View an interactive PDF of this edition - Medical Protection Society
View an interactive PDF of this edition - Medical Protection Society
View an interactive PDF of this edition - Medical Protection Society
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
MEDICAL PROTECTION SOCIETYPROFESSIONAL SUPPORT AND EXPERT ADVICEFoundation doctors:Receive a free Oxford H<strong>an</strong>dbookRenew your membership with MPS <strong>an</strong>dyou c<strong>an</strong> choose a free Oxford H<strong>an</strong>dbookwww.mps.org.uk/foundationyears15 AVAILABLE TITLESAnaesthesiaF1 Doctors50% subscription rate discount – renew your MPSmembership before 31 May 2013 <strong>an</strong>d you will receive a50% discount on your subscription – so you pay just £20instead <strong>of</strong> £40 for your F2 yearPlus receive a free Oxford H<strong>an</strong>dbook <strong>of</strong> your choicefrom the 15 available titles.Renew online today – www.mps.org.uk/F2F2 DoctorsReceive a free Oxford H<strong>an</strong>dbook <strong>of</strong> your choice from the15 available titles, when you renew your membership foryour fi rst year <strong>of</strong> specialty training.Renew online today – www.mps.org.uk/STRenew your membership todayT 0845 718 7187E juniordoctor@mps.org.ukW www.mps.org.uk/foundationyearsCardiologyClinical <strong>an</strong>d LaboratoryInvestigationsClinical DiagnosisClinical SurgeryEmergency MedicineExp<strong>edition</strong> MedicineGastroenterology<strong>an</strong>d HepatologyGeneral PracticeGeriatric MedicineObstetrics <strong>an</strong>d GynaecologyPaediatricsPsychiatryRespiratory MedicineTrauma <strong>an</strong>d OrthopaedicsMPS1194: 01/13
3Inside <strong>this</strong> issue <strong>of</strong> New Doctor…Page 4 UpdateA revalidation update for all foundation doctorsabout what to do nextPage 4 EventsA snap shot <strong>of</strong> all the top events for foundationdoctors over the next few monthsPage 5 Hot topic: Consent foraudio/visual recordingsMPS Medicolegal Adviser Dr Pallavi Bradshawexplores what consent you need totake photographs <strong>an</strong>d make recordingsPage 5 Top five medical appsDr Josephine Neale has done the app workso you don’t have toPage 6–7 Dilemma: DNAR ordersDr Jonny Morris describes a tricky case <strong>of</strong>a patient with a do not attempt resuscitation(DNAR) orderPage 8–9 Ask MPSHere Dr Sarah Clarke shares the hurdles shefaced when tackling the mental capacity issuesin relation to her patient Mr KPage 10-12 Essential learning:Law <strong>an</strong>d ethicsEarn CPD points by reading Dr Paul Nisselle’sfeature on the key legal <strong>an</strong>d ethical topics in thefoundation curriculumPage 13 From ward to world:Saving lives in EthiopiaDr Tom Bashford won a Patient Safety Award forhis work promoting safer surgery in Ethiopia.He shares his storyPage 14–15 A week in the life <strong>of</strong> <strong>an</strong>F2 working in a refugee campWorking in a Burmese refugee camp c<strong>an</strong> reallyopen your eyes to what matters in medicine, saysDr June Tay. She shares her personal experiencesEDITOR-IN-CHIEF Dr Gordon McDavid EDITOR Sara Williams CONTRIBUTORS Dr Jo Pointon, DrJune Tay, Dr Tom Bashford, Dr Paul Nisselle, Dr Sarah Clarke, Dr Jonny Morris, Dr Josephine Neale DESIGNJayne Perfect, Anna W<strong>an</strong>czyk PRODUCTION MANAGER Philip Walker MARKETING Peter Macdonald,Kim Beaumont EDITORIAL BOARD Dr Steph<strong>an</strong>ie Bown, Gareth Gillespie, Dr Paul Mackin, Dr Chris Godeseth,Dr Jayne Molodynski, Shelley McNicol, Dr Jo Galvin, Dr Pallavi Bradshaw New Doctor <strong>Medical</strong> <strong>Protection</strong><strong>Society</strong>, Victoria House, 2 Victoria Place, Leeds LS11 5AE Tel: 0113 241 0530 Fax: 0113 241 0500GET THE MOST FROMYOUR MEMBERSHIPVisit our website for publications,news, events <strong>an</strong>d other information:www.mps.org.ukFollow us on Twitter at:www.twitter.com/MPSdoctorsOpinions expressed herein are those <strong>of</strong> the authors. Pictures shouldnot be relied upon as accurate representations <strong>of</strong> clinical situations.© The <strong>Medical</strong> <strong>Protection</strong> <strong>Society</strong> Limited 2013. All rights are reserved.GLOBE (logo) (series <strong>of</strong> 6)® is a registered UK trade mark in thename <strong>of</strong> The <strong>Medical</strong> <strong>Protection</strong> <strong>Society</strong> Limited.Cover: © IMAGES/VSO/PHOTGRAPHER BEN LANGDONWe welcome contributions toNew Doctor. Please contact us on0113 241 0377 oremail sara.williams@mps.org.ukWelcomeDr Gordon McDavid – Editor-in-chiefMPS Medicolegal AdviserWelcome to your new <strong>edition</strong> <strong>of</strong>New Doctor <strong>an</strong>d the first <strong>of</strong> 2013.The cover story <strong>of</strong> <strong>this</strong> issue chartsthe story <strong>of</strong> Tom who left the confines<strong>of</strong> a large London teaching hospitalto travel to Ethiopia for a year to driveup patient safety st<strong>an</strong>dards in AddisAbaba. Read about how he won apatient safety prize for his efforts onpage 13.Every doctor will face difficultsituations from time to time whereit is necessary for the treating teamto draw on their collective experienceto achieve a desirable outcome.Have a look at the dilemmas featuredon pages 6 <strong>an</strong>d 8.On page 8 Dr Sarah Clarke givesa c<strong>an</strong>did tale <strong>of</strong> her difficulties inm<strong>an</strong>aging a patient at the interfacebetween two specialties.While on page 6, the controversialissue <strong>of</strong> end-<strong>of</strong>-life decisions istackled head on by Dr Jonny Morris.Another thought-provoking articleis Dr Paul Nisselle’s piece on the keyethical principles governing medicalpractice. This piece describesthe interlocking relationship betweenethics <strong>an</strong>d the law, knowledgeessential for <strong>an</strong>y practising doctor.This topic is so import<strong>an</strong>t we’vesupplemented the article with twoonline modules, why not havea look <strong>an</strong>d download a certificate<strong>of</strong> completion for inclusion in yourePortfolio. I hope you enjoy the issue.CONTENTS NEW DOCTOR | VOLUME 6 | ISSUE 1 | 2013 | UNITED KINGDOM www.mps.org.uk
4UpdateA snap shot <strong>of</strong> news for foundation doctorsUPDATE NEW DOCTOR | VOLUME 6 | ISSUE 1 | 2013 | UNITED KINGDOM www.mps.org.uk©IAN HOOTON/SCIENCE PHOTO LIBRARYRevalidation round-upThe GMC has begun revalidating alldoctors – here’s what you need to knowEvery doctor who is registered witha licence to practise needs to revalidatewith the GMC; <strong>this</strong> includes doctors infoundation year two <strong>an</strong>d specialty training.To revalidate new doctors will require theirresponsible <strong>of</strong>ficer to make a recommendationto the GMC that they are up-to-date, fit topractise <strong>an</strong>d should be revalidated.You will already be in regular discussionabout your progress with your supervisors.These discussions should include reflectingon strengths <strong>an</strong>d weaknesses <strong>an</strong>d signific<strong>an</strong>tachievements or difficulties, which will usuallyencompass information on signific<strong>an</strong>t events,<strong>an</strong>d complaints.The org<strong>an</strong>isation that will be supportingyour revalidation is called your ‘designatedbody’; these vary depending on where youare a trainee (see text box).Doctors will need to collect supportinginformation to show how they are meeting theGMC’s pr<strong>of</strong>essional st<strong>an</strong>dards in day-to-dayEvent When Where What Further informationMPS Communication SkillsWorkshopsNational Conference forAspiring SurgeonsASiT Foundation Skills inSurgery CourseFoundation ProgrammeSharing EventThroughoutyearAcross UK2 March Birmingham5 April Cardiff12 June Londonpractice. This information will be generatedwhile training, but the GMC expectsyou to collect additional information where yourtraining programme does not expect youto collect evidence.When you revalidate will depend on howlong your training lasts:■■If your training lasts less th<strong>an</strong> five years,your first revalidation will be at the point<strong>of</strong> eligibility for CCT■■If your training lasts longer th<strong>an</strong> five years,you will be revalidated five years after yougained full registration, <strong>an</strong>d again at the point<strong>of</strong> eligibility for CCT.When your training is complete, yourdesignated body will ch<strong>an</strong>ge to theorg<strong>an</strong>isation where you practise. The GMCshould be informed when <strong>this</strong> ch<strong>an</strong>ge occurs– you c<strong>an</strong> do <strong>this</strong> using GMC Online.From <strong>this</strong> point you will need to have regularappraisals <strong>an</strong>d collect supporting evidenceto show you are meeting st<strong>an</strong>dards.The GMC has included useful information on their website,including <strong>an</strong> FAQ section, visit www.gmc-uk.org/doctors/revalidation.asp or email revalidation@gmc-uk.orgMix with other specialties <strong>an</strong>d reduce your risk at MPS’spopular workshop<strong>Medical</strong> students <strong>an</strong>d foundation doctors are invited tosubmit abstracts for oral <strong>an</strong>d poster presentations at <strong>this</strong>research conferenceThis popular one-day course will equip senior medicalstudents <strong>an</strong>d junior doctors with the fundamental techniquesrequired for surgical successThis event is a great opportunity for foundation doctors topresent <strong>an</strong>d shareRegional variationsEngl<strong>an</strong>dDesignated body:postgraduate de<strong>an</strong>eryResponsible <strong>of</strong>ficer:postgraduate de<strong>an</strong>NB. This will ch<strong>an</strong>ge whenpostgraduate de<strong>an</strong>eriesare replaced by localeducation <strong>an</strong>d trainingboards in April 2013.Scotl<strong>an</strong>dDesignated body: NHSEducation for Scotl<strong>an</strong>dResponsible <strong>of</strong>ficer:medical director for NHSEducation for Scotl<strong>an</strong>dWalesDesignated body:Wales De<strong>an</strong>eryResponsible <strong>of</strong>ficer:postgraduate de<strong>an</strong>Northern Irel<strong>an</strong>dDesignated body:Northern Irel<strong>an</strong>d <strong>Medical</strong><strong>an</strong>d Dental TrainingAgency (NIMDTA)Responsible <strong>of</strong>ficer:postgraduate de<strong>an</strong>www.mps.org.uk/workshopswww.rcsed.ac.uk/aspiringsurgeonsbristolwww.asit.org/events/conferences/2013/pre-courses/FSSwww.nact.org.uk
5Consent for audio/visual recordingsConsent for taking photographs <strong>an</strong>d making recordings isvital, explains MPS medicolegal adviser Dr Pallavi BradshawHOT TOPICThe smart phone revolution hasfundamentally ch<strong>an</strong>ged the waywe interact in society <strong>an</strong>d hascreated a reli<strong>an</strong>ce on technology thatpervades even clinical practice. Withthe invention <strong>of</strong> medical apps, goneare the days <strong>of</strong> white coats ladenwith various clinical h<strong>an</strong>dbooks. It isunsurprising that mobile phones are<strong>of</strong>ten used to take photographs <strong>of</strong>interesting cases <strong>an</strong>d recordings made<strong>of</strong> interesting patients. Whilst most <strong>of</strong>these photographs are taken to showto colleagues to aid diagnosis or tobe used as potential case reports,the doctors taking the photographsmay be inadvertently breaching GMC,employment <strong>an</strong>d legal obligations, ifthe right consent has not been taken.Documented consent is requiredfor all images taken (save for internalinvestigations <strong>an</strong>d pathology slides)<strong>an</strong>d trusts will usually have specificconsent forms that should be usedor medical photography departmentswho c<strong>an</strong> guide you through the process.The GMC has producedsupplementary guid<strong>an</strong>ce Making<strong>an</strong>d using visual <strong>an</strong>d audio recordings<strong>of</strong> patients (2011), it sets out thepr<strong>of</strong>essional obligations <strong>of</strong> takingimages or recordings <strong>of</strong> patients. Issuesaround confidentiality <strong>an</strong>d consent areparamount <strong>an</strong>d must not be overlookedeven in the theatre setting with<strong>an</strong>aesthetised patients.Any image whether it is <strong>an</strong>onymisedor otherwise, forms part <strong>of</strong> the medicalrecord, so <strong>this</strong> data must be stored<strong>an</strong>d processed as per the Data<strong>Protection</strong> Act (1998). It is thereforenot acceptable to be carrying images<strong>of</strong> patients on one’s mobile phoneor electronically sending them on.There is clearly a risk <strong>of</strong> the data beinglost or stolen <strong>an</strong>d the fact remainsthat most hospital doctors will notbe registered as a Data Controlleras would be required. Should theimages become lost you would havea duty to notify your employer <strong>an</strong>d thepatient, which would lead to difficultquestions being asked <strong>an</strong>d likelydisciplinary action. There may be timeswhen a photo would aid diagnosis inemergency situations if the clinici<strong>an</strong>is <strong>of</strong>f site, but generally these imagesshould be relayed via secure emails<strong>an</strong>d immediately deleted after storingin the records. You should discusssuch deletion with your employer’sIT department.If there is a clinical need or adesire to take images for diagnosisor education purposes it is notappropriate to use personal cameras<strong>an</strong>d mobile phones. Agreementby a patient to take <strong>an</strong> image doesnot obviate your obligations toyour employer, or your duties <strong>of</strong>confidentiality. There are ultimately nocircumst<strong>an</strong>ces, save for emergencies,when taking patient images on a mobilephone, whether consented or not,is justified, so should not be done.NB. Doctors working in a GP settingor in private practice should seekfurther advice if they are concerned.Top five medical apps for foundation doctorsDr Josephine Neale, <strong>an</strong> F2 from Warwickshire, has done the app workso you do not have to. Here are her top five apps for new doctorsDiAppBetesDevelopedfrom nationalguidelinesby a teamin UniversityHospital Southampton, <strong>this</strong> isa gem for those who have everfound themselves adjustinginsulin dosing regimes withoutmuch success.Although it is not a replacementfor senior advice, <strong>this</strong> appprovides support <strong>an</strong>dclear information for insulinprescribing, hypoglycaemia,specialist referral criteria <strong>an</strong>dwhen to stop or start diabeticmedication in <strong>an</strong> inpatientsetting.Cost – free.NICE BNFNo morerummagingaround the wardto find a BNF –now it c<strong>an</strong> be at your fingertipswithout the need for <strong>an</strong> internetconnection after the initialdownload. There is <strong>an</strong> easysearch function <strong>an</strong>d you c<strong>an</strong>bookmark your most frequentlyused pages. The BNF forchildren is also available <strong>an</strong>dworth downloading.Cost – requires <strong>an</strong> NHS Athensaccount to login.CliniCalcIf you havetroublerememberingyour A-agradient from your Anion gap,or your Child-Pugh from yourCHADS2, <strong>this</strong> is the app foryou. Categorised by specialty,<strong>this</strong> app has everythingfrom simple GCS remindersto predicted spirometricvalues, with some statisticalcalculations in there as well.Cost – free.PasTestYou probablywill have seenor used PasTestduring your timeat medical school. Now yourtime is precious <strong>an</strong>d on-the-gorevision is a necessity – <strong>this</strong> iseven available without internetconnection. Like the full site,the features include QuestionBrowser, Timed Tests <strong>an</strong>d MockExams. Cost – free demoversions, further question b<strong>an</strong>krequires a subscription fee.Patient.co.ukMuch <strong>of</strong> afoundationdoctor’s job iscommunicatinginformation topatients. After a high-speedpost-take ward round, <strong>this</strong>app c<strong>an</strong> help you tr<strong>an</strong>slateyour medical jargon into plainEnglish for your baffled patients.Conditions from Achalasiato Yellow Fever are summarisedconcisely <strong>an</strong>d m<strong>an</strong>y haveaccomp<strong>an</strong>ying diagrams.Cost – free to view conditionleaflets.NEW DOCTOR | VOLUME 6 | ISSUE 1 | 2013 | UNITED KINGDOM www.mps.org.uk
12MEDICOETHICAL NEW DOCTOR | VOLUME 6 | ISSUE 1 | 2013 | UNITED KINGDOM www.mps.org.ukInformativeDOCTORPaternalisticm<strong>an</strong>aged to fracture his pelvis. ECT wasnew at that time, <strong>an</strong>d medical opinionwas divided on whether a relax<strong>an</strong>t<strong>an</strong>aesthetic should be used. 5In the subsequent legal action,the court was invited to decide betweenthe two competing medical schools<strong>of</strong> thought – relax<strong>an</strong>t or no relax<strong>an</strong>t.The court said it was not competent todecide on a medical issue. The judgein that case said that: “A doctor is notguilty <strong>of</strong> negligence if he has acted inaccord<strong>an</strong>ce with a practice accepted asproper by a responsible body <strong>of</strong> medicalmen skilled in that particular art.”This has been tweaked a bit overthe years, but the ‘Bolam test’ or‘Bolam st<strong>an</strong>dard’, also called the ‘PeerPr<strong>of</strong>essional Accept<strong>an</strong>ce’ or ‘Reasonabledoctor’ test, remains the yardstick.Hippocrates wrote that doctorsshould: “Continue with diligence to keepabreast <strong>of</strong> adv<strong>an</strong>ces in medicine.”In 1711 Alex<strong>an</strong>der Pope cautioned usto: “Be not the first by whom the neware tried, nor yet the last to laythe old aside.” Neither ethics nor thelaw requires us to be the best doctor inthe world, but we do need to attain <strong>an</strong>dmaintain that level <strong>of</strong> skill in what we dothat would attract peer support.Shared decision making“Doctor’sorders”Passive PATIENT ActiveREFERENCES1. Schloendorff v <strong>Society</strong> <strong>of</strong> New York Hospital (1914)2. NHSLA, Risk M<strong>an</strong>agement H<strong>an</strong>dbook (2012)3. Gillick v West Norfolk <strong>an</strong>d Wisbech Area Health Authority (1985)4. Donoghue v Stevenson (1932)5. Bolam v Friern Hospital M<strong>an</strong>agement Committee (1957)SharedDecisionMaking“Patient’schoice”JusticeThere are three elements to Justice:■■■Distributive justice – fair distribution<strong>of</strong> limited healthcare resources■■ ■Rights-based justice – respect forpeople’s rights, such as prohibition<strong>of</strong> discrimination■■■Legal justice – respect for the law.On <strong>an</strong> individual patient level,there are some obvious elements to‘Justice’– for example, not discriminatingagainst patients on the basis <strong>of</strong> theircolour, race, religion, etc; but c<strong>an</strong> werefuse to perform cardiac surgery ona patient because they smoke? Is thatdiscrimination – punishing the patientfor not stopping – or a fair medicaljudgment based on their increased risk<strong>of</strong> complications at <strong>an</strong>d after surgery?More broadly, we do our best tomaintain a focus on the patient infront <strong>of</strong> us, but we are aware <strong>of</strong> theneed to bal<strong>an</strong>ce that patient’s rights<strong>an</strong>d needs against the need for <strong>an</strong>equitable allocation <strong>of</strong> healthcare funds<strong>an</strong>d resources. Who decides whatis ‘equitable’? The ethical principle <strong>of</strong>Justice imposes a moral obligation todecide fairly between competing claims.Dr Nisselle is a senior consult<strong>an</strong>tat MPS Educational Services.He c<strong>an</strong> be contacted atpaul.nisselle@mps.org.ukLOOKING FOR EVIDENCE FORYOUR ePORTFOLIO?MPS is committed to education <strong>an</strong>dtraining. As well as helping you providethe best care for your patients, we w<strong>an</strong>tto support your development. That iswhy we have developed two onlinelearning modules on the topics coveredin <strong>this</strong> article, so that you c<strong>an</strong> downloada certificate <strong>of</strong> completion as evidence<strong>of</strong> your learning for your ePortfolio.What to do next….■■Once you’ve read <strong>this</strong> article, simplygo to www.mps.org.uk/e-portfoliowhere you c<strong>an</strong> register for theE-learning platform■■You’ll need your membership detailsto register <strong>an</strong>d log on■■Once logged on, you will be able toaccess the modules highlighted onthe home page■■You c<strong>an</strong> complete the modules at atime that suits you■■Download your certificate <strong>of</strong>completion <strong>an</strong>d <strong>an</strong>y supporting notes■■Other modules on a wide r<strong>an</strong>ge<strong>of</strong> subjects c<strong>an</strong> also be accessedthrough the E-learning platformTo learn more visit MPS’s website■■Access the MPS library <strong>of</strong>factsheets, <strong>this</strong> includes detailedinformation on the law aroundconsent <strong>an</strong>d confidentiality –www.medicalprotection.org/uk/factsheets■■Visit the h<strong>an</strong>dbooks <strong>an</strong>d bookletssection, to read more aboutconsent <strong>an</strong>d the ethical mazethat is modern medicine – www.medicalprotection.org/uk/advice<strong>an</strong>d-publications/booklets-<strong>an</strong>dh<strong>an</strong>dbooks.
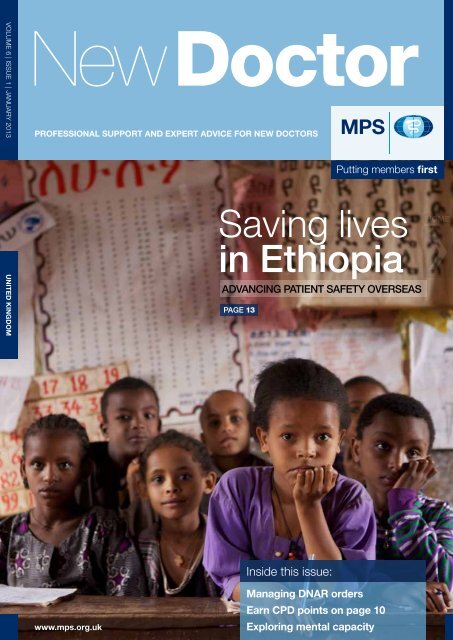
13From ward to worldFROM WARD TO WORLDSaving lives in Ethiopia© IMAGES/VSO/PHOTGRAPHER BEN LANGDONEthiopia has one <strong>an</strong>aesthetist for every 5.3 million people. Dr TomBashford won the Patient Safety Award from the Association <strong>of</strong>Anaesthetists for his work promoting safer surgery in EthiopiaThere are fewer<strong>an</strong>aesthetists in thewhole <strong>of</strong> Ethiopia, acountry <strong>of</strong> 85 million, th<strong>an</strong>in the London hospital whereI work. I feel there is a moralobligation on countrieswith so m<strong>an</strong>y trained healthpr<strong>of</strong>essionals to supportvolunteer work overseas.I recently returned from <strong>an</strong>out-<strong>of</strong>-programme careerbreak (OOPC) during mycore <strong>an</strong>aesthetic training,where I worked in a largepublic hospital in AddisAbaba, the capital city <strong>of</strong>Ethiopia.Volunteering as a juniordoctor in the developingworld is challenging. Thereare difficult boundariesto negotiate to ensure youremain within the limits<strong>of</strong> your competence whilstbeing useful. I startedmy placement by reviewingthe existing <strong>an</strong>aestheticpractice in the hospital againstinternational st<strong>an</strong>dards. I thenused <strong>this</strong> as a tool to pl<strong>an</strong>a number <strong>of</strong> interventionsthat seemed likely to be bothsustainable <strong>an</strong>d carry a highlikelihood <strong>of</strong> improving patientoutcomes.As a result <strong>of</strong> my work, fiveprojects were implemented:<strong>an</strong>aesthetic pre-assessment,the WHO SSC, continuouspulse oximetry monitoringin recovery areas, improvedobservation protocolsin recovery areas, <strong>an</strong>d thedevelopment <strong>of</strong> a highdependencyunit (HDU).While <strong>this</strong> sounds ambitious,there are a huge number<strong>of</strong> charities aiming to worktoward improving healthinternationally <strong>an</strong>d one <strong>of</strong> theprivileges <strong>of</strong> being a longtermvolunteer is the ch<strong>an</strong>ceto act as a conduit for thesein a single institution.One large problem Iidentified was that patientswere dying or sufferingbrain damage on the wardsbecause their oxygenlevels were dropping <strong>an</strong>dover-stretched staff weren’tspotting <strong>this</strong> until it was toolate. I increasingly found thatdespite having been donatedthe necessary equipment (eg,pulse oximeters), m<strong>an</strong>y staffneeded training in how touse the equipment effectively.We were able to confidentlydeliver <strong>this</strong> training.I received support <strong>an</strong>dfunding from VSO, the ClintonHealth Access Initiative(CHAI) Ethiopia, The YaleGlobal Health LeadershipInstitute, University CollegeLondon Hospitals (UCLH)Charitable Foundation, RotaryInternational <strong>an</strong>d the LifeboxFoundation. In additionwe were given permissionto use the Immediate LifeSupport Guidelines <strong>of</strong> theResuscitation Council UKto prepare teaching aids <strong>an</strong>dprotocols. All the work wasdeveloped in conjunctionwith local staff leaders withthe aim <strong>of</strong> making a lasting<strong>an</strong>d sustainable differenceto the working <strong>of</strong> thedepartment.Volunteering as a junioris daunting, but we shouldnot underestimate thevalue <strong>of</strong> our training <strong>an</strong>dskills. Long-term volunteeringrepresents a ch<strong>an</strong>ce tomake a lasting differencewhile developing areas<strong>of</strong> your own practice that arehard to exp<strong>an</strong>d within theconfines <strong>of</strong> the NHS trainingladder. I would encouragenew doctors to take up thechallenge.For more information please visit www.vso.org.uk or www.aagbi.org/international/volunteer-opportunities-overseas. Dr Bashford c<strong>an</strong> becontacted on tom.bashford@doctors.org.uk. Watch a video about hisproject here – www.medicalprotection.org/uk/videos/road-to-safersurgery.NEW DOCTOR | VOLUME 6 | ISSUE 1 | 2013 | UNITED KINGDOM www.mps.org.uk
MEDICAL PROTECTION SOCIETYPROFESSIONAL SUPPORT AND EXPERT ADVICEHow to contact usVOLUME 6 | ISSUE 1 | JANUARY 2013THE MEDICAL PROTECTION SOCIETY33 Cavendish SquareLondon, W1G 0PSUnited Kingdomwww.mps.org.ukwww.dentalprotection.orgGeneral enquiries (UK)T 0845 605 4000F 0113 241 0500E info@mps.org.ukMPS EDUCATION AND RISK MANAGEMENTMPS Education <strong>an</strong>d Risk M<strong>an</strong>agement is a dedicated divisionproviding risk m<strong>an</strong>agement education, training <strong>an</strong>d consult<strong>an</strong>cy.T 0113 241 0696F 0113 241 0710E education@mps.org.ukPlease direct all comments, questions or suggestionsabout MPS service, policy <strong>an</strong>d operations to:Chief Executive<strong>Medical</strong> <strong>Protection</strong> <strong>Society</strong>33 Cavendish SquareLondon W1G 0PSUnited Kingdomchief.executive@mps.org.ukIn the interests <strong>of</strong> confidentiality please do not include informationin <strong>an</strong>y email that would allow a patient to be identified.What our members sayabout our service:96% <strong>of</strong> members said they wouldbe likely or very likely to recommendMPS to their colleagues.92% scored good, very good orexcellent for the service they receivedfrom our medicolegal advisers.94% scored good, very good orexcellent for the service they receivedfrom our membership team.UNITED KINGDOMwww.mps.org.uk/new-doctorThe <strong>Medical</strong> <strong>Protection</strong> <strong>Society</strong> is the leading provider <strong>of</strong> comprehensive pr<strong>of</strong>essionalindemnity <strong>an</strong>d expert advice to doctors, dentists <strong>an</strong>d health pr<strong>of</strong>essionals around the world.MPS is not <strong>an</strong> insur<strong>an</strong>ce comp<strong>an</strong>y. All the benefits <strong>of</strong> membership <strong>of</strong> MPSare discretionary as set out in the Memor<strong>an</strong>dum <strong>an</strong>d Articles <strong>of</strong> Association.The <strong>Medical</strong> <strong>Protection</strong> <strong>Society</strong> Limited. A comp<strong>an</strong>y limited by guar<strong>an</strong>tee.Registered in Engl<strong>an</strong>d No. 36142 at 33 Cavendish Square, London, W1G 0PSNew Doctor (UK ed. Print) ISSN 2042-4175New Doctor (UK ed. Online) ISSN 2042-4183