Application form for Elderly care
Application form for Elderly care
Application form for Elderly care
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
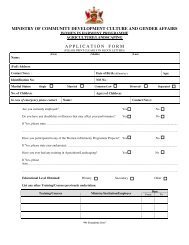
MINISTRY OF COMMUNITY DEVELOPMENT CULTURE AND GENDER AFFAIRSWOMEN IN HARMONY PROGRAMMEELDERLY CAREName: Miss/ Mrs./MsA P P L I C A T I O N F O R M(PLEASE PRINT CLEARLY IN BLOCK LETTERS)(First) (Middle) (Last)(Full) Address:Contact No(s). : Date of Birth (dd/mm/yy): Age:Identification No.:NIS No.:Marital Status: Single Married Common-Law Divorced SeparatedNo. of Children:Age(s) of Children:In case of emergency please contact Name: Contact No(s):Are you currently employed? Yes NoDo you have any disabilities or illnesses that may affect your per<strong><strong>for</strong>m</strong>ance? Yes NoIf Yes, pleasestate………………………………………………………………………………………………………………………………..…………………………………………………………………………………………………………………………………….Have you participated in any of the Women in Harmony Programme Projects? YesNoIf Yes, please state year and project: …………………………………………………………………………………..................Have you ever had any training in <strong>Elderly</strong> Care? Yes NoIf Yes, pleasestate………………………………………………………………………………………………………………………………..…………………………………………………………………………………………………………………………………….Educational Level Obtained: Primary Secondary OtherList any other Training/Courses previously undertaken:DateTraining/Courses Ministry/Institution/Employer From To“We Trans<strong><strong>for</strong>m</strong> Lives”
List two (2) references:(1) Name:………………………………………………………... Address:………………..………………..………………………Telephone No.: ……………………..………………………. Profession:……………………………………………................(2) Name:………………………………………………………... Address:………………..………………..…………………........Telephone No.: ……………………..…………………….... Profession:……………………………………………................I hereby declare that the in<strong><strong>for</strong>m</strong>ation given on this <strong><strong>for</strong>m</strong> is true, complete and accurate to the best of my knowledge. I furtherunderstand that any false statement made could lead to my dismissal from this programme.……………………………………………..Applicant’s Signature….…………………………DateOfficial Use Only………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………WOMEN IN HARMONY PROGRAMME, CARIFESTA HOUSE, 8 A STANMORE AVENUE, PORT OF SPAIN.TELEPHONE: 625-3955/3952; 625-3012/3112. FAX: 627-8303. E-MAIL: gender@cdcga.gov.tt“We Trans<strong><strong>for</strong>m</strong> Lives”