Oral medicine â Update for the dental practitioner - Oral Cancer ...
Oral medicine â Update for the dental practitioner - Oral Cancer ...
Oral medicine â Update for the dental practitioner - Oral Cancer ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
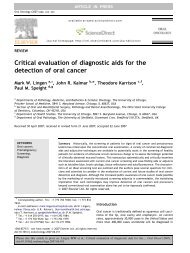
PRACTICECauses of oral ulcerationUlcers and erosions can also be <strong>the</strong> final commonmanifestation of a spectrum of conditions. Theserange from: epi<strong>the</strong>lial damage resulting fromtrauma; an immunological attack as in lichenplanus, pemphigoid or pemphigus; damagebecause of an immune defect as in HIV diseaseand leukaemia; infections such as herpesviruses,tuberculosis and syphilis; cancer and nutritionaldefects such as vitamin deficiencies and somegastrointestinal diseases (Tables 1 and 2).Fig. 6 Minor aphthous ulcerationUlcers of local causesAt any age, <strong>the</strong>re may be burns from chemicalsof various kinds (Fig. 3), heat (Fig. 4), cold, orionising radiation or factitious ulceration, especiallyof <strong>the</strong> maxillary gingivae or palate.Children may develop ulceration of <strong>the</strong> lowerlip by acci<strong>dental</strong> biting following <strong>dental</strong> localanaes<strong>the</strong>sia. Ulceration of <strong>the</strong> upper labialfraenum, especially in a child with bruised andswollen lips, subluxed teeth or fractured jaw canrepresent non-acci<strong>dental</strong> injury. At any age, trauma,hard foods, or appliances may also causeulceration. The lingual fraenum may be traumatisedby repeated rubbing over <strong>the</strong> lower incisorteeth in cunnilingus, in recurrent coughing as inwhooping cough, or in self-mutilating conditions.Most ulcers of local cause have an obviousaetiology, are acute, usually single ulcers, lastless than three weeks and heal spontaneously.Chronic trauma may produce an ulcer with akeratotic margin (Fig. 5).Fig. 5 Traumatic ulceration, lateral tongueRecurrent aphthous stomatitis (RAS; aphthae;canker sores)RAS is a very common condition which typicallystarts in childhood or adolescence and presentswith multiple recurrent small, round or ovoidulcers with circumscribed margins, ery<strong>the</strong>matoushaloes, and yellow or grey floors (Fig. 6).RAS affects at least 20% of <strong>the</strong> population,with <strong>the</strong> highest prevalence in higher socio-economicclasses. Virtually all dentists will seepatients with aphthae.AetiopathogenesisImmune mechanisms appear at play in a personwith a genetic predisposition to oral ulceration. Agenetic predisposition is present, and <strong>the</strong>re is apositive family history in about one third ofpatients with RAS. Immunological factors are alsoinvolved, with T helper cells predominating in <strong>the</strong>RAS lesions early on, along with some naturalkiller (NK) cells. Cytotoxic cells <strong>the</strong>n appear in <strong>the</strong>lesions and <strong>the</strong>re is evidence <strong>for</strong> an antibodydependent cellular cytotoxicity (ADCC) reaction. Itnow seems likely <strong>the</strong>re<strong>for</strong>e that a minor degree ofimmunological dysregulation underlies aphthae.RAS may be a group of disorders of differentpathogeneses. Cross-reacting antigens between<strong>the</strong> oral mucosa and microorganisms may be <strong>the</strong>initiators, but attempts to implicate a variety ofbacteria or viruses have failed.Predisposing factorsMost people who suffer RAS are o<strong>the</strong>rwiseapparently completely well. In a few, predisposingfactors may be identifiable, or suspected.These include:1. Stress: underlies RAS in many cases. RAS aretypically worse at examination times.2. Trauma: biting <strong>the</strong> mucosa, and <strong>dental</strong>appliances may lead to some aphthae.3. Haematinic deficiency (deficiencies of iron,folic acid (folate) or vitamin B 12) in up to 20%of patients.4. Sodium lauryl sulphate (SLS), a detergent insome oral healthcare products may produceoral ulceration.5. Cessation of smoking: may precipitate oraggravate RAS.6. Gastrointestinal disorders particularly coeliacdisease (gluten-sensitive enteropathy) andCrohn’s disease in about 3% of patients.7. Endocrine factors in some women whose RASare clearly related to <strong>the</strong> fall in progestogenlevel in <strong>the</strong> luteal phase of <strong>the</strong>ir menstrual cycle.8. Immune deficiency: ulcers similar to RAS maybe seen in HIV and o<strong>the</strong>r immune defects.9. Food allergies: underlie RAS rarely.Drugs may produce aphthous-like lesions (seebelow).Key points <strong>for</strong> dentists: aphthous ulcers• They are so common that all dentists willsee <strong>the</strong>m• It is important to rule out predisposingcauses (sodium lauryl sulphate, certainfoods/drinks, stopping smoking or vitaminor o<strong>the</strong>r deficiencies) or conditions such asBehcet’s syndrome• Enquire about eye, genital, gastrointestinalor skin lesions• Topical corticosteroids are <strong>the</strong> maintreatmentBRITISH DENTAL JOURNAL VOLUME 199 NO. 5 SEPT 10 2005 261