NEI Visual Function Questionnaire (VF) version 03 - Vision ...
NEI Visual Function Questionnaire (VF) version 03 - Vision ...
NEI Visual Function Questionnaire (VF) version 03 - Vision ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
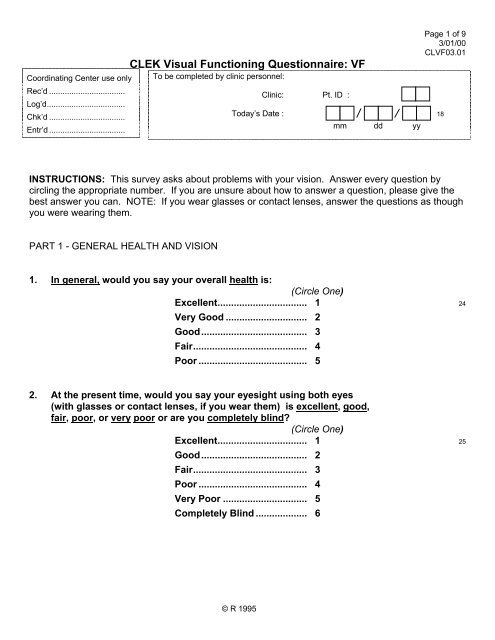
Coordinating Center use onlyRec’d ..................................Log’d...................................Chk’d ..................................Entr’d ..................................*CL<strong>VF</strong>0101*CLEK <strong>Visual</strong> <strong>Function</strong>ing <strong>Questionnaire</strong>: <strong>VF</strong>To be completed by clinic personnel:Clinic: Pt. ID : 9Today’s Date : 18mm dd yyPage 1 of 93/01/00CL<strong>VF</strong><strong>03</strong>.01INSTRUCTIONS: This survey asks about problems with your vision. Answer every question bycircling the appropriate number. If you are unsure about how to answer a question, please give thebest answer you can. NOTE: If you wear glasses or contact lenses, answer the questions as thoughyou were wearing them.PART 1 - GENERAL HEALTH AND VISION1. In general, would you say your overall health is:(Circle One)Excellent................................. 1 24Very Good .............................. 2Good....................................... 3Fair.......................................... 4Poor ........................................ 52. At the present time, would you say your eyesight using both eyes(with glasses or contact lenses, if you wear them) is excellent, good,fair, poor, or very poor or are you completely blind?(Circle One)Excellent................................. 1 25Good....................................... 2Fair.......................................... 3Poor ........................................ 4Very Poor ............................... 5Completely Blind ................... 6© R 1995
*CL<strong>VF</strong>0102*Page 2 of 93/01/00CL<strong>VF</strong><strong>03</strong>.02CLEK <strong>Visual</strong> <strong>Function</strong>ing Questionaire: <strong>VF</strong>Clinic: Pt. ID : 93. How much of the time do you worry about your eyesight?(Circle One)None of the time .................... 1 26A little of the time .................. 2Some of the time ................... 3Most of the time..................... 4All of the time? ...................... 54. How much pain or discomfort have you had in and around your eyes(for example, burning, itching, or aching)? Would you say it is:(Circle One)None ....................................... 1 27Mild ......................................... 2Moderate ................................ 3Severe, or............................... 4Very severe? .......................... 5PART 2 - DIFFICULTY WITH ACTIVITIESThe next questions are about how much difficulty, if any, you have doing certain activitieswearing your glasses or contact lenses if you use them for that activity.5. How much difficulty do you have reading ordinary print innewspapers? Would you say you have:(Circle One)No difficulty at all................................................... 1 28A little difficulty...................................................... 2Moderate difficulty................................................. 3Extreme difficulty .................................................. 4Stopped doing this because of your eyesight .... 5Stopped doing this for other reasons or notinterested in doing this ...................................... 6© R 1995
*CL<strong>VF</strong>01<strong>03</strong>*Page 3 of 93/01/00CL<strong>VF</strong><strong>03</strong>.<strong>03</strong>CLEK <strong>Visual</strong> <strong>Function</strong>ing Questionaire: <strong>VF</strong>Clinic: Pt. ID : 96. How much difficulty do you have doing work or hobbies that require you to see well upclose, such as cooking, sewing, fixing things around the house, or using hand tools?Would you say:(Circle One)No difficulty at all................................................... 1 29A little difficulty...................................................... 2Moderate difficulty................................................. 3Extreme difficulty .................................................. 4Stopped doing this because of your eyesight .... 5Stopped doing this for other reasons or notinterested in doing this ...................................... 67. Because of your eyesight, how much difficulty do you have finding something on acrowded shelf?(Circle One)No difficulty at all................................................... 1 30A little difficulty...................................................... 2Moderate difficulty................................................. 3Extreme difficulty .................................................. 4Stopped doing this because of your eyesight .... 5Stopped doing this for other reasons or notinterested in doing this ...................................... 68. How much difficulty do you have reading street signs or the names of stores?(Circle One)No difficulty at all................................................... 1 31A little difficulty...................................................... 2Moderate difficulty................................................. 3Extreme difficulty .................................................. 4Stopped doing this because of your eyesight .... 5Stopped doing this for other reasons or notinterested in doing this ...................................... 6© R 1995
*CL<strong>VF</strong>0106*Page 6 of 93/01/00CL<strong>VF</strong><strong>03</strong>.06CLEK <strong>Visual</strong> <strong>Function</strong>ing Questionaire: <strong>VF</strong>Clinic: Pt. ID : 915. Are you currently driving, at least once in a while?(Circle One)Yes ..................... 1 Skip To Q 15c 38No....................... 215a. IF NO: Have you never driven a car or have you given up driving?(Circle One)Never drove....... 1 Skip To Part 3, Q 17 39Gave up ............. 215b. IF YOU GAVE UP DRIVING: Was that mainly because of your eyesight,mainly for some other reason, or because of both your eyesight and otherreasons?(Circle One)Mainly eyesight ................................. 1 Skip To Part 3, Q 17 40Mainly other reasons........................ 2 Skip To Part 3, Q 17Both eyesight and other reasons .... 3 Skip To Part 3, Q 1715c. IF CURRENTLY DRIVING: How much difficulty do you have driving during thedaytime in familiar places? Would you say you have:(Circle One)No difficulty at all.............................. 1 41A little difficulty................................. 2Moderate difficulty............................ 3Extreme difficulty.............................. 4© R 1995
*CL<strong>VF</strong>0107*Page 7 of 93/01/00CL<strong>VF</strong><strong>03</strong>.07CLEK <strong>Visual</strong> <strong>Function</strong>ing Questionaire: <strong>VF</strong>Clinic: Pt. ID : 916. How much difficulty do you have driving at night? Would you say you have:(Circle One)No difficulty at all .................................. 1 42A little difficulty ..................................... 2Moderate difficulty ................................ 3Extreme difficulty .................................. 4Have you stopped doing this becauseof your eyesight................................ 5Have you stopped doing this for otherreasons or are you not interested indoing this .......................................... 616a. How much difficulty do you have driving in difficult conditions,such as in bad weather, during rush hour, on the freeway, or in city traffic?Would you say you have: (Circle One)(Circle One)No difficulty at all .................................. 1 43A little difficulty ..................................... 2Moderate difficulty ................................ 3Extreme difficulty .................................. 4Have you stopped doing this becauseof your eyesight................................ 5Have you stopped doing this for otherreasons or are you not interested indoing this .......................................... 6© R 1995
*CL<strong>VF</strong>0109*Page 9 of 93/01/00CL<strong>VF</strong><strong>03</strong>.09CLEK <strong>Visual</strong> <strong>Function</strong>ing Questionaire: <strong>VF</strong>Clinic: Pt. ID : 9For each of the following statements, please circle the number to indicate whether for you thestatement is definitely true, mostly true, mostly false, or definitely false for you or you are notsure.(Circle One On Each Line)Definitely Mostly Not Mostly DefinitelyTrue True Sure False False20. I stay home most of the timebecause of my eyesight..... 1 2 3 4 5 4721. I feel frustrated a lot of thetime because of myeyesight. ............................. 1 2 3 4 5 4822. I have much less controlover what I do, because ofmy eyesight. ....................... 1 2 3 4 5 4923. Because of my eyesight, Ihave to rely too much onwhat other people tell me.. 1 2 3 4 5 5024. I need a lot of help fromothers because of myeyesight. ............................. 1 2 3 4 5 5125. I worry about doing thingsthat will embarrass myselfor others, because of myeyesight. ............................. 1 2 3 4 5 52END 01© R 1995