claim on esb medical benefits scheme - ESB Retired Staff Homepage
claim on esb medical benefits scheme - ESB Retired Staff Homepage
claim on esb medical benefits scheme - ESB Retired Staff Homepage
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
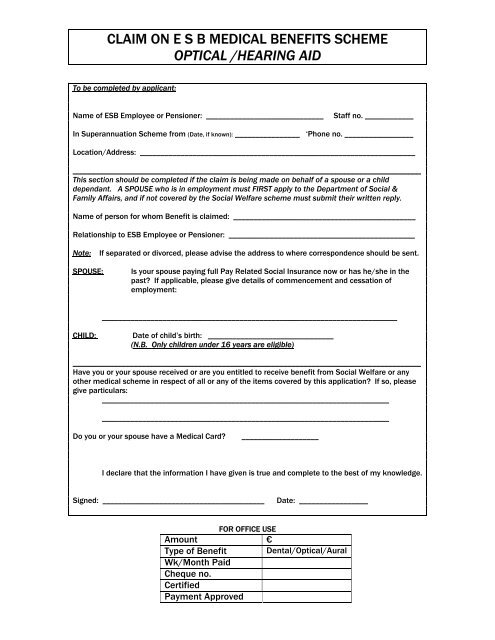
CLAIM ON E S B MEDICAL BENEFITS SCHEMEOPTICAL /HEARING AIDTo be completed by applicant:Name of <strong>ESB</strong> Employee or Pensi<strong>on</strong>er: _____________________________<strong>Staff</strong> no. ____________In Superannuati<strong>on</strong> Scheme from (Date, if known): ________________ ‘Ph<strong>on</strong>e no. _________________Locati<strong>on</strong>/Address: __________________________________________________________________________________________________________________________________________________________This secti<strong>on</strong> should be completed if the <str<strong>on</strong>g>claim</str<strong>on</strong>g> is being made <strong>on</strong> behalf of a spouse or a childdependant. A SPOUSE who is in employment must FIRST apply to the Department of Social &Family Affairs, and if not covered by the Social Welfare <strong>scheme</strong> must submit their written reply.Name of pers<strong>on</strong> for whom Benefit is <str<strong>on</strong>g>claim</str<strong>on</strong>g>ed: _____________________________________________Relati<strong>on</strong>ship to <strong>ESB</strong> Employee or Pensi<strong>on</strong>er: ______________________________________________Note:If separated or divorced, please advise the address to where corresp<strong>on</strong>dence should be sent.SPOUSE:Is your spouse paying full Pay Related Social Insurance now or has he/she in thepast? If applicable, please give details of commencement and cessati<strong>on</strong> ofemployment:_________________________________________________________________________CHILD:Date of child’s birth: _______________________________(N.B. Only children under 16 years are eligible)______________________________________________________________________________________Have you or your spouse received or are you entitled to receive benefit from Social Welfare or anyother <strong>medical</strong> <strong>scheme</strong> in respect of all or any of the items covered by this applicati<strong>on</strong>? If so, pleasegive particulars:______________________________________________________________________________________________________________________________________________Do you or your spouse have a Medical Card?___________________I declare that the informati<strong>on</strong> I have given is true and complete to the best of my knowledge.Signed: ________________________________________Date: _________________FOR OFFICE USEAmount €Type of Benefit Dental/Optical/AuralWk/M<strong>on</strong>th PaidCheque no.CertifiedPayment Approved
This <str<strong>on</strong>g>claim</str<strong>on</strong>g> form should be completed and returned to the appropriate paying office* together withwhichever of the following documents are relevant:Optical Benefit:Hearing Aid:Itemised receipt indicating the services providedOrThe Optician should complete, sign and stamp this side ofthe formReceipt and certificate from Doctorrecommending the purchase of Hearing Aid(s)* For current employees/staff <strong>on</strong> VSS<strong>Staff</strong> <strong>on</strong> Pensi<strong>on</strong>s Payroll:Payroll UnitE S BKilcruttin Business ParkTullamoreCo OffalyPayrollE S BLower Fitzwilliam StreetDublin 2- envelopes should be marked “Medical Benefits”______________________________________________________________________________________TO BE COMPLETED BY OPTICIANExaminati<strong>on</strong> Date: _________________Sight Examinati<strong>on</strong>:€ ___________________Supply or Repair of Spectacles1 pair Distance € ____________________1 pair Reading € ___________________Bi-focal/Varifocal spectacles or repairs thereto:C<strong>on</strong>tact Lenses:(Once-off payment, unless there is a change in prescripti<strong>on</strong> )€ ___________________€ ____________________Total:€ ____________________P D 1068 (9/05)