulin E (IgE)-mediated immune reactions. The most frequent comorbiditiesin women are dysmenorrhea, interstitialcystitis, vestibulitis and vulvodynia; in men,non-bacterial prostatitis is most common.Physical examinationPhysical examination is usually negative with theexception of hyperpathia upon pressure, particularlyat the TPs. However, the semiology of themusculoskeletal system must always be completedfor the purposes of differential diagnosis.Laboratory testsGenerally, lab tests are not useful except for differentialdiagnosis. One criterion for decidingwhich and how many laboratory tests to perform isthe duration of the disease: if the diagnosis wasmade several years ago, it is possible to limit thenumber of tests, whereas more recent or currentdiagnosis may require thorough investigation foraccuracy (Tab. II).Other investigationsThese are not usually necessary unless indicated onthe basis of findings from the physical examinationand laboratory screening (see Figure 4).Table II - Laboratory tests recommended at first observation.Symptom onset 12 monthsERSHemochromeTSHFibromyalgia-like symptoms >3 monthsEvaluate for other disordersComplete physical examination:• Check ESR, CRP, chemistry panel, TSH• Avoid ANA, RF unless indicatedNormal work-upDiagnose or “label”fibromyalgiaAbnormal work-upManage accordingly(may have comorbidfibromyalgia)Figure 4 - Algorithm for the diagnosis of fibromyalgia. Modified from:Clauw D. Fibromyalgia: defining the disorder and its diagnostic andtreatment approach. www.medscape.com, 2007.FM is often part of a wider syndrome encompassingmany symptoms from different organs otherthan muscles. Its clinical diagnosis is not easy becausefibromyalgia-like symptoms are frequentlyfound, and differential diagnosis with other causesof chronic pain is essential (Tabs. III, IV). When













