2010 Annual Report - Regional West Medical Center
2010 Annual Report - Regional West Medical Center
2010 Annual Report - Regional West Medical Center

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CANCER TREATMENT CENTER<strong>2010</strong> <strong>Annual</strong> <strong>Report</strong>ICANCER TREATMENTCENTER
For Additional Copies| Call308.630.2421| Write<strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong>Cancer Treatment <strong>Center</strong>3911 Avenue B | Suite G100Scottsbluff, NE 69361Attention: Cindy Keller, CTRCancer Registry Coordinator| EmailKellerc@rwmc.netAccess the report at www.rwhs.org<strong>2010</strong> <strong>Annual</strong> <strong>Report</strong> published October 2011Teresa Clark, Editor2
Table of contentsIntroduction 2<strong>2010</strong> Accomplishments and Activities 32011 Goals 4Cancer Support Services 5‐6Cancer Support Groups 7‐8Cancer Conference 9Cancer Registry 10Cancer Committee Membership 11Physician Liaison <strong>Report</strong> 13<strong>2010</strong> Comparison of Cancer Data 14Primary Site Table 15Reconstructive Surgery after Breast Cancer 16‐17Accelerated Partial Breast Irradiation 18Breast Cancer 18Breast Cancer Graphs 19‐20On-site <strong>Medical</strong> Physicist 23‐24Glossary of Terms 253
“Our team of professionals isdedicated to offering ‘best practices’and compassionate care to westernNebraska and surrounding communities.”‐Carol Willis, MDChairman, Cancer Committee11
IntroductionBreast cancer is the focus of this year’s annual report.Worldwide, breast cancer is the most frequently diagnosedlife-threatening cancer in women and the leading causeof cancer death among women. Over the past 25 years,breast cancer incidence rates have risen globally, with thehighest rates in western countries. Reasons for this trendinclude change in reproductive patterns, increased screening,dietary changes, and decreased activity.Although breast cancer incidence is on the rise globally,breast cancer mortality has been decreasing, especiallyin industrialized countries. The 2002 international femalebreast cancer incidence rates varied by more than 25-fold,ranging from 3.9 cases per 100,000 in Mozambique to101.1 cases per 100,000 in the United States. In 2008, theAmerican Cancer Society (ACS) estimated there were nearly1.4 million new cases of invasive breast cancer worldwide.In the United States, approximately 207,090 new cases offemale invasive breast cancer were predicted to occur in<strong>2010</strong>, along with 1,970 cases in men. In addition to invasivebreast cancer, 54,010 new cases of in situ breastcancer were expected to occur among women, of whichapproximately 85 percent were expected to be ductal carcinomain situ (DCIS).After two decades of increasing incidence rates, the numberof new female breast cancers decreased by 2.2 percentper year from 1999 to 2005. This decrease is thoughtto reflect reduced use of hormone replacement therapy(HRT) following the publication of the Women’s Health Initiativesfindings in 2002, which linked HRT use to an increasedrisk of heart disease and breast cancer. Rates ofDCIS have stabilized since 2000.The current lifetime risk of breast cancer in the US isestimated at 12.7 percent for all women, 13.3 percentfor non-Hispanic whites, and 9.98 percent for blackwomen. Overall, the annual incidence rates in blackwomen (119.4/100,000) and Hispanic/Latina women(89.9/100,000) have been stable since the early 1990s,and they are lower than the annual incidence of breastcancer in white women (141.1/100,000). However, blackwomen are more likely than white women to be diagnosedwith larger, advanced-stage tumors (>5 cm).Many early breast carcinomas may be asymptomatic; painor discomfort is not usually a symptom of breast cancer.Breast cancer is often first detected as an abnormality ona mammogram before it is felt by the patient or health careprovider. The general approach to evaluation of breast cancerhas become formalized as triple assessment: clinicalexamination, imaging (usually mammography and/or ultrasonography),and needle biopsy. Surgery is consideredprimary treatment for breast cancer. Many patients withearly-stage breast cancer are cured with surgery alone.Increased public awareness and improved screening haveled to earlier diagnosis, at stages amenable to completesurgical resection and curative therapies. Consequently,survival rates for breast cancer have improved significantly,particularly in younger women.Adjuvant treatment of breast cancer is designed to treatmicrometastatic disease, or breast cancer cells that haveescaped the breast and regional lymph nodes but whichhave not yet had an established identifiable metastasis.Depending on the model of risk reduction, adjuvant therapyhas been estimated to be responsible for 35-72 percentof the reduction in mortality rate. Over the last twodecades, breast cancer research has led to extraordinaryprogress in our understanding of the disease, resulting inmore efficient and less toxic treatments.<strong>Regional</strong> <strong>West</strong>’s cancer treatment program is committedto early diagnosis of breast cancer, advanced treatmentregimens, and aggressive prevention strategies. Our teamof professionals is dedicated to offering `best practices’and compassionate care to western Nebraska and surroundingcommunities. We could not do this without thehelp of the tireless effort of physicians, nurses, radiationtherapists, social workers, nutritionists, and support staff.Carol Willis, MDChairman, Cancer CommitteeReferences:http://emedicine.medscape.com/article/1947145-overview#a01562
<strong>2010</strong> <strong>Regional</strong> <strong>West</strong>andCancer ProgramAccomplishments Activities• Implemented partial breast irradiation utilizing (HDR)High Dose Brachytherapy.• Added second MRI; this scanner will be open bore toreduce sedation of patients and give us the ability toscan larger patients.• Added one additional portable X-ray unit to providediagnostic X-ray services to inpatients, EmergencyDepartment, and surgery patients.• Added a second ultrasound unit to increase capacityfor ultrasound at the Breast Health <strong>Center</strong>.• Increased the number of “Look Good Feel Better”sessions held during the year.• Purchased a new U/S unit for use in prostate seedimplants and Partial Breast Irradiation.• Improved post surgical education and managementof PEG and J-Tube placement; continueddevelopment of in-house specialists for this service.• Researched and developed the necessaryrequirements for forming a Palliative Care Teamhere at <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong>.• Conducted “A Time to Heal” program for breastcancer patients.33
2011 GoalsCancer Treatment <strong>Center</strong> andDorwart Cancer Care <strong>Center</strong>• MRI guided breast biopsies.• Conduct “A Time to Heal” program for breast cancerpatients at Dorwart Cancer Care <strong>Center</strong>.• Increase “Reach to Recovery” referrals.• Initiate CT-virtual colonoscopy screening exam.• Expand PET/CT to provide an additional day everyother week due to increased patient volume.• Improve post surgical education and management ofPEG and J-Tube placement; continue development ofin-house specialists for this service.• Increase clinical trial enrollment for qualifying patients.• Create a Survivorship Team consisting of patientnavigation, dietary, social work, physical therapy,occupational therapy, and other supportive servicesas necessary in order to improve the entire patientexperience.• Work with <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> MarketingDepartment to develop a comprehensive CancerProgram marketing campaign (print, TV, and website).• Continue work towards NAPBC Accreditation (Breast<strong>Center</strong> of Excellence).4
Cancer Support ServicesCommunity Outreach, Community Benefits, and AdvocacyAudience Program Month PartnersGeneral Community Complementary techniques and options 1/22/10General Community Sharing with other survivors 1/26/10General Community Developing knowledge about cancer 1/27/10Prostate Support Group• Changes in prostate cancer treatment• Do treatments prevent the spread ofprostate cancer?• Advocating prostate health• Being healthy after cancer• Men’s issues related to sexuality• Taking care of your bones• What is the vaccine-like prostate cancertreatment?1/28/102/25/103/18/104/22/105/20/106/24/1010/21/1011/18/10General CommunityYoung Survivors group• Family activities• Sharing with other survivors• Issues younger survivors face• Being an active voice in the community• Survivorship1/29/102/19/103/20/104/23/105/30/106/9/10 Carol Diffendaffer, MSW, OSW‐CCancer Treatment <strong>Center</strong>General Community Tired of being tired? Cancer fatigue can be beat! 2/10/10General Community Cancer’s silver lining: finding positives 2/16/10General CommunityTime to HealBreast cancer survivors seminar, 12-week course2/22/10through5/10/10General Community Other cancer survivors understand 3/16/10General Community Facing Change: Grief and Loss, Part I 3/23/10General Community Cancer Survivors’ Day 4/11/10 <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> and TheCancer Treatment <strong>Center</strong>General Community Simplifying life 4/16/10 Carol Diffendaffer, MSW, OSW‐CCancer Treatment <strong>Center</strong>General CommunityMemorial Health <strong>Center</strong> Community Health Fair,Sidney, Neb.4/17/10 Jayme Hawk, RT (R)(T);—Gloria WilsonDorwart Cancer Care <strong>Center</strong>5
Audience Program Month PartnersGeneral CommunityGeneral CommunityGeneral CommunityGeneral CommunityGeneral CommunityMoving forward from change, grief, and loss,Part IIColon Cancer Community Health Fair,KNEB radio• Nine top cancer fighting foods• Diagnosis cancer—where do we go from here?Festival of HopeA nonprofit organization whose mission is to helpcancer patients who live in western Nebraska andeastern Wyoming with non-medical expenses asthey relate to their cancer care and treatment.• Healing power of spirituality• Cancer is a family disease• Why cancer prevents sleep• Moving beyond fears• Definitions of cancer words4/20/10 Carol Diffendaffer, MSW, OSW‐C, CancerTreatment <strong>Center</strong>5/19/10 Martha Stricker, BSN, CommunityHealth Nurse, <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong><strong>Center</strong>5/25/10 Carol Diffendaffer, MSW, OSW‐CCancer Treatment <strong>Center</strong>6/19/10 Carol Diffendaffer, MSW, OSW‐C,Jeff Kriewald, Director of CancerServicesCancer Treatment <strong>Center</strong>6/15/106/24/106/29/1010/19/1011/16/10Carol Diffendaffer, MSW, OSW‐CCancer Treatment <strong>Center</strong>General CommunityThelma Jones Memorial Golf TournamentThelma was an avid golfer and cancer patient whoinspired many with her positive mind. A annualmemorial golf scramble fund raiser is held in hername to benefit Cancer Services and Hospice.7/12/10 Carol Diffendaffer, MSW,, OSW‐CJeff Kriewald, Director of CancerServicesGeneral Community <strong>Annual</strong> cancer survivors’ picnic 7/20/10 Carol Diffendaffer, MSW, OSW‐CCancer Treatment <strong>Center</strong>General Community Night of HopeA nonprofit organization whose mission is to helpcancer patients who live in western Nebraska andnorthern Colorado with non-medical expenses asthey relate to their cancer care and treatment.8/13/10 Dorwart Cancer Care <strong>Center</strong> StaffGeneral CommunityCamp HopeProvides a unique experience for those affected bycancer, including survivors, their support persons,and medical professionals, in an atmosphere ofsharing, learning, fun, and relaxation.8/27/10-8/29/10<strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> and TheCancer Treatment <strong>Center</strong>General CommunityFarm and Ranch Museum HarvestFestival, Gering, Neb.Cancer prevention booth providing informationon services available from the American CancerSociety and gathering ideas to meet the needs ofthe community.9/18/10-9/19/10Kay Connery, American Cancer SocietyRepresentative6
Cancer Support GroupsDealing with disease in a positive way“I’m a firm believer in support groups,” says Cancer Treatment<strong>Center</strong> social worker and support group facilitator Carol Diffendaffer.“After attending a few meetings people usually feel likethey’re not alone anymore—it’s a great comfort knowing otherswith similar experiences.” She adds that those attending cancersupport groups learn to be advocates for themselves while developingcoping skills.The list of topics covered at meetings is diverse. In addition tosharing concerns and disease processes, topics include:• Healthy foods and exercise• Discussions about body image• Sexual changes and concerns• Perspectives of young survivors and those of varying ages;learning to move forward after a cancer diagnosis• Coping skills• Living with fatigue and side effects from treatment• Clinical trials• Advocating for yourself• Relationships• Regaining health“No subject is taboo,” says Diffendaffer. “Anyone can utilize thebenefits of a support group—as a matter of fact they’re every bitas important for the support person as for the cancer survivor.I definitely encourage support persons to attend the groups aswell.”Diffendaffer points to a study conducted at Ohio State Universitythat supports the benefits of support groups. Ohio State Universitypsychologist Barbara Anderson asked 58 women who had justundergone breast cancer surgery and were facing chemotherapyto gather weekly with a psychologist. No topic was discouraged—the women shared their fears and concerns, ways to improve eatingand exercise habits and feelings about sex and body image.They also learned techniques for relaxing their muscles in orderto better deal with stress.The results paid off. Blood tests taken four, eight, and 12 monthsinto the study showed the women who got support had far lowerlevels of the stress hormone cortisol—which dampens immuneresponse—than women in the control group (who did not attendsupport groups). The blood samples also revealed that supportgroup members had 25 percent higher amounts of a breast cancerantibody.Diffendaffer encourages anyone interested in a support groupto get on the mailing list for upcoming meetings. Call the CancerTreatment <strong>Center</strong> at 308.630.1348.• Complimentary treatments and techniques• Spirituality7
TOP RIGHT: Participants in the Cooking and Nutrition Women’s Forumtake a break from cooking an easy, nutritious meal. The class was sponsoredby <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong>’s Cancer Treatment <strong>Center</strong>.TOP LEFT: Carole Derr shows her lighter side at the 2011 Cancer Survivors’Day Celebration. The day’s theme was “Laughter is the BestMedicine.”BOTTOM: <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong>88
Peter Schilke, MD, Coordinator for the <strong>2010</strong> Cancer Conferences.Randall Williams, MD, also served as Coordinator.Conference<strong>2010</strong> Cancer<strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> held 23 bi-monthly multidisciplinaryCancer Conferences in <strong>2010</strong> to review and discuss current trendsin the treatment of cancer. Coordinators for <strong>2010</strong> were pathologistsPeter Schilke, MD and Randall Williams, MD.Physician representatives from all the appropriate disciplines, aswell as other cancer health care providers, attend and participate inthese conferences. Average attendance for physicians who activelyparticipated in cancer care was 12. The multidisciplinary averageattendance was 51.Fifty-five cases were presented. Sites discussed included: breast,lung, multiple myeloma, colon, appendix, kidney, Ewing’s sarcoma,cervical, ovarian, lymphoma, tongue, esophagus, testicular, endometrial,and prostate.mammography, the proposed United States Preventive ServicesTask Force guidelines, and when breast (MRI) magnetic resonanceimaging is appropriate.In August, Gottfried Ewald Konecny, MD, Assistant Professor ofMedicine, Division of Hematology-Oncology at the University ofCalifornia, Los Angeles, presented “Early Stage Breast Cancer.” Dr.Konecny discussed the current guidelines for treatment of earlystage breast cancer and the Tax 316 trial, prophylactic use of G-CSF, and the important safety information of Taxotere.To arrange for case presentation at Cancer Conference or forfurther information regarding the Cancer Registry, please call308.630.1747.In April, Lora D. Barke, DO, <strong>Medical</strong> Director, Invision Sally JobeBreast Network, presented “Current Status of Breast Imaging:What you need to know?” Dr. Barke discussed the similarities anddifferences between screen film mammography and full-field digital9
CancerRe g i s t r yBy Cindy Keller, CTR Cancer Registry CoordinatorThe Cancer Registry is a data collecting system for <strong>Regional</strong><strong>West</strong> <strong>Medical</strong> <strong>Center</strong>. The registry is one of the integral componentsrequired by the American College of Surgeons (ACOS)for accreditation as a Community Hospital Cancer Program,and has been accredited since 1985. The Cancer Registry isresponsible for the data collection and follow-up of all cancerpatients diagnosed and/or treated at <strong>Regional</strong> <strong>West</strong>. Thesecases are part of the computerized database utilizing RockyMountain Cancer Data Systems in Salt Lake City, Utah. Theupdated registry computer system allows instant retrieval capabilities.The database includes information on demographics,anatomic site, extent of disease at the time of diagnosis,history, staging of the cancer, and treatment summary.There were a total of 394 analytic cases added to the registryin <strong>2010</strong>. The Dorwart Cancer Care <strong>Center</strong> in Sidney, Neb.treated 21 new cases in <strong>2010</strong>. There have been 12,641 totalcases accessioned since January 1, 1982. The status of cancerpatients is followed annually to assure continued medicalsurveillance and to provide meaningful end-results data. As aresult of computerized follow-up letters and the cooperation ofstaff and referring physicians, the Registry maintains a followuprate of 98 percent.In April the Cancer Registrar attended the 36th annual NationalCancer Registrars Association Education Conference inPalm Springs, Calif. Many educational opportunities took placeduring the three day conference, including a review of the newstaging systems introduced in the 7th Edition, AJCC CancerStaging manual, and understanding and interpreting the <strong>2010</strong>Collaborative Stage Data Collection System (CSv2). In October,the Data Specialist and Cancer Registrar attended the 33rd<strong>Annual</strong> Tumor Registrars Association of Nebraska TRAN workshopheld in conjunction with the Nebraska CARES CancerSummit in North Platte, Neb. This was hosted by Great Plains<strong>Regional</strong> <strong>Medical</strong> <strong>Center</strong>. The state physician liaison, StevenDreyer, MD, presented “Revisions to Cancer Program Standardsfor 2012.” Many other sessions were held that informedand educated all who attended.10
Cancer Committee MembershipJune 1, 2009 – May 31, <strong>2010</strong>William Packard, MD Chairman, Cancer Committee (retired 12/31/09) | <strong>Medical</strong> OncologistCarol Willis, MD Chairman, Cancer Committee (effective 1/1/10) | PathologistTodd Sorensen, MD President/CEO | <strong>Regional</strong> <strong>West</strong> Health ServicesVincent Bjorling, MD <strong>Medical</strong> OncologistErnest Bussinger, MD Obstetrician/GynecologistGitesh Chheda, MD RadiologistGlen A. Forney, MD Chief of Staff/General SurgeonMark Hartman, MD Radiation OncologistJohn Kabalin, MD UrologistPeter Schilke, MD PathologistRichard Simmons, MD PathologistMelissa Stade, MD General SurgeonJason Walsh, MD General SurgeonRandall Williams, MD PathologistVance Siedenburg, PA-C Physician Assistant/Radiation OncologyCarol Diffendaffer, MSW, OSW‐C Social WorkerJan Taylor, MT (ASCP) Vice President, Ancillary ServicesShirley Knodel, RN, MS Chief Nursing Officer/Vice President, Patient ServicesKim Croft, RN, BSN Cancer Case ManagerChristine Buhr, RN, BSN Unit Manager, 3rd FloorNancy Sloan, PharmD Clinical PharmacistCindy Keller, CTR Coordinator, Cancer RegistryJeff Kriewald, BS RT (R)(T) Director, Cancer ServicesKent Dunovan, PT Director, RehabilitationLinda Rock, BA Director, Prairie Haven HospiceRob Flynn, BSN, RN Director, <strong>Medical</strong> Oncology Unit/2W2E/PedsJudith Heigel, CPMSM, CPCS Coordinator, <strong>Medical</strong> Staff*Clinton Dorwart, MD Family Practitioner | Memorial Health <strong>Center</strong>, Sidney*Kay Connery Representative, American Commission on Cancer11*Honorary Member
“We must be the change we wish to see in the world.”“A journey of a thousand miles begins with one small step.”Old Chinese Proverb12
Physician Liaison <strong>Report</strong>By Jason Walsh, MDGeneral Surgery | RWPC‐Surgery, Vascular DiagnosticsJason D. Walsh, MD, General Surgeon, began his term asCancer Liaison Physician July 8, <strong>2010</strong>. In this capacity, Dr.Walsh promotes communication and collaboration betweenthe American College of Surgeons, the Heartland Divisionof the American Cancer Society, <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong><strong>Center</strong> Cancer Committee, and local community agencies.Dr. Walsh attended Chadron State College and earned hismedical degree from the University Of Nebraska College OfMedicine. He completed his residency in General Surgery atGunderson Lutheran <strong>Medical</strong> Foundation in LaCrosse, Wis.Dr. Walsh has served as a Major in the United States ArmyReserve since 2002 and spent three months in Afghanistan.He is a member of the American <strong>Medical</strong> Associationas well as a Fellow in the American College of Surgeons.Along with Dr. Walsh’s new role as Physician Liaison, heserves on <strong>Regional</strong> <strong>West</strong>’s Surgery Committee and thePharmacy and Therapeutic/Infection Control Committee.In October, Dr. Walsh, along with Regine Leconte, MD, presenteda Clinical Trials Update for the general community.13
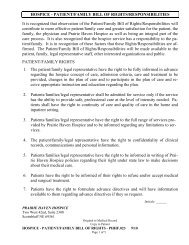
<strong>2010</strong> Comparison of Cancer DataThere were 436 cases of cancer and reportable tumors in the <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> Cancer Registry for <strong>2010</strong>. Ofthese, 42 cases were non-analytic, with a total of 394 cases qualifying for analysis (See Primary Site Table). Breast cancer isthe most frequently diagnosed and treated primary site at <strong>Regional</strong> <strong>West</strong>. All graphs shown include analytic cases only.COMPARISON CHARTSCASE COUNTS BY COUNTY OF RESIDENCESioux2Dawes13Box Butte41Sheridan7CherryScotts Bluff186Banner2Morrill21Garden5Grant1Arthur1Hooker ThomasMcPherson LoganKimball12Cheyenne33Deuel3Keith4LincolnTotal equals 394 casesfor <strong>2010</strong>PerkinsChase Hayes Frontier<strong>Regional</strong> <strong>West</strong>Out of state: 63DundyHitchcockRed WillowTOP FIVE INCIDENCE SITES-MENColon | 12Prostate | 59Kidney/Renal| 14Bladder | 19Lung| 24Other | 69NebraskaTOP FIVE INCIDENCE SITES-WOMENNationalColon | 16Breast | 82Corpus Uteri | 11Melanoma | 9Lung| 25Other | 54SOURCE: American College of Surgeons, National Cancer Data Base(NCDB), Benchmark report, 2005 National Data,2005 Nebraska Health & Human Service System - Nebraska CancerRegistry, <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong>.14
Primary SiteCancer Incidence by Primary Site • <strong>2010</strong> CasesCancer Treatment <strong>Center</strong> and Dorwart Cancer Care <strong>Center</strong>Non-AnalyticCasesAnalyticCasesSexBest AJCC StageM F Stage 0 Stage I StageIIBuccal Cavity/Pharynx 14 13 6 7 0 5 1 0 4 3Tongue/Other Tongue 8 7 3 4 0 4 0 0 2 1Major Salivary Gland 3 3 2 1 0 1 0 0 1 1Gum and Other Mouth 3 3 1 2 0 0 1 0 1 1Digestive System 58 56 29 27 0 10 17 9 13 7Esophagus 3 3 3 0 0 1 0 0 1 1Stomach 5 5 3 2 0 3 1 0 0 1Colon, Excluding Rectum 30 28 12 16 0 6 9 5 6 2Rectum and Rectosigmoid 9 9 6 3 0 0 3 2 3 1Liver 3 3 1 2 0 0 1 1 0 1Anus/ Anal Canal 1 1 0 1 0 0 1 0 0 0Pancreas 6 6 4 2 0 0 2 1 3 0Peritoneum 1 1 0 1 0 0 0 0 0 1Respiratory System 56 52 26 26 0 8 1 16 24 3Nasal Cavity, Sinuses, and Larynx 3 3 2 1 0 2 0 0 1 0Lung, Bronchus 53 49 24 25 0 6 1 16 23 3Soft Tissue 4 4 3 1 0 0 0 0 3 1Skin (Exc. Basal and Sq. Ca) 34 18 9 9 7 5 3 1 0 2Melanoma of the Skin 32 17 8 9 7 5 2 1 0 2Other Skin Cancer 2 1 1 0 0 0 1 0 0 0Breast 84 83 1 82 10 44 17 10 2 0Female Genital 17 15 0 15 1 7 1 3 2 1Cervix Uteri 2 2 0 2 0 1 0 0 1 0Corpus Uteri 13 11 0 11 1 6 0 2 1 1Ovary 2 2 0 2 0 0 1 1 0 0Male Genital 91 59 59 0 0 0 49 5 5 0Prostate 90 58 58 0 0 0 49 4 5 0Testis 1 1 1 0 0 0 0 1 0 0Urinary System 42 42 34 8 20 12 5 2 2 1Urinary Bladder 23 23 19 4 18 2 2 0 1 0Kidney and Renal 18 18 14 4 1 10 3 2 1 1Ureter 1 1 1 0 1 0 0 0 0 0Brain and Other Nervous System 17 17 10 7 N/A N/A N/A N/A N/A N/ABrain 7 7 4 3 N/A N/A N/A N/A N/A N/AOther Nervous System 10 10 6 4 N/A N/A N/A N/A N/A N/AEndocrine System 10 9 4 5 0 3 0 1 0 5Thyroid 4 4 1 3 0 3 0 1 0 0Other Endocrine – Pituitary 6 5 3 2 N/A N/A N/A N/A N/A N/ALymphatic System 16 15 10 5 0 3 4 4 3 1Non-Hodgkin’s Disease 16 15 10 5 0 3 4 4 3 1Multiple Myeloma 5 4 2 2 NA NA NA NA NA NABlood/Leukemia 8 6 4 2 NA NA NA NA NA NAChronic Lymphocytic 2 2 2 0 NA NA NA NA NA NAAcute Myeloid 5 3 2 1 NA NA NA NA NA NAOther Leukemia 1 1 0 1 NA NA NA NA NA NAOther, Ill-Defined and Unk. 1 1 0 1 NA NA NA NA NA NAAll Sites Combined 457 394 197 197 38 97 98 51 58 24StageIIIStageIVNotStaged15M-male, F-female, AJCC Stage Grouping T, N, and M categories describe the anatomic extent of disease.Stage groupings gather cases into homogeneous categories to facilitate analysis. See glossary.
Reconstructive Surgeryafter Breast CancerBy Mary C. Snyder, MDPlastic and Reconstructive Surgery | Monument Plastic SurgeryBreast cancer continues to be the most commonly diagnosed malignancy in women in the U.S., after non-melanoma skincancer. Over the last 10 years, rates of breast cancer have decreased in women over the age of 50, yet the lifetime risk ofdeveloping a cancer of the breast remains one in eight. Over 200,000 cases of invasive disease are diagnosed each year andearly stage disease, or DCIS, is found in over 50,000 patients (1). Death rates from breast cancer have declined over the last20 years, and the current prognosis is favorable, with five year survival rates of approximately 80 percent both at <strong>Regional</strong><strong>West</strong> <strong>Medical</strong> <strong>Center</strong> and nationwide (2). There are approximately 2.5 million breast cancer survivors in the United States,with that number expected to rise over the next 10 years (3).Although many women elect for breast conserving treatment(such as lumpectomy) when faced with the diagnosisof breast cancer, approximately 30 percent of breast cancerpatients choose to undergo mastectomy (4). Recent datasuggests more women are undergoing prophylactic mastectomyon the uninvolved breast in cases of unilateral disease.Additionally, with the advent of genetic testing for BRCA, bilateralprophylactic mastectomies are being performed morefrequently (5). An increase in the number of mastectomiesperformed has led to an increased number of breast reconstructiveprocedures (6).Although not every patient is a candidate for breast reconstruction,it is an option for many women, either at the timeof mastectomy or after completion of treatment. The numberof women who undergo breast reconstruction followingmastectomy in the United States is just under 20 percent.Some studies have shown that women who undergo breastreconstruction after mastectomy report improved quality oflife, including psychosocial and sexual well being, as comparedto those who undergo mastectomy alone (7,8). Significant discrepanciesexist in rates of breast reconstruction among minoritiesand those in certain geographic areas. The Women’sHealth and Cancer Rights Act, which mandates insurancecoverage of breast reconstruction following mastectomy, wasenacted in 1999 (9). However, rates of reconstruction have notsignificantly increased after this law took effect, indicating factorsother than insurance coverage are involved, including lackof availability of a reconstructive surgeon or failure to refer tosuch specialists (10).Breast reconstruction generally falls into one of two categories,autologous tissue or implant. Reconstruction with autologoustissue usually involves skin, fat, and muscle moved from theabdomen, back, buttocks, or thighs. The most common type ofautologous tissue used is the TRAM flap, which involves movingabdominal tissue to the chest to recreate the breast. This tissuerequires a blood supply, provided either by an abdominal musclewhich remains attached, or by a microvascular procedure tosupply blood from vessels in the chest. The TRAM flap is usedmost often in unilateral breast reconstruction and is associatedwith the highest satisfaction rates among patients regardingtheir reconstruction, likely a result of the ability of the tissue tomatch the natural shape and feel of the opposite breast (11).Implant-type reconstruction is a multi-stage procedure that involvesplacement of a temporary implant, or tissue expander, atthe first stage. The tissue expander allows the skin and muscleof the chest wall to be gradually stretched to a size and shapethat is acceptable to both the patient and the surgeon. Once theappropriate expansion is reached, the tissue expander is removedand either a silicone or saline implant is placed. This type of reconstructionhas a quicker recovery time than most autologoustissue reconstructions as it does not involve an additional surgicalsite on the body, such as the abdomen. Many women who elect tohave prophylactic mastectomies chose to have expander-implantreconstruction as it is easier to match the two breasts with implants,resulting in high patient satisfaction rates (11).Continued...16
“We must be the change we wish to see in the world.”ContinuedBreast Cancer ReonstructionNipple and areola reconstruction is usually performed at a laterstage, following completion of the breast mound. Many techniquesare described to reconstruct the nipple and areola, butmost involve the use of skin on the new breast, which is raisedand sutured to create a nipple. Color is then applied to the nippleand areola area by tattooing.The decision to undergo breast reconstruction can be a difficultchoice for a woman who is facing the diagnosis of breast cancer.Whether she elects to undergo reconstruction at the time of mastectomy,after completion of treatment, or not at all, is influencedby many factors, including lifestyle, family, co-morbidities, andstage of disease. This decision cannot be made without adequateinformation. As part of her treatment process, each breast cancerpatient should be given the opportunity to investigate whetherbreast reconstruction is appropriate for her.References1. American Cancer Society, Cancer Statistics, <strong>2010</strong>. Available at http://caonline.amcancersoc.org/cgi/content/full/caac.20073v1,accessed June 26, 2011.172. National Cancer Data, State of Nebraska, <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> data.3. De Angelis R, Tavilla A, Verdecchia A, et al. Breast cancer survivors in the United States:Geographic variability and time trends. 2005-2015. Cancer 2009; 115:1954-1966.4. Baxter NN, Virnig BA, Durham SB, et al. Trends in treatment of ductal carcinoma in situof the breast. L Natl Cancer Inst 2004;96:443-4485. Tuttle TM, Jarosek S, Habermann EB, et al. Increasing rates of contralateral prophylacticmastectomy among patients with ductal carcinoma in situ. J Clin Oncol,2009;27:1362-1367.6. Gos LL, Smith BL, Liao EC. Evolution of breast reconstruction paradigms driven byincrease in numbers of bilateral mastectomy. Plast Reconstr Surg 2011;127:30.7. Wilkins EG, Cederna PD, Lowery JC, et al. Prospective analysis of psychosocial outcomesin breast reconstruction: one-year postoperative results from the MichiganBreast Reconstruction Outcome Study. Plast Reconstr Surg 2000;106:1014-1025.8. Kpodzo DS, Antony A, Damjanovic B, Chretien Y, Austen WG, Colwell AS. Post-mastectomybreast reconstruction versus mastectomy alone: A comparative assessment ofquality of life using patient-reported satisfaction, body image and sexual well-being.Plast Reconstr Surg 2011;127:46.9. The Women’s Health and Cancer Rights Act. Available at https://www.cms.gov/HealthInsReformforConsume/06_TheWomen%27sHealthandCancerRightsAct.asp,accessed June 26, 2011.10.Alderman AK. Use of Breast Reconstruction after Mastectomy Following the Women’sHealth and Cancer Rights Act. JAMA 2006;295(4):387-388.11. Craft RO, Colakoglu S, Curtis MS, et al. Patient satisfaction in unilateral and bilateralbreast reconstruction. Plast Recon Surg 2011;127(4):1417-1424.
Breast Cancer Diagnosed2000–2008National Cancer Data Base: All States – 1,631,390 casesNebraska - 10,097 cases, and <strong>Regional</strong> <strong>West</strong> <strong>Medical</strong> <strong>Center</strong> - 643 casesAJCC Stage<strong>Regional</strong> <strong>West</strong> nebraska all statesSTAGE I STAGE II STAGE III STAGE IV UNKNOWNAge at diagnosis<strong>Regional</strong> <strong>West</strong> nebraska all states20-29 30-39 40-49 50-59 60-69 70-79 80-89 90+21
On‐Site <strong>Medical</strong> PhysicistEnhances <strong>Regional</strong> <strong>West</strong>’sNationally RecognizedBy Joanne Krieg<strong>Regional</strong> <strong>West</strong> Marketing and Public Relations DepartmentCancer ProgramIn 2008, The Cancer Treatment <strong>Center</strong> at <strong>Regional</strong> <strong>West</strong> was the only cancer program in Nebraska and one of 66 nationwide to receivean Outstanding Achievement Award from the American College of Surgeons Commission on Cancer. The award recognizes cancerprograms that strive for excellence in providing quality care to cancer patients.<strong>Regional</strong> <strong>West</strong>’s combination of personalized care and technologicallyadvanced cancer treatment services may be unique for a ruralcancer program, but its award-winning distinction over every othercancer program in the state points to exceptional service and attentionto detail that is truly outstanding.Director of Cancer Services Jeff Kriewald, BS, RT (R)(T) says that chiefamong benefits to patients offered by the Cancer Treatment <strong>Center</strong>and the Dorwart Cancer Care <strong>Center</strong> is the fact that they have thededicated services of a full-time board-certified medical physicist.“Many smaller and especially rural treatment centers around thenation rely on large physics groups to provide coverage for theircenters, but we benefit from having Ross Johnson on-site everyday,”said Kriewald. “As a board-certified medical physicist in bothdiagnostic radiological physics and therapeutic radiological physics,Ross serves as the Radiation Safety Officer for <strong>Regional</strong> <strong>West</strong> andoversees all treatment plan designs for patients treated at both cancercenters.”On any given day Johnson may use a Geiger counter to verify radiationcontainment following High-Dose Rate (HDR) treatment, reviewradiation therapy patient charts, or calibrate a linear accelerator. Heis involved with patient treatment issues daily – verifying targets andradiation dosage to ensure safe and effective radiation treatment.“I understand the nature of the low-level effects of radiation. There area lot of risks. I analyze the probability of those risks,” he said.With his understanding of radiation safety, Johnson is charged withmonitoring the Cancer Treatment <strong>Center</strong>’s equipment performance andmechanical integrity, equipment installations, and control of radiationhazards. He performs yearly radiation safety instruction for hospital departmentsand helps ensure compliance with the State of Nebraska asit relates to <strong>Regional</strong> <strong>West</strong>’s radioactive materials license.Johnson earned his undergraduate degree in physics and a master’sdegree in radiological science at the University of California-Irvine.He has worked for health care facilities in Illinois, Kansas, Iowa,North Dakota, and Texas. He came to western Nebraska about 10years ago to provide a week’s coverage at the Cancer Treatment<strong>Center</strong>, but he liked the area and was asked to stay.“We have a good community‐based cancer treatment programhere,” said Johnson.He is pleased with the evolution from the opening of the Cancer Treatment<strong>Center</strong> to the development of a formal radiation therapy program,which now includes IMRT—Intensity Modulated Radiation Therapy.IMRT is an advanced form of radiation therapy that is particularly beneficialin the treatment of prostate, head, and neck cancer. It allowsvery precise control of higher and more effective doses of radiation totumors—resulting in better outcomes with fewer side effects.Johnson was instrumental in planning and launching IMRT at <strong>Regional</strong><strong>West</strong> – a project so complex that it took nearly two years fromapproval to implementation.“IMRT has better capabilities and finer resolution for dealing withsensitive structures.We can customize treatment to hit specific target shapes and confinetreatment around the tumor to avoid healthy tissue,” he said.For every patient who undergoes 15 to 30 minutes of treatment withIMRT, Johnson spends two days or more planning the treatment,verifying targets, collecting data, running quality control checks,checking calibration and more to ensure the safety and effectivenessof IMRT treatment.“Ross Johnson and our physics staff perform all their work behindthe scenes, but the efforts provided by this group help make our programthe outstanding cancer center that it is today,” said Kriewald.23
<strong>Medical</strong> Physicist Ross Johnson, MS, DABR,oversees radiation usage and safety at TheCancer Treatment <strong>Center</strong> in Scottsbluff andthe Dorwart Cancer Care <strong>Center</strong> in Sidney.24
Glossary of TermsAJCC STAGEAmerican Joint Committee on Cancer Staging Schemeusing tumor size, node involvement and metastases todistant sites, T=primary tumor size; N=regional lymph nodeinvolvement; M=metastasis or distant spreadAJCC STAGE GROUPINGSStage 0 Carcinoma in-situStage I Localized carcinomaStage II: Limited local extension and/or limited regionallymph node involvementStage III: More extensive local extension or regional lymphnode involvementStage IV Involvement of distant sitesANALYTICCancer cases initially diagnosed and /or having receivedall or part of the first course of treatment at <strong>Regional</strong> <strong>West</strong><strong>Medical</strong> <strong>Center</strong>FIRST COURSE OF TREATMENTPlanned definitive therapy initiated within four monthsfollowing initial diagnosisNCDBNational Cancer Date BaseOBSERVED SURVIVAL RATEThe literal survival rate from counting each case in the RegistrySTAGE GROUPING PURPOSET, N, and M categories describe the anatomic extent of thedisease. Stage grouping gathers cases into homogenouscategories to facilitate analysisUNKNOWNTumor is said to be unknown when the stage cannot bedetermined from the medical record or a medical authority25