nerve conduction studies: essentials and pitfalls in practice
nerve conduction studies: essentials and pitfalls in practice
nerve conduction studies: essentials and pitfalls in practice
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Downloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comNEUROLOGY IN PRACTICEii24Box 1: List of abbreviations <strong>and</strong> term<strong>in</strong>ologyusedcccccccccccccccccccccACh: acetylchol<strong>in</strong>eAIDP: acute <strong>in</strong>flammatory demyel<strong>in</strong>at<strong>in</strong>g polyneuropathyAMAN: acute motor axonal neuropathyCMAP: compound muscle action potentialCN: cl<strong>in</strong>ical neurophysiologistDRG: dorsal root ganglionEMG: electromyogramLEMS: Lambert-Eaton myasthenic syndromeMG: myasthenia gravisNAP: <strong>nerve</strong> action potentialNCS: <strong>nerve</strong> <strong>conduction</strong> <strong>studies</strong>NMTD: neuromuscular transmission disordersPNE: peripheral neurophysiological exam<strong>in</strong>ationPNS: peripheral nervous systemRNS: repetitive <strong>nerve</strong> stimulationSNAP: sensory <strong>nerve</strong> action potentialTMS: transcranial magnetic stimulationConduction block: A reduction of proximal CMAP area/amplitude of at least 20% (usually . 50%) compared withdistal CMAP area/amplitude. The duration of theproximal CMAP should not <strong>in</strong>crease by . 20% (seetemporal dispersion)Temporal dispersion: A reduction <strong>in</strong> proximal CMAPamplitude compared with distal CMAP amplitude whenthe proximal CMAP duration <strong>in</strong>creases by . 20%Orthodromic: Nerve action potentials carried <strong>in</strong> thephysiological directionAntidromic: Nerve action potentials carried <strong>in</strong> thedirection opposite to the physiologicalsyndrome it is unnecessary to ask for ‘‘NCS of the rightmedian <strong>nerve</strong>’’. (The wise CN will study both median <strong>nerve</strong>sanyway as this condition is frequently bilateral.)Basic <strong>nerve</strong> <strong>and</strong> muscle physiologyThe referr<strong>in</strong>g doctor needs only a m<strong>in</strong>imal knowledge of basic<strong>and</strong> applied physiology to underst<strong>and</strong> the test results, but allPNE reports should be written <strong>in</strong> terms that do not assumespecialist knowledge. A m<strong>in</strong>imum knowledge set to underst<strong>and</strong>the pr<strong>in</strong>ciples of the techniques is shown <strong>in</strong> box 2 withl<strong>in</strong>ks to more detail.The pr<strong>in</strong>cipals of <strong>nerve</strong> <strong>conduction</strong> <strong>studies</strong>NCS <strong>in</strong>volve the application of a depolaris<strong>in</strong>g square waveelectrical pulses to the sk<strong>in</strong> over a peripheral <strong>nerve</strong> produc<strong>in</strong>g:(1) a propagated <strong>nerve</strong> action potential (NAP) recordedat a distant po<strong>in</strong>t over the same <strong>nerve</strong>: <strong>and</strong> (2) a compoundmuscle action potential (CMAP) aris<strong>in</strong>g from the activationof muscle fibres <strong>in</strong> a target muscle supplied by the <strong>nerve</strong>. Inboth cases these may be recorded with surface or needleelectrodes.Surface electrodes are designed to give <strong>in</strong>formation aboutthe whole of a muscle stimulated, giv<strong>in</strong>g data for the timetaken for the fastest axons to conduct an impulse to themuscle <strong>and</strong> the size of the response.Needle electrodes for NCS give very accurate <strong>conduction</strong>time <strong>in</strong>formation, but because they record from only a smallarea of muscle or <strong>nerve</strong>, they give poor or, <strong>in</strong> the case of thelatter, more complex <strong>in</strong>formation mak<strong>in</strong>g numerical analysisdifficult. However, needle record<strong>in</strong>gs are most appropriatewhen severe muscle wast<strong>in</strong>g has occurred, or when the depthBox 2: M<strong>in</strong>imum basic physiological knowledgeto underst<strong>and</strong> <strong>nerve</strong> <strong>conduction</strong> <strong>studies</strong>c Membrane potential: genesis; threshold effects; effect ofmembrane damage; denervationc S<strong>in</strong>gle axon: saltatory <strong>and</strong> non-saltatory <strong>conduction</strong>;factors which determ<strong>in</strong>e <strong>conduction</strong> velocity: diameter,myel<strong>in</strong>ation, <strong>in</strong>ter-nodal distancec Whole <strong>nerve</strong> composition: fascicular structure; size <strong>and</strong><strong>conduction</strong> velocity distribution; afferent <strong>and</strong> efferentmodalities <strong>and</strong> their relative contributionc Neuromuscular transmission: <strong>nerve</strong> term<strong>in</strong>al function;transmitter production, storage <strong>and</strong> release; post-synapticmembrane structure <strong>and</strong> function; receptor dynamics;endplate potentials; propagated muscle action potentialsc External electrical/magnetic stimulation: local depolarisation;bidirectional propagation once depolarised;effects of sk<strong>in</strong> <strong>and</strong> subcutaneous tissue impedance;electrical <strong>in</strong>ductive effect of applied magnetic field;stimulation threshold depends on: membrane properties(accommodation),<strong>nerve</strong> fibre location <strong>and</strong> size withrespect to stimulatorc Muscle function: excitation contraction coupl<strong>in</strong>g; musclefibre types <strong>and</strong> function; fatigueFor an excellent <strong>in</strong>teractive physiological education toolsee Richard Carpenter’s Neurolab at http://www.cudos.ac.uk/web/copyright.htm.of a muscle under study makes a surface record<strong>in</strong>gimpossible.Nerves may be stimulated through the sk<strong>in</strong> with surfacestimulators, or via a needle placed close to a <strong>nerve</strong> or a <strong>nerve</strong>root. Sp<strong>in</strong>al root <strong>and</strong> cerebral cortical stimulation may also becarried out us<strong>in</strong>g transcutaneous magnetic stimulation(TMS) dealt with elsewhere <strong>in</strong> this issue. Thus the fulllength of the motor pathway may be assessed from cortex tocord, root, neuromuscular junction, <strong>and</strong> the contractileapparatus. Choice of the stimulation po<strong>in</strong>ts depends bothon the desire to ‘‘bracket’’ above <strong>and</strong> below the po<strong>in</strong>t of aproposed focal lesion <strong>and</strong> the anatomical availability of theappropriate structure.The aim of the NCSOur m<strong>in</strong>imum knowledge set above has shown us thatperipheral <strong>nerve</strong>s conta<strong>in</strong> many <strong>nerve</strong> fibres of differentdiameters, degrees of myel<strong>in</strong>ation, <strong>and</strong> afferent or efferentconnections. The NCS <strong>studies</strong> the fastest 20% of these fibres<strong>and</strong> the aim of the <strong>in</strong>vestigation is to document focal orcont<strong>in</strong>uous abnormalities <strong>in</strong> the length of the mixed, motoror sensory <strong>nerve</strong>. Particular attention is paid to the follow<strong>in</strong>gquestions as the test progresses:c Is the fastest <strong>conduction</strong> velocity normal?c Is the velocity gradient normal. Normally <strong>nerve</strong>s closer tothe neuraxis <strong>and</strong> more cephalad conduct faster than moredistal <strong>and</strong> caudal <strong>nerve</strong>s.c Is the CMAP normal <strong>in</strong> size <strong>and</strong> shape?c Does the CMAP alter <strong>in</strong> size, shape or duration betweenstimulation po<strong>in</strong>ts?– giv<strong>in</strong>g evidence for temporal dispersion (see terms, box 2).– giv<strong>in</strong>g evidence for <strong>conduction</strong> block (see terms, box 2).Normal values for NCSAge matched ‘‘Normal’’ values for NCS parameters are eitherderived from <strong>studies</strong> of groups of neurologically normalsubjects or culled from the literature. Regrettably <strong>in</strong> the viewwww.jnnp.com
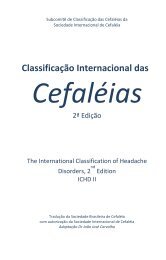
NEUROLOGY IN PRACTICEDownloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comii25Figure 1 (A, B). Median motor <strong>nerve</strong> <strong>conduction</strong> study. Active record<strong>in</strong>g electrode is over the APB muscle, with stimulation at the wrist, elbow, axilla,<strong>and</strong> brachial plexus. Panel B shows the motor response from stimulation at all four sites. Responses are of the same shape but the latency is longer withmore proximal stimulation. (C) The compound muscle action potential (CMAP) <strong>and</strong> its parameters.of the authors the most frequent statistics used are limits of95% or less frequently 99% confidence limits of a normalgroup to <strong>in</strong>dicate abnormality of a s<strong>in</strong>gle parameter.This approach may mislead as a crude separation between‘‘normal’’ <strong>and</strong> ‘‘abnormal’’ dilutes the <strong>in</strong>formation whereas aZ score, for example, <strong>in</strong>dicat<strong>in</strong>g the separation between as<strong>in</strong>gle value <strong>and</strong> the group mean expressed <strong>in</strong> SD, may bemore <strong>in</strong>formative. Alternatively, (a) a number of electrophysiologicalparameters may be taken together either as an‘‘<strong>in</strong>dex’’ or ‘‘score’’, or (b) the neurophysiologist assesses anumber of parameters together to make a judgement as towhether a cl<strong>in</strong>ically relevant numerical abnormality shouldbe emphasised <strong>in</strong> the report <strong>in</strong>terpretation or not.There are a number of physical parameters that requirecorrection or allowance for. The most important is temperature.The fastest motor <strong>nerve</strong> <strong>conduction</strong> velocity (FMNCV) isreduced by approximately 1 m/s per ˚C temperature fall.Conventionally, <strong>studies</strong> are performed as close to a surfacerecorded temperature of 34 ˚C. If that is not achieved byadequate heat<strong>in</strong>g or the limb, rarely a temperature correctionmust be applied. Some measures of <strong>conduction</strong> requirecorrection for limb length or height. F<strong>in</strong>ally <strong>nerve</strong> <strong>conduction</strong>data alter with age. The motor <strong>conduction</strong> slows by 0.4–1.7 m/s per decade after 20 years <strong>and</strong> the sensory by 2–4 m/s.SPECIFIC NERVE CONDUCTION STUDYTECHNIQUESMotor <strong>nerve</strong> <strong>conduction</strong> <strong>studies</strong>Motor <strong>studies</strong> are performed by electrical stimulation of a<strong>nerve</strong> <strong>and</strong> record<strong>in</strong>g the compound muscle action potential(CMAP) from surface electrodes overly<strong>in</strong>g a muscle suppliedby that <strong>nerve</strong>.The record<strong>in</strong>g electrodes are performed us<strong>in</strong>g adhesiveconductive pads placed onto the sk<strong>in</strong> overly<strong>in</strong>g the targetmuscle. The active electrode is placed over the muscle belly<strong>and</strong> the reference over an electrically <strong>in</strong>active site (usually themuscle tendon). A ground electrode is also placed somewherebetween the stimulat<strong>in</strong>g <strong>and</strong> record<strong>in</strong>g electrodes provid<strong>in</strong>g azero voltage reference po<strong>in</strong>t. The median motor study might<strong>in</strong>volve stimulation at the wrist, the elbow, <strong>and</strong> lessfrequently the axilla <strong>and</strong> the brachial plexus (fig 1A,B).The CMAP is a summated voltage response from the<strong>in</strong>dividual muscle fibre action potentials. The shortest latencyof the CMAP is the time from stimulus artefact to onset of theresponse <strong>and</strong> is a biphasic response with an <strong>in</strong>itial upwarddeflection followed by a smaller downward deflection. TheCMAP amplitude is measured from basel<strong>in</strong>e to negative peak(the neurophysiological convention is that negative voltage isdemonstrated by an upward deflection) <strong>and</strong> measured <strong>in</strong>millivolts (mV) (fig 1C).To record the CMAP, the stimulat<strong>in</strong>g current or voltage isgradually <strong>in</strong>creased until a po<strong>in</strong>t is reached where an <strong>in</strong>crease<strong>in</strong> stimulus produces no <strong>in</strong>crement <strong>in</strong> CMAP amplitude. It isonly at this (supramaximal) po<strong>in</strong>t that reproducible valuesfor CMAP amplitude <strong>and</strong> the latency between the stimulus<strong>and</strong> the onset of the CMAP can be recorded accurately.The <strong>nerve</strong> is then stimulated at a more proximal site—<strong>in</strong>the median <strong>nerve</strong> this will be the antecubital fossa, close tothe biceps tendon. In the normal state stimulat<strong>in</strong>g themedian <strong>nerve</strong> at the wrist <strong>and</strong> the elbow results <strong>in</strong> twowww.jnnp.com
R M E D I A N - A P B1 .21 .31 .41 .51 .61 .71 .81 .91 .1 05 0 m s 5 0 0 µ VDownloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comNEUROLOGY IN PRACTICEMii26CellbodyAxonF waveStimulusMMuscleFFigure 2 Median orthodromic sensory study. The <strong>in</strong>dex f<strong>in</strong>ger digital<strong>nerve</strong>s are stimulated via r<strong>in</strong>g electrodes <strong>and</strong> the response recordedover the median <strong>nerve</strong> at the wrist.CMAPs of similar shape <strong>and</strong> amplitude because the samemotor axons <strong>in</strong>nervate the muscle fibres mak<strong>in</strong>g up theresponse. However, the latency will be greater for elbowstimulation compared with wrist stimulation because of thelonger distance between the stimulat<strong>in</strong>g <strong>and</strong> record<strong>in</strong>gelectrodes (fig 1B). The difference <strong>in</strong> latency represents thetime taken for the fastest <strong>nerve</strong> fibres to conduct between thetwo stimulation po<strong>in</strong>ts as all other factors <strong>in</strong>volv<strong>in</strong>gneuromuscular transmission <strong>and</strong> muscle activation arecommon to both stimulation sites. If one measures thedistance between the two sites then the fastest motor <strong>nerve</strong><strong>conduction</strong> velocity can be calculated as follows: FMNCV(m/s) = distance between stimulation site 1 <strong>and</strong> site 2(mm)/[latency site 2 – latency site 1 (ms)].Sensory <strong>conduction</strong> <strong>studies</strong>The sensory <strong>nerve</strong> action potential (SNAP) is obta<strong>in</strong>ed byelectrically stimulat<strong>in</strong>g sensory fibres <strong>and</strong> record<strong>in</strong>g the <strong>nerve</strong>action potential at a po<strong>in</strong>t further along that <strong>nerve</strong>. Onceaga<strong>in</strong> the stimulus must be supramaximal.Record<strong>in</strong>g the SNAP orthodromically refers to distal <strong>nerve</strong>stimulation <strong>and</strong> record<strong>in</strong>g more proximally (the direction <strong>in</strong>which physiological sensory <strong>conduction</strong> occurs). Antidromictest<strong>in</strong>g is the reverse. Different laboratories prefer antidromicor orthodromic methods for test<strong>in</strong>g different <strong>nerve</strong>s. Anorthodromic median sensory study is shown <strong>in</strong> fig 2. Thesensory latency <strong>and</strong> the peak to peak amplitude of the SNAPare measured. The velocity correlates directly with thesensory latency <strong>and</strong> therefore either the result may beexpressed as a latency over a st<strong>and</strong>ard distance or a velocity.Only the 20% largest diameter <strong>and</strong> fastest conduct<strong>in</strong>gsensory fibres are tested us<strong>in</strong>g conventional sensory <strong>studies</strong>functionally supply<strong>in</strong>g f<strong>in</strong>e touch, vibration, <strong>and</strong> positionsense. Predom<strong>in</strong>antly small fibre neuropathies affect<strong>in</strong>g theother 80% of fibres exist usually with prom<strong>in</strong>ent symptoms ofpa<strong>in</strong> <strong>and</strong> conventional sensory <strong>studies</strong> may be normal. Insuch cases quantitative sensory test<strong>in</strong>g <strong>and</strong> autonomictest<strong>in</strong>g will be required, which are beyond the scope of thisarticle (see Interpretation <strong>pitfalls</strong>).FwavesF waves (F for foot where they were first described) are a typeof late motor response. When a motor <strong>nerve</strong> axon iselectrically stimulated at any po<strong>in</strong>t an action potential ispropagated <strong>in</strong> both directions away from the <strong>in</strong>itial stimulationsite. The distally propagated impulse gives rise to theMFFigure 3 Schematic representation of the early M response from thedistally propagated action potential <strong>and</strong> the later F wave from theproximally propagated action potential. The latter depolarises the axonhillock caus<strong>in</strong>g it to backfire. Actual F wave responses are shown <strong>in</strong> thelower trace. F waves vary <strong>in</strong> latency <strong>and</strong> shape due to differentpopulations of axons backfir<strong>in</strong>g each time.CMAP. However, an impulse also conducts proximally to theanterior horn cell, depolaris<strong>in</strong>g the axon hillock <strong>and</strong> caus<strong>in</strong>gthe axon to backfire. This leads to a small additional muscledepolarisation (F wave) at a longer latency. Only about 2% ofaxons backfire with each stimulus. Unlike the M response(fig 3), F waves vary <strong>in</strong> latency <strong>and</strong> shape because differentpopulations of neurones normally backfire with eachstimulus. The most reliable measure of the F wave is them<strong>in</strong>imum latency of 10–20 fir<strong>in</strong>gs.Why are F waves useful?F waves allow test<strong>in</strong>g of proximal segments of <strong>nerve</strong>s thatwould otherwise be <strong>in</strong>accessible to rout<strong>in</strong>e <strong>nerve</strong> <strong>conduction</strong><strong>studies</strong>. F waves test long lengths of <strong>nerve</strong>s whereas motor<strong>studies</strong> test shorter segments. Therefore F wave abnormalitiescan be a sensitive <strong>in</strong>dicator of peripheral <strong>nerve</strong> pathology,particularly if sited proximally. The F wave ratio whichcompares the <strong>conduction</strong> <strong>in</strong> the proximal half of the totalpathway with the distal may be used to determ<strong>in</strong>e the site of<strong>conduction</strong> slow<strong>in</strong>g—for example, to dist<strong>in</strong>guish a root lesionfrom a patient with a distal generalised neuropathy.ErrorsThe ma<strong>in</strong> sources of non-biological error <strong>in</strong> NCS measurementsare the identification <strong>and</strong> measurement of waveformonset <strong>and</strong> the measurement of the length of the <strong>nerve</strong>segment on the limb. Calculations have shown that <strong>in</strong> a <strong>nerve</strong>with a <strong>conduction</strong> velocity of 50 m/s, the 26SD experimentalerror for velocity is 14 m/s over 10 cm <strong>and</strong> 4.7 m/s over25 cm. Of the error, time measurement is 92.3% <strong>and</strong> distance7.7%, so the use of the measur<strong>in</strong>g tape is quite adequate <strong>in</strong>conventional NCS.www.jnnp.com
NEUROLOGY IN PRACTICEDownloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comTable 1Typical <strong>nerve</strong> <strong>conduction</strong> study abnormalities seen with axon loss or demyel<strong>in</strong>ationAxon lossDemyel<strong>in</strong>ationSensory responses Small or absent Small or absentDistal motor latency Normal or slightly prolonged ProlongedCMAP amplitude Small Normal (reduced if <strong>conduction</strong> block or temporal dispersion)Conduction block/temporal dispersion Not present (responses may disperse slightly) PresentMotor <strong>conduction</strong> velocity Normal or slightly reduced Notably reducedF waves m<strong>in</strong>imum latency Normal or slightly prolonged Significantly prolongedii27It is not necessary to have all the features of axon loss or demyel<strong>in</strong>ation to come to a conclusion. Some conditions only affect motor or sensory <strong>nerve</strong>s, <strong>and</strong> someprocesses are length dependent <strong>and</strong> others universal. It can sometimes be quite difficult to decide whether a process is primarily demyel<strong>in</strong>at<strong>in</strong>g or demyel<strong>in</strong>at<strong>in</strong>gwith secondary axonal changes as features of both may coexist.NERVE CONDUCTION STUDIES IN DISEASEGeneralNCS provides <strong>in</strong>formation to locate lesions <strong>in</strong> the length of a<strong>nerve</strong>, <strong>and</strong> pathophysiological <strong>in</strong>formation. Peripheral <strong>nerve</strong>pathology primarily affects axons or myel<strong>in</strong>. In reality, thetwo pathologies often co-exist but usually one predom<strong>in</strong>ates(table 1).In focal lesions characterisation of the pathophysiologicalprocess can be important for determ<strong>in</strong><strong>in</strong>g prognosis. Apatient with a radial <strong>nerve</strong> palsy at the spiral groove caus<strong>in</strong>gwrist drop is more likely to make a complete <strong>and</strong> speedierrecovery (6–12 weeks) if this is ma<strong>in</strong>ly due to focaldemyel<strong>in</strong>ation <strong>and</strong>/or <strong>conduction</strong> block (neuropraxia) comparedwith when significant axonal <strong>in</strong>jury has also occurred(6–12 months).In generalised processes it is also important to determ<strong>in</strong>ewhether a peripheral neuropathy is demyel<strong>in</strong>at<strong>in</strong>g or axonalas this will affect further <strong>in</strong>vestigation <strong>and</strong> management. Forexample, acute <strong>in</strong>flammatory demyel<strong>in</strong>at<strong>in</strong>g polyneuropathy(AIDP or Guilla<strong>in</strong>-Barré syndrome) results <strong>in</strong> a characteristicpattern of segmental <strong>nerve</strong> demyel<strong>in</strong>ation <strong>and</strong> may be treatedwith human immunoglobul<strong>in</strong> or plasma exchange.Conversely a length dependent axonal neuropathy develop<strong>in</strong>g<strong>in</strong> a patient on chemotherapy requires reassessment ofthe chemotherapy or addition of a protective agent.Neuropathies may be classified pathologically <strong>in</strong> thisfashion, anatomically or electrophysiologically.Motor NCSIn axonal lossThe most strik<strong>in</strong>g abnormality is a reduction <strong>in</strong> CMAPamplitude as fewer function<strong>in</strong>g motor axons are connected tomuscle fibres. S<strong>in</strong>ce myel<strong>in</strong> is unaffected, the rema<strong>in</strong><strong>in</strong>gaxons conduct normally <strong>and</strong> one would expect latencies <strong>and</strong><strong>conduction</strong> velocities to rema<strong>in</strong> normal. However, with<strong>in</strong>creas<strong>in</strong>g motor axon loss some of the largest fastestconduct<strong>in</strong>g fibres will be lost. Therefore distal motor latencymay be slightly prolonged (, 120% of normal limit) <strong>and</strong><strong>conduction</strong> velocity slightly slowed (. 80% of normal limit).The dynamics <strong>and</strong> tim<strong>in</strong>g of an axonal <strong>in</strong>sult can affect theabnormalities seen. Immediately after a traumatic completetransection of the <strong>nerve</strong>, the portion of the <strong>nerve</strong> distal to thelesion will be normal as there has not been time for axonaldegeneration to occur. The CMAP amplitude will only start tofall a few days later. Conversely, if there is a very slow loss ofaxons <strong>in</strong> a generalised neuropathy, the rema<strong>in</strong><strong>in</strong>g unaffectedaxons may have time to sprout new connections to musclefibres that have lost their <strong>in</strong>nervation (collateral re<strong>in</strong>nervation)<strong>and</strong> the CMAP may rema<strong>in</strong> with<strong>in</strong> the normalamplitude range even though the total number of <strong>nerve</strong>axons is smaller. However, the immature regenerat<strong>in</strong>g fibreshave slower velocities due to the effect of the short <strong>in</strong>ternodaldistances <strong>and</strong> this produces a more dispersed CMAP.In demyel<strong>in</strong>ationWith loss of myel<strong>in</strong> thickness <strong>nerve</strong> <strong>conduction</strong> is slowed<strong>and</strong>, if severe enough, saltatory <strong>conduction</strong> fails (<strong>conduction</strong>block). NCS shows severely prolonged motor latencies <strong>and</strong>notably slowed <strong>conduction</strong> velocities. The precise changesseen depend on the site <strong>and</strong> extent of demyel<strong>in</strong>ation. Ifdemyel<strong>in</strong>ation is very proximal then distal motor latency <strong>and</strong><strong>conduction</strong> velocity may be normal <strong>in</strong> which case only Fwaves may show abnormalities.Normal <strong>nerve</strong>Conduction blockTemporal dispersionResponses arrive atrecord<strong>in</strong>g electrodealmost together=DistalstimulationDemyel<strong>in</strong>ationTemporal dispersionProximalstimulationResponses arrive atdifferent timesphase cancellation=Figure 4 Both these traces show demyel<strong>in</strong>ation <strong>in</strong> median motor<strong>studies</strong>. The trace on the left shows almost complete <strong>conduction</strong> blockwith an absent response with proximal stimulation. The trace on theright shows temporal dispersion where the CMAP duration <strong>in</strong>creases byalmost 40% with proximal stimulation. In both situations the CMAPamplitude with proximal stimulation is smaller.Figure 5 Schematic representation of phase cancellation <strong>and</strong>temporal dispersion <strong>in</strong> demyel<strong>in</strong>ation. In the normal <strong>nerve</strong>, theresponses are synchronised <strong>in</strong> time <strong>and</strong> therefore summate (amplitudeis higher that that of the <strong>in</strong>dividual components). Temporal dispersionresults <strong>in</strong> an <strong>in</strong>creased duration <strong>and</strong> reduced amplitude of CMAP.www.jnnp.com
123R ULNA R- Ort ho -V4V 110ms 10µV10123R ULNA R- Ort ho -V4V 110ms 10µV10Downloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comNEUROLOGY IN PRACTICEii28Sp<strong>in</strong>alcordNo lesion Pre-ganglionic lesion Post-ganglionic lesionDRGFigure 6 Sensory responses arenormal <strong>in</strong> pre-ganglionic lesions eventhough sensation may be abnormalcl<strong>in</strong>ically. Post-ganglionic lesions result<strong>in</strong> abnormal sensory responses. DRG,dorsal root ganglion.NormalsensationAbnormalsensationAbnormalsensationNormal SNAP Normal SNAP Abnormal SNAPConduction block or temporal dispersion both result <strong>in</strong> areduction <strong>in</strong> CMAP amplitude. The CMAP area is used toassess the contribution of these two processes. In <strong>conduction</strong>block there is complete failure of <strong>conduction</strong> <strong>in</strong> some or all ofthe motor axons studied. Therefore the CMAP area withstimulation proximal to site of <strong>conduction</strong> block is smaller(. 20% reduction) compared with distal stimulation (fig 4).For true <strong>conduction</strong> block to be detected, the proximal CMAPduration must not <strong>in</strong>crease by . 20%. In temporal dispersion(fig 4) there is a loss of synchrony <strong>in</strong> the <strong>nerve</strong> actionpotentials result<strong>in</strong>g <strong>in</strong> a loss of CMAP amplitude because thepositive part of one muscle fibre action potential cancels outthe negative part of another (phase cancellation) (fig 5).Cl<strong>in</strong>ical correlates of motor <strong>conduction</strong> velocity slow<strong>in</strong>g <strong>and</strong><strong>conduction</strong> blockIt is important to realise that slow<strong>in</strong>g of <strong>conduction</strong> velocityalone without <strong>conduction</strong> block does not result <strong>in</strong> weaknessas the impulses are still conducted from <strong>nerve</strong> to muscle. Agood example of this is the presence of profound slow<strong>in</strong>g ofmotor <strong>nerve</strong> <strong>conduction</strong> <strong>in</strong> totally asymptomatic primaryrelatives of patients with demyel<strong>in</strong>at<strong>in</strong>g hereditary motor <strong>and</strong>sensory neuropathy.Sensory NCSIn generalised disordersIn both axonal <strong>and</strong> demyel<strong>in</strong>at<strong>in</strong>g pathologies the SNAPamplitude is reduced for different reasons. Sensory axonalloss will result <strong>in</strong> a smaller SNAP. Demyel<strong>in</strong>ation alsoproduces small SNAPs but with prolonged durations. Asthey are of much shorter duration than CMAPs they are moresusceptible to phase cancellation (fig 5).The distribution of sensory NCS abnormalities may behelpful <strong>in</strong> determ<strong>in</strong><strong>in</strong>g aetiology. For example, the loss ofSNAPS <strong>in</strong> the lower limbs is common <strong>in</strong> an axonal dy<strong>in</strong>g backneuropathy related to drugs like v<strong>in</strong>crist<strong>in</strong>e, whereas equal<strong>in</strong>volvement of upper <strong>and</strong> lower limb SNAPS raise thepossibility of a sensory ganglionopathy such as that related tothalidomide treatment.Focal lesionsMultiple sensory NCS allow the <strong>in</strong>vestigator to locate sensoryneuropathies that <strong>in</strong>volve s<strong>in</strong>gle or multiple digital <strong>nerve</strong>sdistally (for example, vasculitis or h<strong>and</strong> arm vibrationsyndrome) right up to the major trunks, cords, <strong>and</strong> divisionsof the brachial plexus proximally.In proximal <strong>nerve</strong> trauma, ma<strong>in</strong>tenance of the sensorypotential depends on the <strong>in</strong>tact cell bodies <strong>in</strong> the dorsal rootganglia. Thus sensory NCS are extremely useful <strong>in</strong> localis<strong>in</strong>ga PNS lesion as either pre- <strong>and</strong>/or post-ganglionic. In apatient with a cl<strong>in</strong>ically suspected C8, T1 root lesion <strong>and</strong> withappropriate anaesthesia <strong>in</strong> that dermatome, the absence ofthe ulnar <strong>and</strong> medial antebrachial cutaneous sensorypotential places the lesion distal to the dorsal root ganglion(DRG) <strong>in</strong> the lower trunk of the brachial plexus <strong>and</strong> not atroot level (fig 6). Needle EMG can then be used to def<strong>in</strong>e thisfurther.FwavesGeneralised disordersF waves are sensitive to all forms of generalised peripheralneuropathy with their absence or a prolonged m<strong>in</strong>imumlatency occurr<strong>in</strong>g early. For example, <strong>in</strong> AIDP wheredemyel<strong>in</strong>ation may be segmental, proximal <strong>and</strong> patchy,F wave abnormalities may be the earliest <strong>and</strong> (<strong>in</strong> mild cases)the only electrophysiological abnormality seen.In axonal pathology F wave latencies may also be mildlydelayed <strong>in</strong> keep<strong>in</strong>g with the motor <strong>conduction</strong> velocityslow<strong>in</strong>g secondary to the loss of the fastest conduct<strong>in</strong>g motoraxons.In motor neuronopathies such as the motor neuronediseases, prolongation of any F wave latency is strongevidence either that this is the <strong>in</strong>correct diagnosis (such as<strong>in</strong> multifocal motor neuropathy) or that a second pathologicalprocess is present.Focal lesionsF waves may be absent <strong>in</strong> focal peripheral <strong>nerve</strong> or anteriorsp<strong>in</strong>al disorders. They were <strong>in</strong>itially also thought to be verywww.jnnp.com
NEUROLOGY IN PRACTICEDownloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comPre-exerciseImmediately post-exercise1 m<strong>in</strong> post-exercise2 m<strong>in</strong> post-exerciseFigure 7 (A) Normal repetitive <strong>nerve</strong> stimulation from abductor digitim<strong>in</strong>imi muscle <strong>in</strong> the h<strong>and</strong>. The amplitude of the CMAPs with<strong>in</strong> eachtra<strong>in</strong> does not decrement nor is there any significant <strong>in</strong>crement <strong>in</strong> CMAPamplitude after exercise. (B) Repetitive <strong>nerve</strong> stimulation <strong>in</strong> myastheniagravis from the nasalis muscle. Four stimulus tra<strong>in</strong>s are given—all atbasel<strong>in</strong>e with no exercise. A reproducible decrement of 55% is seen(tra<strong>in</strong> 3 is technically unsatisfactory because of movement artefact).REPETITIVE NERVE STIMULATIONRepetitive <strong>nerve</strong> stimulation (RNS) is used <strong>in</strong> the evaluationof patients with suspected neuromuscular transmissiondisorders (NMTD) such as myasthenia gravis (MG) orLambert-Eaton myasthenic syndrome (LEMS). RNS is amodified motor NCS where <strong>in</strong>stead of record<strong>in</strong>g CMAPs withs<strong>in</strong>gle supramaximal electrical stimuli, a tra<strong>in</strong> of 8–10 stimuliis applied <strong>and</strong> the sequential response amplitudes <strong>and</strong>/orareas measured. This may be carried out at low (3–4 Hz) orhigh frequency stimulation (20–50 Hz). In the latter case thetra<strong>in</strong> is prolonged to allow 2–10 seconds of cont<strong>in</strong>uous datato be measured. Both distal <strong>and</strong> proximal muscles/<strong>nerve</strong>sshould be studied <strong>in</strong> every patient suspected of an NMTD asthe sensitivity of the test is greatly <strong>in</strong>creased by this means.With low frequency stimulation <strong>in</strong> normal subjects, theCMAP amplitude <strong>and</strong>/or area falls over the first 4–5 stimuliby a maximum of 10–12%. The maximum fall should bebetween potentials 1 <strong>and</strong> 2 (see RNS <strong>pitfalls</strong>). A number ofdepartment specific protocols have been published to studythe RNS over time both before <strong>and</strong> after a period ofmaximum voluntary contraction of the muscle to pick upearly or late NMT failure (fig 7).High frequency stimulation may be used to discoverevidence of a post-synaptic transmitter release disorder likeLEMS. It is pa<strong>in</strong>ful <strong>and</strong> requires considerable patienttolerance. There is evidence that record<strong>in</strong>g low frequencyRNS immediately before <strong>and</strong> after a 20–30 second period ofmaximum voluntary contraction by the patient is equallysensitive <strong>and</strong> is more humane (fig 8).There are many <strong>pitfalls</strong> <strong>in</strong> the RNS test <strong>and</strong> artefact almostalways gives rise to an abnormal test. Thus adherence to astrict protocol <strong>and</strong> heightened suspicion on the part of the CNto an abnormal result is essential as are repeated <strong>studies</strong> forreproducibility of abnormalities (see RNS <strong>pitfalls</strong>).ii29useful <strong>in</strong> identify<strong>in</strong>g <strong>in</strong>dividual root distribution abnormalities.However, particularly <strong>in</strong> the upper limbs, the substantialoverlap of segmental <strong>in</strong>nervation <strong>in</strong> the distally availableperipheral <strong>nerve</strong>s makes this test on its own of low sensitivity<strong>and</strong> anatomical specificity. In addition, the effect ofdemyel<strong>in</strong>ation is diluted by the length of the path overwhich the F wave passes. In dist<strong>in</strong>guish<strong>in</strong>g the presence of adistal or proximal lesion, the use of the F wave ratio whichcompares the F wave latency <strong>in</strong> the upper <strong>and</strong> lower halves ofthe limb (conventionally us<strong>in</strong>g knee <strong>and</strong> elbow as thedivid<strong>in</strong>g l<strong>in</strong>e) may be useful.Physiological basis for the RNSThe neuromuscular junction consists of the motor axonterm<strong>in</strong>al, the synaptic cleft, <strong>and</strong> the post-synaptic musclemembrane. As the motor axon potential depolarises the <strong>nerve</strong>term<strong>in</strong>al, voltage gated calcium channels open <strong>in</strong>creas<strong>in</strong>g theconcentration of calcium <strong>in</strong> the pre-synaptic <strong>nerve</strong> term<strong>in</strong>al.This <strong>in</strong> turn facilitates the release of quanta of acetylchol<strong>in</strong>e(ACh) from the <strong>nerve</strong> term<strong>in</strong>al <strong>in</strong>to the synaptic cleft. AChb<strong>in</strong>ds to receptors on the post-synaptic membrane caus<strong>in</strong>gdepolarisation (end plate potential). The size of the end platepotential is dependent on the amount of ACh released <strong>and</strong> itsUlnar CMAPPre-exercisePost-exercise1234Pre-exercise0 secs post-exercise30 secs post-exercise1 m<strong>in</strong> post-exerciseFigure 8 These traces show typicalelectrophysiological features of a presynapticneuromuscular transmissiondisorder <strong>in</strong> a patient with LEMS. Thetraces on the left show a small amplitudeulnar CMAP that after exercise <strong>in</strong>creasesfourfold <strong>in</strong> amplitude. The traces on theright show repetitive <strong>nerve</strong> stimulation<strong>studies</strong>. The amplitude <strong>in</strong>creases postexercise.Tra<strong>in</strong>s 1, 3, <strong>and</strong> 4 show adecrement of 30% which repairs withexercise (tra<strong>in</strong> 2).www.jnnp.com
Downloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comNEUROLOGY IN PRACTICETable 2Performance of testsTechnique Pitfall Explanationii30Motor NCS Temperature A low FMNCV or long DL may relate to low sk<strong>in</strong> temperature. It should always be recorded <strong>and</strong> coollimbs heatedF waves No pathway length allowance Because of the long pathway, normal values have to be related to limb length, pathwaymeasurement or body heightMotor NCS Waveform measurements If the onset of the CMAP is positive—that is, a downward deflection—the active record<strong>in</strong>g electrodeis misplaced away from the motor po<strong>in</strong>t <strong>and</strong> spurious latency <strong>and</strong> amplitude values will occurIf an <strong>in</strong>itially positive go<strong>in</strong>g waveform is only seen <strong>in</strong> proximal median <strong>nerve</strong> stimulation there is alikelihood of an anatomic anomaly <strong>in</strong> the forearmMotor <strong>and</strong> sensoryNCSMotor <strong>and</strong> sensoryNCSInadequate numbers of <strong>nerve</strong>sstudiedIn order to determ<strong>in</strong>e whether abnormalities are focal, generalised, length dependent, a sample of<strong>nerve</strong>s <strong>in</strong> upper <strong>and</strong> lower limbs usually need to be studiedEven <strong>in</strong> simple entrapment neuropathies, <strong>studies</strong> should be bilateral <strong>and</strong> <strong>in</strong>clude at least one other<strong>nerve</strong> not under suspicion to exclude an underly<strong>in</strong>g generalised processInadequate range of stimulus sites Dependent on the cl<strong>in</strong>ical picture stimulation may be required proximally to detect focal proximalabnormality. However, particularly with root <strong>and</strong> plexus stimulation, care <strong>in</strong> ensur<strong>in</strong>g supramaximalstimulation is vitalMotor NCS Electrode position<strong>in</strong>g If optimal position<strong>in</strong>g not used, the <strong>in</strong>different electrode may contribute significantly to amplitudemeasurementsMotor NCS Nerve length measurement A flexible ruler/tape is necessary to follow the <strong>nerve</strong> path accuratelySome measurements around jo<strong>in</strong>ts are affected by flexion/extension of the jo<strong>in</strong>t. For example, theleast errors are found <strong>in</strong> ulnar NCS if the elbow is flexed to .100˚Motor NCS Not supramaximal If the CMAP is not recorded supramaximally at all sites, the measured FMNCV will be <strong>in</strong> error.Spurious <strong>conduction</strong> block may be seen if proximal <strong>nerve</strong> stimulation is not supramaximalMotor NCS Over stimulation If a <strong>nerve</strong> is stimulated with too high a current/voltage, adjacent <strong>nerve</strong>s may be recruited <strong>and</strong>produce spurious resultsSensory NCS Stimulus artefacts Particularly <strong>in</strong> the lower limb <strong>nerve</strong>s the stimulus may cause an artefact which alters the NAP shape.This must be allowed for <strong>in</strong> calculation if it cannot be abolishedSensory NCS Absent potentials In some <strong>nerve</strong>s, us<strong>in</strong>g the orthodromic technique, the 95% confidence limits may <strong>in</strong>clude zeromicrovolts. Thus an absent potential may not be ‘‘abnormal’’Motor <strong>and</strong> sensory NCS Normal values Failure to use age specific normal values <strong>in</strong> the very young <strong>and</strong> very old may lead to errorRNSInadequate position<strong>in</strong>g <strong>and</strong>movement restrictionInadequate facilitationToo short an analysis periodLimited sitesWrong testIf the record<strong>in</strong>g electrodes do not lie right over the motor po<strong>in</strong>t, a spurious decrement may becreated as the muscle contracts repeatedly. Care over position<strong>in</strong>g <strong>and</strong> ideally spl<strong>in</strong>tage of themuscle so that it rema<strong>in</strong>s isometric helpsPatients may need cont<strong>in</strong>uous encouragement to obta<strong>in</strong> 30–30 second maximal voluntarycontractionRNS tra<strong>in</strong>s should be followed for at least 3 m<strong>in</strong>utes (preferably 5) to pick up the occasional postfacilitationexhaustionThe sensitivity of RNS <strong>in</strong> NMT disorders is greatly <strong>in</strong>creased by study<strong>in</strong>g both proximal (nasalis,trapezius) muscles as well as distal (abductor digiti m<strong>in</strong>imi).As a rule of thumb, a patient who has an unequivocally normal edrophonium test will frequently alsohave a normal distal <strong>and</strong> proximal RNS test. In these circumstances the authors go straight to s<strong>in</strong>glefibre electromyography of an <strong>in</strong>termediate <strong>and</strong> proximal muscle as a more sensitive test.CMAP, compound muscle action potential; DL, distal latency; FMNCV, fastest motor <strong>nerve</strong> <strong>conduction</strong> velocity; NAP, <strong>nerve</strong> action potential; NCS, <strong>nerve</strong><strong>conduction</strong> <strong>studies</strong>; NMT, neuromuscular transmission; RNS, repetitive <strong>nerve</strong> stimulation.Table 3InterpretationPitfallExplanationOver<strong>in</strong>terpretation of results c A limited numerical abnormality must be reported but placed <strong>in</strong> the context of the cl<strong>in</strong>ical problem—for example, thef<strong>in</strong>d<strong>in</strong>g of a subcl<strong>in</strong>ical carpal tunnel abnormality on NCS does not make the diagnosis of carpal tunnel syndromec An NCS abnormality may relate to a previous <strong>and</strong> currently irrelevant <strong>in</strong>jury or operationOver simplification of results c All <strong>studies</strong> should be <strong>in</strong>terpreted together <strong>in</strong> case multiple diagnoses are present. Occum’s razor may be too sharp. Forexample, <strong>in</strong> a patient with obvious polymyositis, NCS should ideally be performed to del<strong>in</strong>eate any additionalcoexist<strong>in</strong>g neuropathyMis<strong>in</strong>terpretation of NCS results c If the FMNCV is normal, the patient may still have slow<strong>in</strong>g of <strong>conduction</strong> of other <strong>nerve</strong> fibres related to a neuropathyc If the SNAPS are normal <strong>in</strong> all respects the patient may still have a small fibre sensory neuropathy produc<strong>in</strong>g symptoms<strong>and</strong> signsc If a <strong>nerve</strong> is reported unstimulatable, th<strong>in</strong>k of anomalous <strong>in</strong>nervation or anatomical variation of <strong>nerve</strong> position beforeconclud<strong>in</strong>g pathologyMis<strong>in</strong>terpretation of RNS results c If a decrement cont<strong>in</strong>ues throughout the RNS tra<strong>in</strong>, this is probably artefactc If a decrement is found <strong>in</strong> RNS, it is not pathognomic of myasthenia gravis. It has been found to be abnormal <strong>in</strong> anumber of conditions with abnormal <strong>nerve</strong> term<strong>in</strong>al function (motor neurone disease, active axonal neuropathy) ormuscle membrane <strong>in</strong>stability (polymyositis)c While MG <strong>and</strong> LEMS are the most common NMT disorders, the unwary will miss correctly diagnos<strong>in</strong>g congenitalmyasthenic syndromes, botulism, drug <strong>and</strong> tox<strong>in</strong>s (for example, organophosphates), all of which have characteristicPNE patterns when all tests are <strong>in</strong>terpreted together with the cl<strong>in</strong>ical pictureFor the referrer c If the referr<strong>in</strong>g doctor has not asked a specific question of the CN <strong>in</strong>vestigator, they should not be surprised ifoccasionally their request for a PNE is misunderstoodc A PNE request should never be couched <strong>in</strong> ‘‘please exclude’’ terms. While probabilities may be discussed, totalexclusion of a diagnosis depends on non-biological errors such as sampl<strong>in</strong>gc In the UK, CN are a scarce resource, often struggl<strong>in</strong>g with large wait<strong>in</strong>g lists. Thus all referrals should be considered <strong>in</strong>terms of: (a) what knowledge will I ga<strong>in</strong> about my patient from this <strong>in</strong>vestigation? (b) Will the result change mymanagement? (c) How urgent should the request be?CN, cl<strong>in</strong>ical neurophysiologist; LEMS, Lambert Eaton myasthenic syndrome; MG, myasthenia gravis; PNE, peripheral neurophysiological exam<strong>in</strong>ation; SNAPS,sensory <strong>nerve</strong> action potentials.www.jnnp.com
NEUROLOGY IN PRACTICEDownloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comb<strong>in</strong>d<strong>in</strong>g to receptors. In the healthy state, the end platepotential reaches a threshold level <strong>and</strong> causes an actionpotential to be propagated along a muscle fibre result<strong>in</strong>g <strong>in</strong>muscle contraction. Normally there is a large safety factor forneuromuscular transmission with the amount of AChreleased per impulse several times that required to generatea threshold level end plate potential.In low frequency RNS, the rate of stimulation is such thatthe end plate physiology is stressed, but not to the level thatproduces the natural facilitation of NMT at greater stimulationfrequencies. Thus an abnormal fall (decrement) <strong>in</strong>CMAP amplitude <strong>and</strong>/or area at low stimulation rates<strong>in</strong>dicates a drop <strong>in</strong> the safety factor for transmission whetherfrom a pre- or post-synaptic cause.In high frequency stimulation natural facilitation isenhanced by pre-synaptic Ca ++ <strong>in</strong>flux <strong>and</strong> this may counteracta process such as LEMS where quantal release isdepressed.RNS <strong>in</strong> diseaseNMT disorders may be congenital or acquired <strong>and</strong> <strong>in</strong> broadterms can be thought of as pre-synaptic or post-synapticdepend<strong>in</strong>g on where the defect lies.Post-synaptic disorders of neuromuscular junctiontransmissionThe archetypal post-synaptic disorder is myasthenia gravis(MG) where antibodies to acetylchol<strong>in</strong>e receptors (AChR)cause degradation <strong>and</strong> <strong>in</strong>creased turnover of receptor as wellas macrophage <strong>in</strong>itiated post-synaptic membrane simplification.In MG the safety factor is lost because as AChRs aredepleted, less post-synaptic depolarisation occurs <strong>and</strong> someend plate potentials do not reach threshold for genesis of apropagated muscle membrane potential produc<strong>in</strong>g neuromuscularblock. If this process affects a significant proportionof the tested muscle end plates, the RNS basel<strong>in</strong>e tra<strong>in</strong> willshow a significant decrement (greater than 10%). Thedecrement is usually measured by compar<strong>in</strong>g the amplitudeof the third or fourth CMAP <strong>in</strong> the tra<strong>in</strong> to the first (fig 7B).Very often some slight facilitation reduces the decrementover potentials 7–10 of the tra<strong>in</strong>.An abnormal decrement<strong>in</strong>g RNS test is non-specific <strong>and</strong>can be seen <strong>in</strong> a number of circumstances where musclecontraction processes may fail with repetitive stimulation(see RNS <strong>pitfalls</strong>).Pre-synaptic disordersIn LEMS there are antibodies to voltage gated calciumchannels (pre-synaptic disorder) caus<strong>in</strong>g impaired release ofACh quanta. Low frequency RNS stimulation may produceexactly the same decrement as seen <strong>in</strong> MG with additionallya small <strong>in</strong>itial CMAP amplitude. Here calcium <strong>in</strong>flux <strong>in</strong>to the<strong>nerve</strong> term<strong>in</strong>al is reduced due to the action of voltage gatedcalcium channel antibodies <strong>and</strong> <strong>in</strong> turn ACh release <strong>in</strong>to thesynaptic cleft is reduced <strong>and</strong> some end plate potentials will besub-threshold.However, the diagnostic abnormality is of a significant. 100% <strong>in</strong>crement <strong>in</strong> the CMAP amplitude after exercise orfast repetitive stimulation. Exercise <strong>in</strong>creases calcium <strong>in</strong>flux<strong>and</strong> the CMAP amplitude may <strong>in</strong>crease by up to 10 times. Inthis case we are just compar<strong>in</strong>g the amplitude of the firstCMAP <strong>in</strong> the tra<strong>in</strong> before <strong>and</strong> after exercise (fig 8). Despitethis <strong>in</strong>crement, with<strong>in</strong> each low frequency tra<strong>in</strong> a furtherdecrement may occur due to ACh depletion.PITFALLSThere are many <strong>pitfalls</strong> that can trap the unwary both <strong>in</strong> theperformance <strong>and</strong> the <strong>in</strong>terpretation of the NCS <strong>and</strong> RNS. Forconvenience these are separated <strong>in</strong> tables 2 <strong>and</strong> 3. Thetechnical <strong>pitfalls</strong> more appropriately addressed to the readerwho is an expert or tra<strong>in</strong><strong>in</strong>g <strong>in</strong> CN are not <strong>in</strong>cluded.CONCLUSIONSNerve <strong>conduction</strong> <strong>studies</strong> as part of the PNE are an extensionof the cl<strong>in</strong>ical history <strong>and</strong> exam<strong>in</strong>ation <strong>and</strong> are important <strong>in</strong>the management of cranial <strong>and</strong> peripheral neuromusculardisease as well as contribut<strong>in</strong>g to diagnosis of sp<strong>in</strong>al cordlesions. NCS can be extremely useful both <strong>in</strong> localis<strong>in</strong>glesions <strong>and</strong> determ<strong>in</strong><strong>in</strong>g the pathological processes responsible.We have listed many of the <strong>pitfalls</strong> both for the CNcarry<strong>in</strong>g out <strong>and</strong> <strong>in</strong>terpret<strong>in</strong>g the tests as well as for thereferr<strong>in</strong>g doctor. For the former it is vital both to carry outtests accurately <strong>and</strong> reproducibly <strong>and</strong> to develop an <strong>in</strong>vestigationstrategy based on the patient’s symptoms <strong>and</strong> signsrather than a fixed protocol. The <strong>in</strong>vestigator should thenreport the results clearly <strong>and</strong> then place them <strong>in</strong> the contextof the cl<strong>in</strong>ical situation.For the neurologist or other referr<strong>in</strong>g doctor, it is equallyvital that the cl<strong>in</strong>ical questions asked are explicit <strong>and</strong>answerable for the most to be ga<strong>in</strong>ed from what can be aconsiderable <strong>in</strong>vestment <strong>in</strong> time <strong>and</strong> skills for the <strong>in</strong>vestigator<strong>and</strong> tolerance of discomfort <strong>in</strong> the patient. For the bestuse of scarce resources therefore tra<strong>in</strong><strong>in</strong>g <strong>and</strong> awareness ofall the techniques detailed <strong>in</strong> this monograph are essential aspart of general neurological tra<strong>in</strong><strong>in</strong>g...................Authors’ affiliationsA Mallik, A I Weir, Department of Cl<strong>in</strong>ical Neurophysiology, Institute ofNeurological Sciences, Southern General Hospital, Glasgow, UKREFERENCES1 Oh SJ. Pr<strong>in</strong>ciples of cl<strong>in</strong>ical electromyography case <strong>studies</strong>. Baltimore:Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s, 1998.c An extremely readable book with excellent explanatory sections on<strong>nerve</strong> <strong>conduction</strong> techniques <strong>and</strong> lots of case <strong>studies</strong>.2 B<strong>in</strong>nie C, Cooper R, Mauguière F, et al. Cl<strong>in</strong>ical neurophysiology Vol 1 & 2,Elsevier, 2004.c A reference text cover<strong>in</strong>g all aspects of cl<strong>in</strong>ical neurophysiology<strong>in</strong>clud<strong>in</strong>g <strong>nerve</strong> <strong>conduction</strong> <strong>studies</strong>. Primarily aimed towards thosetra<strong>in</strong><strong>in</strong>g <strong>in</strong> cl<strong>in</strong>ical neurophysiology.3 Kimura J, Facts, Fallacies, et al. Twenty-First annual Edward H LambertLecture. Muscle & Nerve 1997;20:777–87.c Reviews basic techniques, pr<strong>in</strong>ciples <strong>and</strong> <strong>pitfalls</strong> of <strong>nerve</strong> <strong>conduction</strong><strong>studies</strong>. An excellent <strong>in</strong>troduction to <strong>nerve</strong> <strong>conduction</strong> <strong>studies</strong>.4 DeLisa JA, Lee HJ, Baran EM, et al. Manual of <strong>nerve</strong> <strong>conduction</strong> velocity <strong>and</strong>cl<strong>in</strong>ical neurophysiology, 3rd ed. Baltimore: Lipp<strong>in</strong>cott Williams & Wilk<strong>in</strong>s,1994.c L<strong>in</strong>e draw<strong>in</strong>gs illustrate how to actually perform most <strong>nerve</strong> <strong>conduction</strong><strong>studies</strong>.5 BSCN website. www.bscn.org.uk/education.c Conta<strong>in</strong>s part of the Glasgow <strong>in</strong>teractive EMG course with examples ofall the abnormalities discussed as well as self assessment cases.6 Donofrio PD, Albers JW. Polyneuropathy: classification by <strong>nerve</strong> <strong>conduction</strong><strong>studies</strong> <strong>and</strong> electromyography. Muscle & Nerve 1990;13:889–903.ii31www.jnnp.com
Downloaded from jnnp.bmj.com on June 5, 2012 - Published by group.bmj.comNerve <strong>conduction</strong> <strong>studies</strong>: <strong>essentials</strong> <strong>and</strong><strong>pitfalls</strong> <strong>in</strong> <strong>practice</strong>A Mallik <strong>and</strong> A I WeirJ Neurol Neurosurg Psychiatry 2005 76: ii23-ii31doi: 10.1136/jnnp.2005.069138Updated <strong>in</strong>formation <strong>and</strong> services can be found at:http://jnnp.bmj.com/content/76/suppl_2/ii23.full.htmlReferencesEmail alert<strong>in</strong>gserviceThese <strong>in</strong>clude:This article cites 2 articleshttp://jnnp.bmj.com/content/76/suppl_2/ii23.full.html#ref-list-1Receive free email alerts when new articles cite this article. Sign up <strong>in</strong> thebox at the top right corner of the onl<strong>in</strong>e article.TopicCollectionsArticles on similar topics can be found <strong>in</strong> the follow<strong>in</strong>g collectionsDrugs: CNS (not psychiatric) (1237 articles)Immunology (<strong>in</strong>clud<strong>in</strong>g allergy) (1271 articles)Neuromuscular disease (939 articles)Peripheral <strong>nerve</strong> disease (480 articles)NotesTo request permissions go to:http://group.bmj.com/group/rights-licens<strong>in</strong>g/permissionsTo order repr<strong>in</strong>ts go to:http://journals.bmj.com/cgi/repr<strong>in</strong>tformTo subscribe to BMJ go to:http://group.bmj.com/subscribe/