Medical History Questionnaire - Student Health Center
Medical History Questionnaire - Student Health Center
Medical History Questionnaire - Student Health Center

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
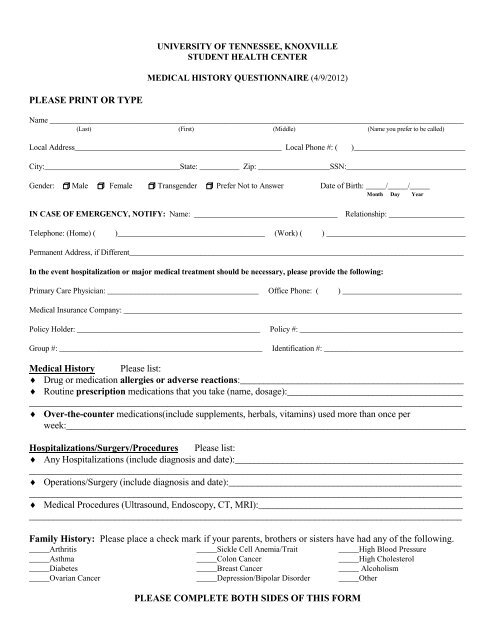
UNIVERSITY OF TENNESSEE, KNOXVILLESTUDENT HEALTH CENTERMEDICAL HISTORY QUESTIONNAIRE (4/9/2012)PLEASE PRINT OR TYPEName ________________________________________________________________________________________________________(Last) (First) (Middle) (Name you prefer to be called)Local Address____________________________________________________ Local Phone #: ()____________________________City:__________________________________State: __________ Zip: __________________SSN:______________________________Gender: Male Female Transgender Prefer Not to Answer Date of Birth: _____/_____/_____Month Day YearIN CASE OF EMERGENCY, NOTIFY: Name: ____________________________________ Relationship: ___________________Telephone: (Home) ( )_____________________________________ (Work) ( ) ___________________________________Permanent Address, if Different____________________________________________________________________________________In the event hospitalization or major medical treatment should be necessary, please provide the following:Primary Care Physician: ______________________________________ Office Phone: ( ) ______________________________<strong>Medical</strong> Insurance Company: _____________________________________________________________________________________Policy Holder: ______________________________________________Group #: ___________________________________________________Policy #: _________________________________________Identification #: ___________________________________<strong>Medical</strong> <strong>History</strong> Please list:♦ Drug or medication allergies or adverse reactions:_______________________________________________♦ Routine prescription medications that you take (name, dosage):________________________________________________________________________________________________________________________________♦ Over-the-counter medications(include supplements, herbals, vitamins) used more than once perweek:____________________________________________________________________________________Hospitalizations/Surgery/Procedures Please list:♦ Any Hospitalizations (include diagnosis and date):___________________________________________________________________________________________________________________________________________♦ Operations/Surgery (include diagnosis and date):____________________________________________________________________________________________________________________________________________♦ <strong>Medical</strong> Procedures (Ultrasound, Endoscopy, CT, MRI):______________________________________________________________________________________________________________________________________Family <strong>History</strong>: Please place a check mark if your parents, brothers or sisters have had any of the following._____Arthritis _____Sickle Cell Anemia/Trait _____High Blood Pressure_____Asthma _____Colon Cancer _____High Cholesterol_____Diabetes _____Breast Cancer _____ Alcoholism_____Ovarian Cancer _____Depression/Bipolar Disorder _____OtherPLEASE COMPLETE BOTH SIDES OF THIS FORM
Please place a check mark beside any of the following that you have had:__Anemia __ Anxiety/Panic disorder __Chronic Pain__Blood Transfusion __Depression/Bipolar Disorder __Frequent Headaches/Migraines__Sickle Cell Anemia/Trait __ ADD/ADHD __Seizures/Epilepsy__Bleeding disorder __ Eating disorder __Arthritis__Cancer/Tumor (type) _______________ __ Sleep disorder __Muscle/Joint Disorders__ Mononucleosis __Chemical/Alcohol dependency __ Hearing Loss__ Hay fever/Allergies __Physical/Sexual Abuse __ Visual Problems__Asthma __ Stomach Ulcers/Reflux __Learning Disabilities__Eczema/Psoriasis __ Gallbladder Disorder __ Physical impairments: list below__High Blood Pressure __ Hepatitis _______________________Heart Condition/Murmur __ Colon disorder (Crohn’s, Ulcerative Colitis, __Tuberculosis/Positive Skin Test__Thyroid Disorder Irritable Bowel) __ Malaria__Diabetes __ Kidney Stones __Other Significant <strong>Health</strong>__High Cholesterol __ Frequent Urinary Tract Infections Problems (list)_______________ Sexually Transmitted Infection_________________________Please explain any positive answers____________________________________________________________________________________________________________________________________________________________________________________________Women’s <strong>Health</strong>:Age at your first menstrual period: _____Number of days your period usually lasts: _____Date of your last Pap smear:_____Abnormal Pap smear ever?____ If so, date:________Number of Pregnancies: _____ Number of children:_____List any hormones or oral contraceptives that you take:______________________________________________________♦ Have you ever had: Breast disorders ___; Ovarian cysts ___; Endometriosis ___; Pelvic infections____<strong>Health</strong> Habits Assessment: Please place a check mark beside any of the following that apply:__Drink alcohol – if so, number of drinks per week _______Smoke cigarettes/cigars__Use snuff/chewing tobacco__Use seat belts__Feel unsafe in a current relationship__Exercise regularly (3 – 4 times per week)__Are you sexually activeLearning Needs: Please list any Language Barriers, Learning Disabilities, Physical Disabilities or Cultural/Religious issuesthat may affect <strong>Medical</strong> care. ____________________________________________________________________________________________________________________________________________________________________________________________<strong>Student</strong>’s Signature______________________________________Date:______________If you have a medical problem which might require attention during your period of attendance, it would assist your student healthphysician to have a report from your private physician regarding that condition. Records should be submitted to:<strong>Medical</strong> Records DepartmentUniversity of Tennessee<strong>Student</strong> <strong>Health</strong> <strong>Center</strong>1800 Volunteer BlvdKnoxville, TN 37996-3102*Receipt of this form by the <strong>Student</strong> <strong>Health</strong> Service does not constitute the establishment of a doctor–patient relationship.This is established only after an eligible student is first seen at the <strong>Student</strong> <strong>Health</strong> <strong>Center</strong>.FOR OFFICE USE ONLYReviewed by: __________Date: __________