World Deaf Leadership * Scholarship Program - Gallaudet University
World Deaf Leadership * Scholarship Program - Gallaudet University
World Deaf Leadership * Scholarship Program - Gallaudet University

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
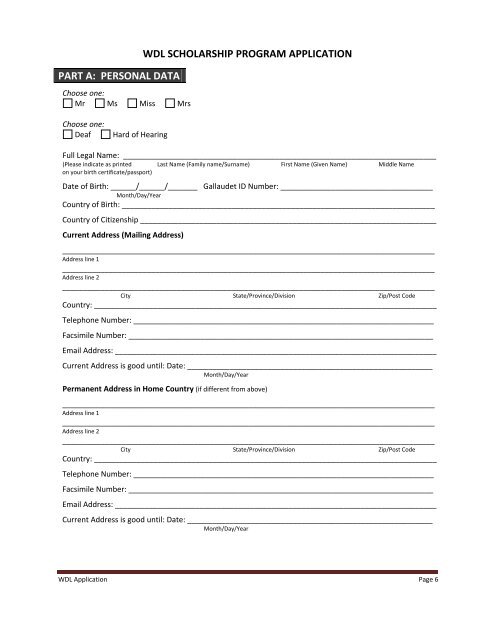
PART A: PERSONAL DATAChoose one:Mr Ms Miss MrsWDL SCHOLARSHIP PROGRAM APPLICATIONChoose one:<strong>Deaf</strong>Hard of HearingFull Legal Name: __________________________________________________________________________(Please indicate as printed Last Name (Family name/Surname) First Name (Given Name) Middle Nameon your birth certificate/passport)Date of Birth: ______/______/_______ <strong>Gallaudet</strong> ID Number: ____________________________________Month/Day/YearCountry of Birth: __________________________________________________________________________Country of Citizenship ______________________________________________________________________Current Address (Mailing Address)________________________________________________________________________________________Address line 1________________________________________________________________________________________Address line 2________________________________________________________________________________________City State/Province/Division Zip/Post CodeCountry: _________________________________________________________________________________Telephone Number: _______________________________________________________________________Facsimile Number: ________________________________________________________________________Email Address: ____________________________________________________________________________Current Address is good until: Date: __________________________________________________________Month/Day/YearPermanent Address in Home Country (if different from above)________________________________________________________________________________________Address line 1________________________________________________________________________________________Address line 2________________________________________________________________________________________City State/Province/Division Zip/Post CodeCountry: _________________________________________________________________________________Telephone Number: _______________________________________________________________________Facsimile Number: ________________________________________________________________________Email Address: ____________________________________________________________________________Current Address is good until: Date: __________________________________________________________Month/Day/YearWDL Application Page 6