Download the Medical Information Release Authorization form
Download the Medical Information Release Authorization form
Download the Medical Information Release Authorization form
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
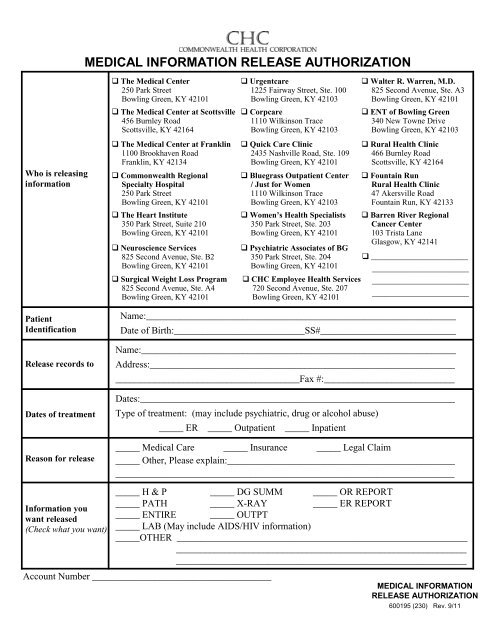
MEDICAL INFORMATION RELEASE AUTHORIZATIONWho is releasingin<strong>form</strong>ation The <strong>Medical</strong> Center250 Park StreetBowling Green, KY 42101 The <strong>Medical</strong> Center at Scottsville456 Burnley RoadScottsville, KY 42164 The <strong>Medical</strong> Center at Franklin1100 Brookhaven RoadFranklin, KY 42134 Commonwealth RegionalSpecialty Hospital250 Park StreetBowling Green, KY 42101 The Heart Institute350 Park Street, Suite 210Bowling Green, KY 42101 Neuroscience Services825 Second Avenue, Ste. B2Bowling Green, KY 42101 Surgical Weight Loss Program825 Second Avenue, Ste. A4Bowling Green, KY 42101 Urgentcare1225 Fairway Street, Ste. 100Bowling Green, KY 42103 Corpcare1110 Wilkinson TraceBowling Green, KY 42103 Quick Care Clinic2435 Nashville Road, Ste. 109Bowling Green, KY 42101 Bluegrass Outpatient Center/ Just for Women1110 Wilkinson TraceBowling Green, KY 42103 Women’s Health Specialists350 Park Street, Ste. 203Bowling Green, KY 42101 Psychiatric Associates of BG350 Park Street, Ste. 204Bowling Green, KY 42101 CHC Employee Health Services720 Second Avenue, Ste. 207Bowling Green, KY 42101 Walter R. Warren, M.D.825 Second Avenue, Ste. A3Bowling Green, KY 42101 ENT of Bowling Green340 New Towne DriveBowling Green, KY 42103 Rural Health Clinic466 Burnley RoadScottsville, KY 42164 Fountain RunRural Health Clinic47 Akersville RoadFountain Run, KY 42133 Barren River RegionalCancer Center103 Trista LaneGlasgow, KY 42141 ________________________________________________________________________________________________PatientIdentification<strong>Release</strong> records toDates of treatmentReason for releaseName:________________________________________________________________Date of Birth:___________________________SS#____________________________Name:_________________________________________________________________Address:_____________________________________________________________________________________________________Fax #:___________________________Dates:_________________________________________________________________Type of treatment: (may include psychiatric, drug or alcohol abuse)_____ ER _____ Outpatient _____ Inpatient_____ <strong>Medical</strong> Care _____ Insurance _____ Legal Claim_____ O<strong>the</strong>r, Please explain:_____________________________________________________________________________________________________________________<strong>In<strong>form</strong>ation</strong> youwant released(Check what you want)_____ H & P_____ PATH_____ ENTIRE_____ DG SUMM_____ X-RAY_____ OR REPORT_____ ER REPORT_____ OUTPT_____ LAB (May include AIDS/HIV in<strong>form</strong>ation)_____OTHER ____________________________________________________________________________________________________________________________________________________________________________________Account Number _____________________________________MEDICAL INFORMATIONRELEASE AUTHORIZATION600195 (230) Rev. 9/11
I understand that this authorization is valid only for a maximum of 90 days from <strong>the</strong> date below, and it coversonly treatment prior to <strong>the</strong> date below.This in<strong>form</strong>ation may be released by facsimile machine if request warrants. Commonwealth HealthCorporation and its subsidiaries are hereby released from any liability and <strong>the</strong> undersigned will holdCommonwealth Health Corporation harmless for complying with this authorization. A photostat copy of thisauthorization is acceptable and will be treated as original.The undersigned acknowledges that <strong>the</strong> provision of free medical records by any healthcare provider whoreceives this release shall fulfill that healthcare provider’s obligation to provide one free copy of <strong>the</strong> medicalrecords, and that any future report request for medical records from <strong>the</strong> healthcare provider may result in acopying fee up to one dollar per page.I understand that <strong>the</strong> in<strong>form</strong>ation in my health record may include in<strong>form</strong>ation relating to sexually transmitteddisease, acquired immunodeficiency syndrome (AIDS), or human immunodeficiency virus (HIV). It may alsoinclude in<strong>form</strong>ation about behavioral or mental health services, and treatment for alcohol and drug abuse.I understand that I have a right to revoke this authorization at anytime. I understand that if I revoke thisauthorization I must do so in writing and present my written revocation to <strong>the</strong> Health <strong>In<strong>form</strong>ation</strong> ManagementDepartment. I understand that <strong>the</strong> revocation will not apply to in<strong>form</strong>ation that has already been released inresponse to this authorization. I understand that <strong>the</strong> revocation will not apply to my insurance company when<strong>the</strong> law provides my insurer with <strong>the</strong> right to contest a claim under my policy.Revocation date__________________ Patient/Legal Representative:______________________________I understand that authorizing <strong>the</strong> disclosure of this health in<strong>form</strong>ation is voluntary. I can refuse to sign thisauthorization. I need not sign this <strong>form</strong> in order to assure treatment. I understand that I may inspect or copy <strong>the</strong>in<strong>form</strong>ation to be used or disclosed, as provided in CFR 164.524. I understand that any disclosure ofin<strong>form</strong>ation comes with it <strong>the</strong> potential for an unauthorized redisclosure and <strong>the</strong> in<strong>form</strong>ation may not beprotected by federal confidentiality rules. If I have questions about disclosure of my health in<strong>form</strong>ation, I cancontact <strong>the</strong> Health <strong>In<strong>form</strong>ation</strong> Management Department.Patient/Legal Representative Signature: ____________________________________ Date:_____________Relationship to patient:__________________________________Please mail <strong>the</strong> completed authorization <strong>form</strong> to:Attn: <strong>Release</strong> of <strong>In<strong>form</strong>ation</strong>Health <strong>In<strong>form</strong>ation</strong> Management DepartmentThe <strong>Medical</strong> Center250 Park StreetBowling Green, KY 42101FOR OFFICE USE ONLY <strong>Release</strong>d by: ____________________________________ # of pages copied: ______________First free copy: Yes No MEDICAL INFORMATIONRELEASE AUTHORIZATIONPage 2 600195 (245) Rev. 9/11