Pre-Travel Health Questionnaire - Connecticut College
Pre-Travel Health Questionnaire - Connecticut College
Pre-Travel Health Questionnaire - Connecticut College

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
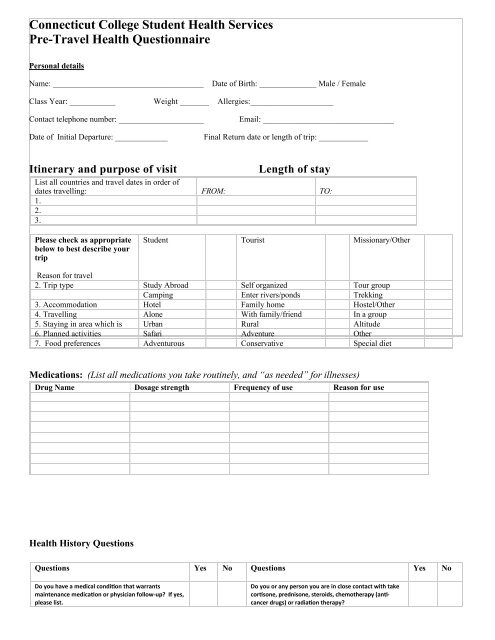
<strong>Connecticut</strong> <strong>College</strong> Student <strong>Health</strong> Services<strong>Pre</strong>-<strong>Travel</strong> <strong>Health</strong> <strong>Questionnaire</strong>Personal detailsName: _____________________________________Date of Birth: ______________ Male / FemaleClass Year: ___________ Weight _______ Allergies:____________________Contact telephone number: _____________________ Email: ________________________________Date of Initial Departure: _____________Final Return date or length of trip: ____________Itinerary and purpose of visitLength of stayList all countries and travel dates in order ofdates travelling: FROM: TO:1.2.3.Please check as appropriatebelow to best describe yourtripStudent Tourist Missionary/OtherReason for travel2. Trip type Study Abroad Self organized Tour groupCamping Enter rivers/ponds Trekking3. Accommodation Hotel Family home Hostel/Other4. <strong>Travel</strong>ling Alone With family/friend In a group5. Staying in area which is Urban Rural Altitude6. Planned activities Safari Adventure Other7. Food preferences Adventurous Conservative Special dietMedications: (List all medications you take routinely, and “as needed” for illnesses)Drug Name Dosage strength Frequency of use Reason for use<strong>Health</strong> History QuestionsQuestions Yes No Questions Yes NoDo you have a medical condi0on that warrantsmaintenance medica0on or physician follow‐up? If yes,please list.Do you or any person you are in close contact with takecor0sone, prednisone, steroids, chemotherapy (an0‐cancer drugs) or radia0on therapy?
Do Influenza you have A heart problems? Do you have a cardiacarrhythmia or irregularity?Do you have high blood pressure?Do you have any bleeding problems; take aspirin, orother blood thinner medica0on?Do you have a history of cloKng disorders? (Stroke,heart aLack, pulmonary embolus, etc)Do you have lung disease, asthma, or shortness ofbreath?Do you have a stomach or bowel condi0on such asbowel irritability, frequent diarrhea or cons0pa0on,heartburn or ulcer?Have you ever been treated for depression, anxiety orother psychiatric illness?Have you ever aLempted suicide or had suicidalthoughts?Do you have diabetes? If so do you take insulin?Have you ever tested posi0ve for tuberculosis?If so, describe your treatment:Do you or any person you are in close contact with havecancer, leukemia, HIV/AIDS, or other auto immunesystem problems?Do you have kidney problems?Do you have a G6PD deficiency?Do you smoke cigareLes? If so, how much?Do you have a history of seizures or Guillian‐BarreSyndrome?Do you have any skin condi0ons such as psoriasis, eczemaor shingles?Have you received any vaccina0ons in the past 4 weeks?Please list:Are you prone to mo0on sickness?Have you ever had a serious reac0on such as hives, rash,wheezing, difficulty breathing, or shock aTer receiving avaccina0on? If so, describe:Have you had any medical problems occur duringprevious travel? If so, describeWOMEN ONLY: Are you pregnant, or planning to getpregnant in the next 3 months?Please share any other per0nent medical informa0onthat may impact your travel:MD/APRN Notes:FOR MD/APRN/RN OFFICIAL USE:DATE: <strong>Travel</strong> risk assessment performed on:<strong>Travel</strong> vaccines recommended for this tripDiseaseprotectionDate of LastDose(s)Recommendedby the CDCTd/DTP/DT(Tetanus/Diptheria)MMRPolioHepatitis AHepatitis BTyphoidInfluenza BRequiredbyCountryPatientdeclinedDosage info: Lot#/Exp. Date/IM-SQ/site