Leading from Preparedness Through Recovery - The 2012 ...
Leading from Preparedness Through Recovery - The 2012 ...
Leading from Preparedness Through Recovery - The 2012 ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Leading</strong> <strong>from</strong> <strong>Preparedness</strong><strong>Through</strong> <strong>Recovery</strong>May 21-25 • Nashville, TN
TRAINING SUMMIT INFORMATIONRegistration Desk HoursLocated in the Delta BCD LobbySunday, May 20.........................................................................1600 – 2000 hrsMonday, May 21.......................................................................0700 – 1730 hrsTuesday, May 22.......................................................................0700 – 1900 hrsWednesday, May 23..................................................................0700 – 1800 hrsThursday, May 24......................................................................0700 – 1730 hrsFriday, May 25...........................................................................0700 – 1200 hrsEvaluation StationsLocation: Delta LobbyEvaluation stations will open Monday, May 21 at 1700 hrs.<strong>The</strong>y will close Friday, May 25 at 1200 hrs.Pre-ordered box lunch pickup(Monday – Wednesday only)Located at Water’s Edge, on the lower level of the DeltaIslands (below STAX’s)1145 – 1230 hrsITS 5K Fun Run/WalkThursday, May 24 0630 – 0800 hrsLocation: Presidential PorticoJoin us Thursday morning for the 2nd AnnualElizabeth Fitch Memorial 5K Fun Run/Walk.This is the perfect way to start day two of the Integrated TrainingSummit. Fresh air, exercise and a chance to relax before starting thedaily sessions. Fun Run/Walk will begin at 0630 hrs on Thursday, May24th. Registration will be open at 0600 hrs and will be located in thePresidential Lobby/Portico.Water AerobicsFriday, May 25 0630 – 0800 hrsLocation: Indoor PoolJoin us on Friday morning for some early exercise in theINDOOR pool at the Gaylord Opryland. An energeticand fun way to start your day!Towels will be provided.A Psychologist EH Environmental Health M Mortician Rx PharmacistC Certified Counselor EP Emergency Physician MA Medical Administrator SW Social WorkerCAMarriage & Family <strong>The</strong>rapists& Licensed Clinical SocialWorkers of CAAccreditation KeyHE Health Educator MD Physician V VeterinarianD Dentist HX Healthcare Executive N Nurse NA No AccreditationE EMT IH Industrial Hygienist R Respiratory <strong>The</strong>rapist
Table of ContentsAmericans with Disabilities Act........................................................................................................................4Integrated Training Summit Partner Descriptions.............................................................................................5Focus Areas......................................................................................................................................................6Late Breakers/Early Risers.................................................................................................................................9Sunday Workshops - Agenda at a Glance......................................................................................................10Monday Workshops - Agenda at a Glance.....................................................................................................10Table of ContentsTuesday Workshops - Agenda at a Glance......................................................................................................11TELL Classes - Agenda at a Glance.................................................................................................................11Medical Reserve Corps (MRC) Workshops - Agenda at a Glance.....................................................................12Wednesday Sessions - Agenda at a Glance.....................................................................................................13Thursday Sessions - Agenda at a Glance........................................................................................................15Friday Sessions - Agenda at a Glance.............................................................................................................17Disaster Medical Information Suite (DMIS) Training - Agenda at a Glance......................................................18Workshop Descriptions..................................................................................................................................20DMIS Training Descriptions............................................................................................................................29Session Descriptions.......................................................................................................................................34MRC Workshop Descriptions..........................................................................................................................59Continuing Education Information.................................................................................................................63Training Summit Goals...................................................................................................................................63Training Summit Objectives............................................................................................................................63Target Audience ............................................................................................................................................63Continuing Education Credits.........................................................................................................................63Report of Training..........................................................................................................................................64Certificate of Attendance...............................................................................................................................64Accreditation Information..............................................................................................................................64AAMA (Medical Administrators).............................................................................................................64AARC (Respiratory <strong>The</strong>rapists)................................................................................................................64AAVSB - Race (Veterinarians) (Veterinary Technicians)............................................................................64ABIH (Industrial Hygienists)....................................................................................................................64ACEP (Emergency Physicians).................................................................................................................64ACHE (Healthcare Executives).................................................................................................................64<strong>2012</strong> Integrated Training Summit 3
Table of ContentsTable of ContentsACPE (Pharmacists).................................................................................................................................64ADA (Dentists) (Dental Hygienists)..........................................................................................................65AMA PRA Category 1 credit TM ................................................................................................................65(Physicians) (Physicians Assistants) (Psychiatrists)ANCC (Nurses) (Nurse Practitioners).......................................................................................................65APA (Psychologists)................................................................................................................................65CECBEMS (EMTs)....................................................................................................................................65CHES (Certified Health Education Specialists)..........................................................................................65MFT & LCSW (Marriage and Family <strong>The</strong>rapists) (Licensed Clinical Social Workers of California)..............65MSM (Morticians)...................................................................................................................................65NASW (Social Workers)..........................................................................................................................66NBCC (Certified Counselors)...................................................................................................................66NEHA (Environmental Health Specialists)................................................................................................66Planning Committee.......................................................................................................................................67Planning Subcommittee.................................................................................................................................68Presenters......................................................................................................................................................69Presenter Disclosures.....................................................................................................................................73Poster Presentations.......................................................................................................................................75Americans with Disabilities Act PolicyChesapeake Health Education Program, Inc. (CHEP.INC.) wishes to ensure no individual with adisability is excluded, denied services, segregated or otherwise treated differently <strong>from</strong> otherindividuals attending this training because of the absence of auxiliary aids and services. If yourequire any special arrangements to attend and fully participate in any educational workshopprovided by CHEP.INC., please notify a member of the CHEP.INC. staff at the Training Summitregistration desk.4<strong>2012</strong> Integrated Training Summit
Integrated Training Summit Partner DescriptionsNational Disaster Medical System (NDMS)<strong>The</strong> National Disaster Medical System is a Federally coordinatedsystem that augments the nation’s medical response capability. <strong>The</strong> overallpurpose of the NDMS is to supplement an integrated national medicalresponse capability for assisting state and local authorities in dealing withthe medical impacts of major peacetime disasters and to provide support tothe military and Department of Veterans Affairs medical systems in caringfor casualties evacuated back to the United States <strong>from</strong> overseas armedconventional conflicts.<strong>The</strong> National Response Framework utilizes the NDMS as part of theDepartment of Health and Human Services, Office of <strong>Preparedness</strong> andResponse, under Emergency Support Function #8 (ESF#8), Health andMedical Services, to support Federal agencies in the management andcoordination of the Federal medical response to major emergencies andFederally declared disasters, including:❖ Natural disasters❖ Major transportation accidents❖ Technological disasters❖ Acts of terrorism including weapons of mass destruction eventsOur VisionTo serve the Federal response by providing disaster medical care to the nation.Our MissionIt is the mission of the National Disaster Medical System to temporarilysupplement Federal, tribal, state, and local capabilities by funding,organizing, training, equipping, deploying, and sustaining a specialized andfocused range of public health and medical capabilities.<strong>The</strong> components of the National Disaster Medical System include thefollowing:❖ Medical response to a disaster area in the form of personnel (teamsand individuals), supplies, and equipment❖ Patient movement <strong>from</strong> a disaster site to unaffected areas of thenation❖ Definitive medical care at participating hospitals in unaffected areasUnited States Public Health Service (USPHS)<strong>The</strong> mission of the U.S. Public Health Service CommissionedCorps is to protect, promote, and advance the health and safety of ournation. As America’s uniformed service of public health professionals, theCommissioned Corps achieves its mission through:❖ Rapid and effective response to public health needs❖ Leadership and excellence in public health practices❖ Advancement of public health scienceAs one of the nation’s seven uniformed services, the Commissioned Corpsfills essential public health leadership and service roles within the Federalgovernment agencies and programs. <strong>The</strong> Corps’ 6,200-plus active-duty officersare full-time, well-trained, highly qualified public health professionals.Commissioned Corps emergency response teams are managed by the Officeof the Surgeon General. <strong>The</strong> multidisciplinary teams are capable of respondingto domestic disasters, emergencies, public health crises, and internationalhumanitarian missions. <strong>The</strong>re are 41 response teams in the CommissionedCorps Readiness and Response System as well as five rosters of multidisciplinaryindividual augmentees. “Projecting and Responding Everyday”Medical Reserve Corps (MRC)<strong>The</strong> Medical Reserve Corps is a national network of local groupsof volunteers committed to improving the health, safety, and resiliencyof their communities. MRC volunteers include medical and public healthprofessionals, as well as others interested in strengthening the public healthinfrastructure and improving the preparedness and response capabilitiesof their local jurisdiction. MRC units identify, screen, train, and organizethe volunteers, utilizing them to support routine public health activities andaugment preparedness and response efforts.<strong>The</strong> Division of the Civilian Volunteer Medical Reserve Corps (DCVMRC)is headquartered in the Office of the Surgeon General. It functions as aclearinghouse for information and guidance to help communities establish,implement, and maintain MRC units nationwide. Office activities includestrategic planning, policy development, program operations, deploymentoperations, communications, stakeholder outreach, and technical assistance.<strong>The</strong>se activities are carried out by DCVMRC staff and the MRC RegionalCoordinators.Emergency System for AdvanceRegistration of Volunteer HealthProfessionals (ESAR-VHP)<strong>The</strong> Emergency System for Advance Registration of Volunteer Health Professionalsprogram is housed in the Office of the Assistant Secretary for <strong>Preparedness</strong> andResponse at the U.S. Department of Health and Human Services. <strong>The</strong> missionof the ESAR-VHP program is to establish a national network of state-basedprograms for managing volunteers at all tiers of response. ESAR-VHP supports62 states and territories in establishing standardized volunteer registrationprograms for disasters and medical and public health emergencies. <strong>The</strong> program,administered on the state level, verifies health professionals’ identification andcredentials so that they can respond more quickly when disaster strikes. Byregistering through ESAR-VHP, volunteers’ identities, licenses, credentials, andhospital privileges are all verified in advance, saving valuable time in emergencysituations. ESAR-VHP has grown to encompass the cumulative registration ofover 188,000 health and non-health professional volunteers across the 62 stateand territorial programs..Chesapeake Health EducationProgram, Inc. (CHEP.INC)<strong>The</strong> Chesapeake Health Education Program is a multifaceted nonprofitcorporation established in 1990. CHEP is recognized as a trusted partnerboth nationally and locally by Federal, state, and local organizations as wellas professional organizations that are involved in providing education andtraining services. CHEP is a recognized provider of professional accreditation,maintains strong partnerships with a variety of community groups, and playsan important role in enhancing the vision and mission of its Federal partnersthrough the provision of continuing education and transitional housing forhomeless veterans. <strong>Through</strong> partnerships with the Federal government and thecommunity, CHEP is able to bridge the gap between available resources andidentified needs. <strong>The</strong> resulting partnerships transcend diminishing resources,changes in technology, and the constantly changing healthcare climate.Partner Descriptions<strong>2012</strong> Integrated Training Summit 5
Focus area DescriptionsFocus Area DescriptionsHealthcare Systems:Healthcare organizations are critical to a community’s responseto disasters and major emergencies. Those organizations,when aligned as healthcare coalitions, have the potential ofeffectively integrating with multiple local, state, tribal, andFederal agencies, creating a powerful, unified system of careand services.<strong>The</strong> Healthcare Systems focus area seeks to provideinformation, techniques, tools, and networking opportunitiesessential to the continuing development of both individualhealthcare organizations and emerging healthcare coalitions.Proposed participants will include hospitals, communityhealth centers, air and ground EMS providers, skilled nursingand other long-term care organizations, physician medicaloffices, state, tribal, and jurisdictional health departments,dialysis and other outpatient service providers, and theirpartner agencies.Leadership:Building community, state, and national resilience requiresstrong leaders to develop preparedness plans and provideguidance to volunteers and other response groups. Leaders inall phases of the disaster life-cycle can benefit <strong>from</strong> developingand improving the process of motivating others to accomplishboth strategic planning and tactical response objectives. <strong>The</strong>success of leadership is measured by those willing to follow.It is never too late to discover the leader in you!Planning & Development: Sessions in this area will highlightprinciples of strategic leadership such as setting goals,developing teams, creating and executing plans, andevaluating outcomes.Tactical: Sessions in this area will focus on the tactical leadershipof “boots on the ground,” including team dynamics, effectiveleadership communication, and ensuring responder wellbeing.6<strong>2012</strong> Integrated Training Summit
Focus area DescriptionsFocus Area DescriptionsPublic Health:<strong>The</strong> broad scope and complicated nature of health threatsafter hazards require an interdisciplinary approach to publichealth. A foundation of “prevention versus reaction” in publichealth methods will increase overall community resilience.Public health response has been ever more prevalent in theaftermath of hazards. From the responder health issues after9/11 and the long-term recovery <strong>from</strong> the gulf oil spill tothe fungal skin infections in Joplin, Missouri, public healthresponse continues long after public interest has waned.Over the course of the <strong>2012</strong> Integrated Training Summit, thepublic health sessions will be built on the foundation of adisaster risk reduction (DRR) framework. Governments andorganizations across the globe, such as the United Nations,utilize this model to reduce the risk of hazards. <strong>The</strong> publichealth sessions will leverage presenters’ experiences and riskreducinglessons through the components of emergencymanagement. Presenters will focus on each phase andincorporate training approaches and materials that enhancethe learning experience.Professionals <strong>from</strong> all disciplines and fields will find the publichealth sessions to be relevant to aspects of their work in local,state, regional, tribal, Federal, and international health-relatedarenas. Each session will generate ideas and take-homelessons for communities of all sizes.Resource Management andPatient Movement:<strong>The</strong> sessions in this focus area will emphasize the importanceof coordination and collaboration among local, state, tribal,territorial, and Federal partners for preparedness, response,and lessons identified. Each session will feature expert facultywho will explain their experiences and facilitate interactionswith the audience in order to provide participants with anunderstanding of planning factors and special considerations,such as crisis standards of care and ethical considerations,across the spectrum of ESF#8 requirements when incident sizeor significance involves all ESF#8 partners at multiple levels.Lessons learned and toolbox development will be explored.Resources: Sessions on this focus area subtopic willassist participants to better understand the challenges ofpreparedness, response, and lessons identified as well asemergency management and ethical considerations whenresources are constrained or unavailable during disasters.Resources include people, equipment, supplies, and IT/communications systems.Patient Movement: Sessions on this focus area subtopic willassist participants with identifying the types of resourcesavailable within each level of response (local/state/tribal/Federal), demonstrating the relationship and effectiveintegration of various ESF#8 response partners to meetresponse requirements, describing the ESF#8 patient andevacuee movement processes and associated challenges,identifying unique characteristics of caring for or movingat-risk and vulnerable populations, identifying challenges topatient and evacuee tracking and information sharing, andunderstanding the processes used to obtain, deploy, andsustain resources.<strong>2012</strong> Integrated Training Summit 7
Focus area DescriptionsFocus Area DescriptionsResponse Integration andOperational Medicine:Disasters can have catastrophic impacts and significantimplications for population health and medical systems.<strong>The</strong> U.S. Department of Health and Human Services (HHS),in collaboration with its planning partners, mobilizes a widerange of response systems to augment local, state, and tribalresources as they strive to serve populations impacted bydisaster. This focus area emphasizes the integration of variousdiverse entities to achieve positive outcomes and address theunique challenges of operational medicine.Response Integration focuses on vertical and horizontalintegration and collaboration of multidisciplinary teams amonglocal, state, tribal, and national governments. Participants willbe provided with a broad overview of response operations,including complex public health, human and veterinarymedical, and mass fatality operations. Individual sessions willprovide timely examples of how these practices are developedand how they have evolved.All sessions will focus on and define mechanisms for buildingoperational partnerships, coupled with cultural competencies,necessary to forge sustainable relationships among operationalpublic health and medical responding agencies and systems.Operational Medicine is defined as the provision of multidisciplinaryhealthcare in resource-challenged environmentswith unique and hazardous conditions. Practicing “goodmedicine in poor conditions” is a major emphasis of thisfocus area since recent events and worldwide attentionhave identified the critical need to have and maintain viableresponse capabilities in austere environments. Sessions in theOperational Medicine focus area range <strong>from</strong> fundamentals ofoperating in austere environments to recommendations andtools for development and implementation of operationalmedicine concepts.Focus Area Descriptions Color Key:Agenda At A Glance is color coded by focus area for your reference.See below for the color assigned to each focus area and refer to pages 13-17 for session information.Healthcare SystemsLeadershipPublic HealthResource Management and Patient MovementResponse Integration and Operational Medicine8<strong>2012</strong> Integrated Training Summit
Late Breakers & Early RisersTuesday, May 22Late BreakerCrisis Standards of Care: A Systems Framework for Catastrophic Disaster Response 1700-1930 hrs Bayou CWednesday, May 23Early RisersOPEO International Response Programs, Opportunities and Challenges 0700-0800 hrs Bayou ABOPEO <strong>Recovery</strong> Coordination, Completing the Disaster Cycle 0700-0800 hrs Bayou CDAmerican Red Cross: Social Media Engagement and the Digi-Doc 0700-0800 hrs Bayou EAmerican Red Cross: Collaborative Service Delivery Models- Functional andAccess Needs Support Integrated Care Teams 0700-0800 hrs Canal CTRAIN (Triaging Resource Allocation for Inpatient Movement);How Lucile Packard Children’s Hospital is Preparing for Evacuation 0700-0800 hrs Canal BLate Breakers & Early RisersThursday, May 24Early RisersIntegration and Execution of the National Veterinary Response 0700-1000 hrs Canal BOPEO International Response Programs, Opportunities and Challenges 0700-0800 hrs Bayou ABOPEO <strong>Recovery</strong> Coordination, Completing the Disaster Cycle 0700-0800 hrs Bayou CDAmerican Red Cross: Social Media Engagement and the Digi-Doc 0700-0800 hrs Bayou EAmerican Red Cross: Collaborative Service Delivery Models- Functional andAccess Needs Support Integrated Care Teams 0700-0800 hrs Canal CThursday, May 24Mid Day DiscussionOn the Frontlines of “All Health” Emergencies 1130-1300 hrs Canal BThursday, May 24Late BreakerChief Veterinary Officer’s Town Meeting and Update on the NVRT Program 1730-1815 hrs Canal BRock and Roll Up Your Sleeve Blood DriveTuesday, May 22nd, 1400-2000 hrsLocation: Delta C<strong>2012</strong> Integrated Training Summit 9
Handy Perforated Daily Agendas - Detach and Take With You!Workshops at-a-galnceSunday, May 20, <strong>2012</strong>monday, May 21, <strong>2012</strong>Agenda At-A-GlanceWorkshop Title Workshop Time Room Accreditation PageRegistration Desk Hours 1600-2000 Delta LobbyContinental Breakfast 0700-0830 Delta LobbyBasic Disaster Life Support (BDLS) a 1200-1900 Governor’s AE E, MD, N 20Certified Healthcare Emergency Professional CredentialPrep Course – EXAM Onlyb 1900-2200 Bayou A NA 20Agenda At-A-GlanceWorkshop Title Workshop Time Room Accreditation PageRegistration Desk Hours 0700-1730 Delta LobbyContinental Breakfast 0700-0830 Delta LobbySuturing i 0730-0930 Bayou D E, N 23Advanced Disaster Life Support (ADLS) C 0800-1700 Governor’s AE E, MD, N 21Navigation Skills for Disaster Response d 0800-1200 Bayou E C, CA, D, E, EH, EP, HE, HX,IH, M, MA, MD, N, R, SW, V21Practical Application of the Hospital HVA and Its Incorporationinto the Emergency Management Programe 0800-1200 Canal B E, EH, EP, HE, HX, IH, MA,MD, N, RCertified Healthcare Emergency Professional (CHEP) f 0800-1700 Bayou A D, E, EH, EP, HE, HX, IH,MA, MD, N, R2222Simulation Training for Disaster Response in AustereEnvironments: Fostering TeamworkWhere <strong>The</strong>y Are @: Utilizing Social Networking toCommunicate Prevention, <strong>Preparedness</strong>, Response,and <strong>Recovery</strong> Informationg 0800-1200 Ryman Hall C2 D, E, EP, HE, HX, MA, MD,N, Rm 0800-1200 Bayou B C, CA, D, E, EH, EP, HE, HX,IH, M, MA, MD, N, SW, VMass Casualty Incident Management x 0800-1700 Governor’s B D, EP, HE, HX, MA, MD, N 25MedMap Discussion o 0900-1100 Bayou C C, CA, D, E, EH, EP, HE, HX,IH, M, MA, MD, N, SW, VBreak 1000-1030 Multiple LocationsSuturing j 1000-1200 Bayou D E, N 23Lunch (on own) 1145-1300Using HSEEP Tools to Develop Effective Hospital Exercises h 1300-1700 Bayou B E, EH, EP, HE, HX, IH, MA,MD, N, RSuturing k 1300-1500 Bayou D E, N 24Disaster Response: Are You Ready for the Kids? A Refresheron Basic Pediatric MCI Triage and Caren 1300-1700 Delta D D, E, EP, HE, MD, N, R, Rx 24MedMap p 1300-1500 Bayou C NA 24Break 1430-1500 Multiple LocationsSuturing l 1530-1730 Bayou D E, N 242224242310<strong>2012</strong> Integrated Training Summit
Handy Perforated Daily Agendas - Detach and Take With You!tuesday, May 22, <strong>2012</strong>Agenda At-A-GlanceWorkshop Title Workshop Time Room Accreditation PageRegistration Desk Hours 0700-1900 Delta LobbyContinental Breakfast 0700-0830 Delta LobbyAdvanced Disaster Life Support (ADLS) C 0800-1700 Governor’s AE E, MD, N 21Certified Healthcare Emergency Professional (CHEP) f 0800-1700 Bayou A D, E, EH, EP, HE, HX, IH,MA, MD, N, REmergency Management Programs for HealthcareSystems: Program Developmentq 0800-1200 Bayou E EP, HE, HX, MA, MD, N,R, RxAdvanced Airway Management in Austere Conditions s 0800-1200 Canal B E, EP, HE, MD, N, R 27Using HSEEP Tools to Develop Effective Hospital Exercises t 0800-1200 Bayou B E, EH, EP, HE, HX, IH, MA,MD, N, R, Rx222627Workshops at-a-galncePsychological First Aid (PFA) u 0800-1200 Bayou C D, E, EH, EP, HE, HX, IH, M,MA, MD, N, R, Rx, V27Medical Skills in the Disaster Setting w 0800-1700 Governor’s C E, MD, N, R 28Mass Casualty Incident Management x 0800-1700 Governor’s B D, EP, HE, HX, MA, MD, N 25Break 1000-1030 Multiple LocationsLunch (on own) 1145-1300Emergency Management Programs for Healthcare System:Program Evaluationr 1300-1700 Bayou E EP, HE, HX, MA, MD, N,R, Rx26Practical Medication Management in Disasters v 1300-1700 Canal B E, EP, MD, N, Rx 28Break 1430-1500 Multiple LocationsTELL Classes At-A-GlanceWorkshop Title Room Day TimeICS 300 – Intermediate ICSThis training will be conducted over three days.Attendance at all sessions is required.Ryman Studio PQRWednesdayThursdayFriday1300-1700 hrs0800-1700 hrs0800-1200 hrsICS 400 – Advanced ICSThis training will be conducted over three days.Attendance at all sessions is required.Ryman Studio HIWednesdayThursdayFriday1300-1700 hrs0800-1700 hrs0800-1200 hrsE-956; All-Hazards Position-Specific:Liaison Officer (LOFR) CourseThis training will be conducted over three days.Attendance at all sessions is required.Governor’s Chamber ETuesdayWednesdayThursday0800-1700 hrs0800-1700 hrs0800-1200 hrsE-960; All-Hazards Position-Specific:Division/Group Supervisor (DIVS) CourseThis training will be conducted over three days.Attendance at all sessions is required.Governor’s Chamber DMondayTuesdayWednesday0800-1700 hrs0800-1700 hrs0800-1700 hrs<strong>2012</strong> Integrated Training Summit 11
Handy Perforated Daily Agendas - Detach and Take With You!tuesday, May 22, <strong>2012</strong>MRC Agenda At-A-GlanceWorkshop Title Time Room PageUnit Activity Reporting 0800-0900 Ryman Studio JK 59MRC at-a-galnceNew Leader Workshop 0800-1200 Ryman Studio PQR 59MRC-TRAIN: <strong>The</strong> Basics 0800-1200 Ryman Studio L 59MRC Seasoned Leader Workshop 0800-1200 Ryman Ballroom EF 59Strategic Road-Mapping: Planning for Success 0800-1200 Ryman Studio MNO 59Volunteer Management: Leadership 0800-1000 Ryman Studio FG 60Getting the Word Out: An MRC Messaging Workshop 0800-1000 Ryman Studio E 60Overview of Disaster Risk Reduction 0800-1700 Ryman Studio ABC 60Elements of Sustainability for Grassroots Organizations 0800-1000 Ryman Studio HI 60Unit Leader Transition Planning 0900-1000 Ryman Studio JK 61Diversity of Funding 1000-1100 Ryman Studio HI 61Volunteer Management: Recruitment and Retention 1000-1200 Ryman Studio FG 61MRC-TRAIN: Create Training Plans 1000-1200 Ryman Studio JK 61Cultural Efficacy: Putting Cultural Competency to Work in the MRC 1000-1200 Ryman Studio E 61Proposal Development (Awards and Funding) 1100-1200 Ryman Studio HI 62Unit Activity Reporting 1300-1400 Ryman Studio JK 59New Leader Workshop 1300-1700 Ryman Studio PQR 59MRC-TRAIN: <strong>The</strong> Basics 1300-1700 Ryman Studio L 59MRC Seasoned Leader Workshop 1300-1700 Ryman Ballroom EF 59Volunteer Management: Leadership 1300-1500 Ryman Studio FG 60Elements of Sustainability for Grassroots Organizations 1300-1500 Ryman Studio HI 60Getting the Word Out: An MRC Messaging Workshop 1300-1500 Ryman Studio E 60Growing Leaders <strong>from</strong> Within 1300-1700 Ryman Studio MNO 62Unit Leader Transition Planning 1400-1500 Ryman Studio JK 61Diversity of Funding 1500-1600 Ryman Studio HI 61Volunteer Management: Recruitment and Retention 1500-1700 Ryman Studio FG 61MRC-TRAIN: Create Training Plans 1500-1700 Ryman Studio JK 61Proposal Development (Awards and Funding) 1600-1700 Ryman Studio HI 62Volunteer Management: Recruitment and Retention 1500-1700 Ryman Studio E 6112<strong>2012</strong> Integrated Training Summit
Handy Perforated Daily Agendas - Detach and Take With You!Wednesday, May 23, <strong>2012</strong>Focus AreaSub Focus AreaGeneral SessionSession Title Time Room AccreditationRegistration Desk Hours 0700-1800 Delta LobbyContinental Breakfast 0700-0830 Delta LobbySession 01: Opening Ceremony 0830-0900 Delta A Ballroom 34Session 02: <strong>Preparedness</strong> and Professionalism in PublicHealth and Disaster Management: Historical ReflectionsPage0900-1000 Delta A Ballroom 34Break 1000-1030 Multiple LocationsAgenda At-A-GlanceMeet the Author – Poster Presentations 1000-1030 Delta Lobby andGovernor’s LobbySessions at-a-galnceHealthcare SystemsPlanning & DevelopmentSession 03: Integrating Resilience into DisasterMedical Care1030-1145 Bayou CD C, CA, E, EP,HE, HX, IH,MA, MD, N,Rx, SW34Healthcare SystemsOperations ExcellenceSession 04: Palliative Care Considerations inDisaster Situations1030-1145 Bayou E A, C, CA, D,E, EP, HE, HX,MA, MD, N,Rx, SW34LeadershipPlanning & DevelopmentSession 05: Passing the Torch: Succession PlanningDone Right?1030-1145 Delta C C, CA, D, E,EH, EP, HE, HX,IH, M, MA,MD, N, SW, V35leadershipTacticalSession 06: Chaplaincy Support for DisasterDeployment Responses1030-1145 Delta D C, CA, E, EP,HE, HX, M,MA, MD, N,SW35Public HealthIntermediateSession 07: DRAT! (Disaster Readiness Actions forTeens) and North Minneapolis Tornado <strong>Recovery</strong>1030-1145 Governor’s AE A, C, CA, E,EP, HE, HX,M, MA, MD,N, SW36Public HealthAdvancedSession 08: Medication Needs of Survivors with ChronicConditions to Prevent Deterioration during Sheltering1030-1145 Bayou AB C, CA, D, E,EP, HE, HX,MA, MD, N,Rx, SW36Resource Management &Patient MovementResourcesSession 09: Triage in the Field: Taking It to theNext Level1030-1145 Governor’s C E, EP, HE, HX,MA, MD, N,R, Rx37Resource Management &Patient MovementPatient MovementSession 10: ESF#8 Patient Tracking Force Multiplier 1030-1145 Governor’s D C, CA, D, E,EP, HE, HX,IH, MA, MD,N, SW37Response Integration/Operational MedicineResponse IntegrationSession 11: Zombie Emergency: All-Hazards Emergency<strong>Preparedness</strong> Instruction1030-1145 Delta B C, CA, D, E,EP, HE, HX, IH,MA, MD, N,Rx, SW38Response Integration/Operational MedicineOperational MedicineSession 12: Operational Medicine: Past, Present,and Future1030-1145 Governor’s B E, EP, MD,N, Rx38Lunch (on own) 1145-1315Healthcare SystemsPlanning & DevelopmentSession 13: Advancements in HPP Regional HealthcareCoalitions: Utah’s Experiences1315-1430 Bayou CD E, EP, HE, HX,MA, MD, N39<strong>2012</strong> Integrated Training Summit 13
Handy Perforated Daily Agendas - Detach and Take With You!Sessions at-a-galnceWednesday, May 23, <strong>2012</strong>Focus AreaSub Focus AreaHealthcare SystemsOperations ExcellenceLeadershipPlanning & DevelopmentLeadershipTacticalAgenda At-A-GlanceSession Title Time Room AccreditationSession 14: Emergency Planning for Safe andAppropriate Management of Behavioral Health Patientsduring DisastersSession 15: Engaging Youth: A Key Component ofSuccession PlanningSession 16: <strong>The</strong> New Normal? Managing the Rise ofIncivility in Today’s Deployment1315-1430 Bayou E E, EP, HE, HX,MA, MD, N1315-1430 Delta C C, CA, D, E,EH, EP, HE, HX,IH, M, MA, MD,N, SW, V1315-1430 Delta D C, CA, D, E,EH, EP, HE, HX,IH, M, MA, MD,N, SW, VPage394040Public HealthIntermediateSession 17: 36-Hour Exercise, Ventura’s Story: OperationMedical Shelter 20111315-1430 Governor’s AE C, CA, D, E,EH, EP, HE, HX,IH, MA, MD, N,Rx, SW, V40Public HealthAdvancedSession 18: Heat Emergency Response Plans andImplementation1315-1430 Bayou AB C, CA, D, E,EH, EP, HE, HX,IH, MA, MD, N,Rx, SW41Resource Management &Patient MovementResourcesSession 19: Veterinary Resources: First Aid for Non-Vetsand Disaster Animal Health1315-1430 Governor’s C D, E, EH, EP,HE, HX, MA,MD, N, V41Resource Management &Patient MovementPatient MovementSession 20: Hurricanes, Earthquakes, and Patients...OH MY! A Peek behind the USTRANSCOM Curtain1315-1430 Governor’s D C, CA, E, EP,HE, HX, MA,MD, N, SW42Response Integration/Operational MedicineResponse IntergrationSession 21: A Military and Public Health Joint TrainingModel That Cares1315-1430 Delta B D, E, EP, HE,HX, MA,MD, N42Response Integration/Operational MedicineOperational MedicineSession 22: <strong>The</strong> HHS Disaster Behavioral Health CONOPS:Optimizing Public Health and Medical Response and<strong>Recovery</strong> for Survivors and Responders1315-1430 Governor’s B C, CA, E, EP,HE, HX, MA,MD, N, SW43Break 1430-1500 Multiple LocationsJoint Session Session 23: Responder Risk in Crisis Standards of Care 1515-1645 Delta B C, CA, D, E,EH, EP, HE,HX, IH, M, MA,MD, N, R, Rx,SW, V43Joint SessionSession 24: Developing Guidance to Support Allocationby HHS of Scarce Federal Resources in Disaster Settings:An Opportunity for Stakeholder Input1515-1645 Delta D A, C, CA, E, EP,HE, HX, MA,MD, N, SW44Joint SessionSession 25: Implications of New InternationalAgreements on Public Health <strong>Preparedness</strong> andResponse1515-1645 Delta C C, CA, D, E,EH, EP, HE, HX,IH, M, MA, MD,N, SW, V4414<strong>2012</strong> Integrated Training Summit
Handy Perforated Daily Agendas - Detach and Take With You!thursday, May 24, <strong>2012</strong>Focus AreaSub Focus AreaGeneral SessionSession Title Time Room Accreditation Page5K Fun Run/Walk 0630-0800 PresidentialPorticoRegistration Desk Hours 0700-1730 Delta LobbyContinental Breakfast 0700-0830 Delta LobbySession 26: Ethics of Altered Standards of Care in aDisaster Response0830-0945 Delta A Ballroom D, E, EP, EH, HE, HX,IH, MA, MD, N, R, RxBreak 0945-1015 Multiple LocationsMeet the Author – Poster Presentations 0945-1015 Delta Lobby andGovernor’s LobbyAgenda At-A-Glance45Sessions at-a-galnceHealthcare SystemsPlanning & DevelopmentSession 27: Successful Strategies in VolunteerIntegration1015-1130 Bayou CD C, CA, D, E, EH, EP,HE, HX, IH, MA, MD,N, R, SW, V45Healthcare SystemsOperations ExcellenceSession 28: Veterans Health Administration Officeof Emergency Management (VHAOEM) PerformanceImprovement Management System1015-1130 Bayou E C, CA, E, EP, HE,HX, IH, MA, MD, N,Rx, SW45LeadershipPlanning & DevelopmentSession 29: Likability and Leadership 1015-1130 Delta C C, CA, D, E, EP, HE,HX, MA, MD, N,SW, V46LeadershipTacticalSession 30: Listen, Protect, Connect 1015-1130 Delta D C, CA, D, E, EP, HE,HX, MA, MD, N,SW, V46Public HealthIntermediateSession 31: Animals and Nuclear Accidents:Lessons Learned <strong>from</strong> Japan1015-1130 Governor’s AE EH, IH, V 46Public HealthAdvancedSession 32: Cultural Components of Response 1015-1130 Bayou AB A, C, CA, D, E, EP,HE, HX, MA, MD,N, SW47Resource Managementand Patient MovementResourcesSession 33: Leveraging Health Information Exchangefor Disaster <strong>Preparedness</strong> and Response toImprove Patient Care1015-1130 Governor’s C C, CA, D, E, EP, HE,HX, MA, MD, N, SW47Resource Managementand Patient MovementPatient MovementSession 34: Triage, Evaluation, and Care of SpecialNeeds/Vulnerable Populations: Putting It All Together1015-1130 Governor’s D C, CA, D, E, EP, HE,HX, MA, MD, N,R, SW48Response Integration/Operational MedicineResponse IntegrationSession 35: Health System Response to RapidRestoration of Medical Services after the JoplinTornado1015-1130 Delta B E, EP, HE, HX, MA,MD, N, R, Rx48Response Integration/Operational MedicineOperational MedicineHealthcare SystemsPlanning & DevelopmentSession 36: Workforce Health Protection 1015-1130 Governor’s B C, CA, D, E, EH, EP,HE, HX, IH, M, MA,MD, N, R, SW, VLunch (on own) 1130-1300Session 37: In the Line of Fire: How to Prepare for,Respond to, and Recover <strong>from</strong> a Shooting Incident1300-1415 Bayou CD C, CA, E, EP, HE, HX,MA, MD, N, R, SW4849<strong>2012</strong> Integrated Training Summit 15
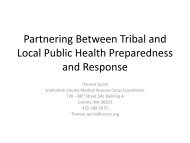
Handy Perforated Daily Agendas - Detach and Take With You!Sessions at-a-galncethursday, May 24, <strong>2012</strong>Focus AreaSub Focus AreaHealthcare SystemsOperations ExcellenceLeadershipPlanning & DevelopmentLeadershipTacticalPublic HealthIntermediatePublic HealthAdvancedSession Title Time Room AccreditationSession 38: Identifying the Factors: Evacuation of theMedically DependentSession 39: A Training Primer: Leaders UsingOrganizational Building Blocks1300-1415 Bayou E C, CA, D, E, EP,HE, HX, MA, MD,N, R, Rx, SW1300-1415 Delta C C, CA, D, E, EH,EP, HE, HX, IH,M, MA, MD, N,SW, VSession 40: Integrating Your Team with <strong>The</strong>ir Team 1300-1415 Delta D A, C, CA, D, E,EH, EP, HE, HX,IH, M, MA, MD,N, SW, VSession 41: Performing a Pediatric Hazard VulnerabilityAnalysis Utilizing a Web-Based Interface: <strong>The</strong> ChicagoExperienceSession 42: Partnering between Tribal and Local PublicHealth <strong>Preparedness</strong> and ResponseAgenda At-A-Glance1300-1415 Governor’s AE E, EP, HE, HX,MA, MD, N, R1300-1415 Bayou AB A, C, CA, D, E,EP, HE, HX,, MA,MD, N, SWPage4950505051Resource Managementand Patient MovementResourcesSession 43: Where the Public Is @: Or How I Learned toStop Worrying and Love Social Media1300-1415 Governor’s C C, CA, D, E, EH,EP, HE, HX, IH,M, MA, MD, N,SW, V51Resource Managementand Patient MovementPatient MovementSession 44: Train as You Respond: Integration of MilitaryFirst Responders and the Forgotten Heroes1300-1415 Governor’s D C, CA, D, E, EH,EP, HE, HX, IH,MA, MD, N, SW52RResponse Integration/Operational MedicineResponse IntegrationSession 45: Mass Fatality Event: Responding to theReno Air Race Tragedy1300-1415 Delta B C, CA, D, E, EH,EP, HE, HX, IH,M, MA, MD,N, SW52Response Integration/Operational MedicineOperational MedicineSession 46: Animal Health Impacts on Human Responseand <strong>Recovery</strong> Efforts1300-1415 Governor’s B C, CA, D, E, EH,EP, HE, HX, IH,M, MA, MD, N,SW, V53Break 1415-1500 Multiple LocationsJoint SessionSession 47: Bioterrorism and the Emerging InfectiousDisease Threat: <strong>Preparedness</strong> and Response Are Critical1500-1630 Delta B C, CA, D, E,EH, EP, HE, HX,IH,MA, MD, N, R,Rx, SW53Joint Session Session 48: When Leadership Goes Askew 1500-1630 Delta C C, CA, D, E, EH,EP, HE, HX, IH,M, MA, MD, N,R, SW, V54Joint SessionSession 49: <strong>The</strong> Regional Sandbox ExperienceREGIONROOMRegion 1Governor’s AERegion 2Governor’s CRegion 3Governor’s BRegion 4Governor’s DRegion 5Delta DRegion 6Bayou ABRegion 7 & 8Bayou DRegion 9Bayou ERegion 10Canal B1500-1700 5416<strong>2012</strong> Integrated Training Summit
Handy Perforated Daily Agendas - Detach and Take With You!Friday, May 25, <strong>2012</strong>Focus AreaSub Focus AreaHealthcare SystemsPlanning & DevelopmentHealthcare SystemsOperations ExcellenceSession Title Time Room AccreditationWater Aerobics 0630-0800 Indoor PoolRegistration Desk Hours 0700-1200 Delta LobbyContinental Breakfast 0700-0830 Delta LobbyAgenda At-A-GlanceSession 50: <strong>The</strong> Joplin Tornado 0830-0945 Bayou CD E, EP, HE, HX, MA,MD, N, RSession 51: What Do You Mean “No Notice”? 0830-0945 Bayou E E, EP, HE, HX, MA,MD, N, RPage5455Sessions at-a-galnceLeadershipPlanning & DevelopmentSession 52: Leadership: When It Counts the Most 0830-0945 Delta C C, CA, D, E, EH, EP,HE, HX, IH, M, MA,MD, N, R, SW, V55LeadershipTacticalSession 53: Emergency Management Dilemma 0830-0945 Delta D C, CA, D, E, EH, EP,HE, HX, IH, M, MA,MD, N, SW, V55Public HealthIntermediateSession 54: Five Feet High and Rising: <strong>The</strong> GaylordOpryland Response to the 2010 Tennessee Flood0830-0945 Governor’s AE C, CA, D, E, EH, EP,HE, HX, IH, M, MA,MD, N, SW, V56Public HealthAdvancedSession 55: U.S. EPA: A National to Local Look atHow Emergency Response and Cleanup ActivitiesAre Conducted0830-0945 Bayou AB C, CA, D, E, EH, EP,HE, HX, IH, M, MA,MD, N, SW56Resource Managementand Patient MovementResourcesSession 56: Working Together! Integration ofVolunteers with ARC, MRC, and ESAR-VHP Partnersduring the Recent Hurricane Responses0830-0945 Governor’s C A, C, CA, D, E, EH,EP, HE, HX, MA,MD, N, SW57Resource Managementand Patient MovementPatient MovementSession 57: “In the Eye of the Storm”: A ProvenSystem of Safe, Integrated, Multiregional PatientEvacuation0830-0945 Governor’s D C, CA, D, E, EH,EP, HE, HX, IH, MA,MD, N, Rx, SW57Response Integration/Operational MedicineResponse IntegrationSession 58: A Comparison of U.S. and CanadianEmergency Support Functions: Public Health,Medical, and Human Services0830-0945 Delta B C, CA, D, E, EH, EP,HE, HX, IH, MA,MD, N, SW57Response Integration/Operational MedicineOperational MedicineSession 59: “Survey Says” . . . ! 0830-0945 Governor’s B E, EP, HE, HX, MA,MD, N58Break 0945-1015 Multiple LocationsGeneral Session Closing Remarks 1015-1045 Delta A Ballroom 58General SessionSession 60: Room for Mistakes: Learning <strong>from</strong>International Disaster Response1045-1215 Delta A Ballroom A, C, CA, D, E, EH,EP, HE, HX, IH,M, MA, MD, N, R,SW, V58<strong>2012</strong> Integrated Training Summit 17
Handy Perforated Daily Agendas - Detach and Take With You!Focus Area DescriptionsTuesday, May 22, <strong>2012</strong>wednesday, May 23, <strong>2012</strong>ZWorkshop Title Time Room Accreditation PageElectronic Medical Record (EMR) Best Practices - Pearls of Wisdom to IncreaseClinical Efficiency1030-1145 Ryman Ballroom F E, EP, N, MD, R 29AA Introduction to Joint Patient Assessment Tracking System (JPATS) 1030-1145 Ryman Studio MNO E, EP, N, MD, R 29BBBasic Information Technology (IT) for Electronic Medical Records (EMR)-Clinical andIT UsersDMIS Agenda At-A-GlanceWorkshop Title Time Room Accreditation PageY DMIS Review and Updates for Instructors - INVITATION ONLY 1700-1930 Ryman Ballroom AB E, EP, N, MD, R 291315-1430 Ryman Ballroom DE E, EP, N, MD, R 30CC Joint Patient Assessment Tracking System (JPATS) Basic Application Training 1315-1430 Ryman Ballroom AB E, EP, N, MD, R 30DD Electronic Medical Record (EMR) Overview 1515-1645 Ryman Ballroom F E, EP, N, MD, R 31Sharing the Disaster Medical Information Suite (DMIS) applications:Question & Answer Session1515-1645 Ryman Studio MNO 32Thursday, May 24, <strong>2012</strong>Workshop Title Time Room Accreditation PageEE Joint Patient Assessment Tracking System (JPATS) Refresher 0800-1000 Ryman Ballroom F E, EP, N, MD, R 31FFElectronic Medical Record (EMR) Best Practices - Pearls of Wisdom to IncreaseClinical Efficiency1030-1145 Ryman Ballroom F E, EP, N, MD, R 31GG Introduction to Joint Patient Assessment Tracking System (JPATS) 1030-1145 Ryman Ballroom C E, EP, N, MD, R 32HHBasic Information Technology (IT) for Electronic Medical Records (EMR)-Clinicaland IT Users1315-1430 Ryman Ballroom DE E, EP, N, MD, R 32II Joint Patient Assessment Tracking System (JPATS) Basic Application Training 1315-1430 Ryman Ballroom AB E, EP, N, MD, R 32JJ Electronic Medical Record (EMR) Overview 1515-1645 Ryman Ballroom F E, EP, N, MD, R 32Sharing the Disaster Medical Information Suite (DMIS) applications: Question &Answer Session1515-1645 Ryman Studio MNO 32friday, May 25, <strong>2012</strong>KKWorkshop Title Time Room Accreditation PageElectronic Medical Record (EMR) Best Practices - Pearls of Wisdom to IncreaseClinical Efficiency0800-0945 Ryman Ballroom C E, EP, N, MD, R 32Disaster Medical Information Suite (DMIS)/Responder E-Learn Cyber CafeRyman Ballroom AB Monday 1200-1600, Tuesday 0800-1700, Wednesday 1030-1145,Thursday 1030-1145, Friday 0800-0945Disaster Medical Information Suite (DMIS) Hands-On LabRyman Ballroom D Monday 1200-1600, Tuesday 0800-1700, Wednesday 1030-1145,Thursday 1030-1145, Friday 0800-094518<strong>2012</strong> Integrated Training Summit
WorkshopDescriptions<strong>2012</strong> Integrated Training Summit 19
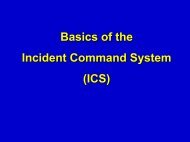
Sunday, May 20, <strong>2012</strong>Workshop DescriptionsWorkshop DescriptionsSunday, May 20, <strong>2012</strong>Workshop A: Basic Disaster Life Support (BDLS)Presenters: Lindsey Anthony, MPA, CEM, EMHP; Philip Coule, MD,FACEP; Archie Hirschmann, AS; Jack Horner, BS; Thomas Lehman;John Ryan; Italo Subbaro, DO, MBA; Ray Swienton, MD, FACEP;Trina von Waldner, PharmDTime: 1200-1900 hrsRoom: Governor’s AEBDLS ® is targeted to multiple disciplines including emergency medicalservice (EMS) personnel, hazardous materials personnel, public healthpersonnel, and healthcare providers. <strong>The</strong> goal of teaching multipledisciplines simultaneously is to develop a commonality of approach andlanguage in the healthcare community, improving the care and coordinationof response in weapons of mass destruction (WMD) disasters and publichealth emergencies. <strong>The</strong> BDLS ® course is a review of the all-hazards topics,including natural and accidental man-made events, traumatic and explosiveevents, nuclear and radiological events, biological events, and chemicalevents. Also included is information on the healthcare professional’s rolein the public health and incident management systems, community mentalhealth, and special needs of underserved and vulnerable populations.<strong>The</strong> recognition and management of the disaster scene and victims arereinforced through a unique approach, introduced in the Core Disaster LifeSupport course, called the DISASTER paradigm. <strong>The</strong> DISASTER paradigmorganizes the students’ preparation and response to disaster management. Itemphasizes an all-hazards approach to mass casualty incident managementand facilitates ongoing qualitative and quantitative assessment of anincident.D – DetectI – Incident CommandS – Scene Security and SafetyA – Assess hazardsS – SupportT – Triage and TreatmentE – EvacuationR – <strong>Recovery</strong><strong>The</strong> mass casualty triage system used in BDLS® and the other NationalDisaster Life Support NDLS courses employs the SALT methodology. ID-me!is a simple mnemonic for sorting patients during triage after a mass casualtyincident (MCI). Detailed discussion and application of these assessmenttools are reinforced throughout the BDLS® and ADLS® courses.S – SortA – AssessL – LifesavingT – Treatment/Transport/TriageI– ImmediateD – DelayedM – MinimalE – ExpectantLearning Objectives:u Identify the critical need to establish healthcare preparedness fordisasters.u Define “all-hazards” and list the possibilities; define “disaster” and“mass casualty incident (MCI).”u Identify the components of the DISASTER paradigm; identify and applythe BDLS triage model using SALT and ID-me!; describe the differencesbetween Basic Disaster Life Support and Advanced Disaster LifeSupport.Intended Audience: EMT/paramedics, nurses, physiciansWorkshop B: Certified Healthcare EmergencyProfessional Credential Prep Course – EXAM OnlyPresenters: Jerry T. Anderson, MS, FAACP, FAAMA, CHEP;Paul V. Richter, MA, FASHE, CHEP, CHSPTime: 1900-2200 hrsRoom: Bayou ASummary: This option is for participants who wish to challenge the CHEPexam without taking the classroom preparation course.<strong>The</strong> International Board for Certification of Safety Managers (IBFCSM)has developed the Certified Healthcare Emergency Professional (CHEP)credential especially for healthcare emergency executives, managers,coordinators and associates. Unlike other healthcare-related certifications,the CHEP is not clinically or first responder oriented – it was designedspecifically for the emergency professional working in a healthcare orpublic health environment. Individuals with the CHEP credential havedemonstrated knowledge of information, standards, and best practices<strong>from</strong> reliable sources: the National Fire Protection Agency (NFPA), <strong>The</strong> JointCommission (TJC), Department of Homeland Security (DHS), OccupationalSafety and Health Administration (OSHA), Federal Emergency ManagementAgency (FEMA), Environmental Protection Agency (EPA), American Societyfor Testing and Materials (ASTM). <strong>The</strong> certification examination also coversareas with which a healthcare emergency manager should be familiar, suchas, Incident Command System (ICS), National Incident Management System(NIMS), Hazard Vulnerability Analysis (HVA), accreditation standards, safety,and the handling of chemicals.20<strong>2012</strong> Integrated Training Summit
Monday, May 21, <strong>2012</strong>Workshop DescriptionsMonday, MAy 21, <strong>2012</strong>Workshop C: Advanced Disaster Life Support (ADLS)Presenters: Lindsey Anthony, MPA, CEM, EMHP; Philip Coule, MD,FACEP; Archie Hirschmann, AS; Jack Horner, BS; Thomas Lehman;John Ryan; Italo Subbaro, DO, MBA; Ray Swienton, MD, FACEP;Trina von Waldner, PharmDTime: 0800-1700 hrs (16-hour workshop, continued Tuesday, May 22,0800-1700 hrs)Room: Governor’s AEADLS ® is an advanced practicum course for the trained BDLS ® provider.It is an intensive, two-day course that allows students to demonstratecompetencies in casualty decontamination, specified essential skills, andmass casualty incident information systems and technology applications.Using simulated, all-hazards scenarios and mass casualty incidents, ADLS ®makes use of four interactive sessions in which participants treat simulatedpatients in various disaster drills and situations. Training is focused on thedevelopment of hands-on skills to allow participants to apply the knowledgelearned in BDLS ® .ADLS ® ’s interactive scenarios and drills utilize high-fidelity mannequins andvolunteer patients to simulate a realistic experience in treating pathologicpatient conditions not routinely encountered by responders and healthcareproviders. Hands-on exercises teach practical skills, such as decontaminationand use of protective equipment, and provide instruction in topics thattraditionally are not addressed in healthcare education curricula.Day 2 of ADLS ® is the hands-on day of training. Four skills stations reinforcethe previous day’s learning. <strong>The</strong>se skills stations are as follows:MASS Triage. This challenging station allows students to practice theconcepts of the disaster paradigm with an emphasis on patient triage.Simulated disaster victims must be triaged and treated correctly whilestudents attempt to manage a chaotic scene and request appropriateresources.Personal Protective Equipment (PPE) and Decontamination. Thisstation teaches important concepts about the use of personal protectiveequipment (PPE) and decontamination technique. Students are given theopportunity to wear PPE and participate in a simulated decontaminationwhile attempting to render medical care.Disaster Skills. This station teaches information about vital skillsnecessary for medical disaster management. Students are taught aboutthe Strategic National Stockpile and proper Mark-I kit use. Students alsopractice smallpox immunization.Human Patient Simulator. Recognition of victims of a chemical andbiological disaster is paramount. This station is designed to reinforcethe detection and proper treatment of conditions that may occur duringdisasters that participants do not normally treat. Treatment of chemical,biological, and traumatic patients is covered. <strong>The</strong> use of high-fidelityhuman patient simulators allows the student to see, hear, and feelinformation that would normally be provided by an instructor, creating amore realistic experience than standard mannequins can provide.Learning Objectives:u Apply the BDLS DISASTER paradigm to respond to various disasterscenarios and treat simulated patients using high-fidelity mannequins.u Apply the BLDS triage model utilizing M.A.S.S. and ID-me!;demonstrate decontamination techniques for disaster scenarios withcontaminated casualties and the correct use of personal protectiveequipment (PPE) for various hazardous scenarios.u Practice the use of autoinjectors for the treatment of chemicalcasualties; practice smallpox immunization with bifurcated needles;obtain information about the Strategic National Stockpile at a DisasterSkills station.Intended Audience: EMT/paramedics, nurses, physiciansWorkshop D: Navigation Skills for Disaster ResponsePresenter: Ben Ho, MDTime: 0800-1200 hrsRoom: Bayou EAll response team members deploying to disasters need to understand thefundamentals of land navigation as well as the newly mandated U.S. NationalGrid System. Whether DMAT, DMORT, NVRT, or USAR, personnel shouldalways know where they are, how to return, how to direct others, and howto identify the location of victims, medical facilities, landing zones, and otherkey landmarks. This concentrated workshop will teach the basics of typicalnavigation skills and tools, map and compass, and new devices and aids.Using actual case histories <strong>from</strong> previous disaster deployments, the coursewill also cover signage, route finding, pattern recognition, and map data,as well as the practical application of these concepts in the altered disasterenvironment. <strong>The</strong> workshop will additionally review the fundamentals ofthe U.S. National Grid System (USNGS). Due to the limitations of class size,indoor conference facilities, and equipment variability and availability, fieldtraining will not be possible. Further practical experience in this perishableskill is highly encouraged for all team members at home.Learning Objectives:u Describe the basics of land navigation.u Apply the basics of land navigation in disasters.u Explain the U.S. National Grid System.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,respiratory therapists, social workers, veterinarians<strong>2012</strong> Integrated Training Summit 21Workshop Descriptions
MoNday, May 21, <strong>2012</strong>Workshop DescriptionsWorkshop DescriptionsWorkshop E: Practical Application of the Hospital HVAand Its Incorporation into the Emergency ManagementProgramPresenters: Ann Potter, RN; Mitch Saruwatari, PhD, MPH, EMTTime: 0800-1200 hrsRoom: Canal BOne of the primary goals of an emergency management program is toreduce organizational risk. This may include promoting the safety of patients,visitors, and staff as well as preventing the disruption of patient care servicesand minimizing resulting damage to the facility. This workshop will providepractical steps and tools for using a hazard vulnerability analysis (HVA) totarget and measure risk reduction through specific quality improvementindicators. Participants will simulate a multidisciplinary hospital safetycommittee. Based on information provided regarding a midsize general acutecare hospital, members will walk through the steps necessary to completean HVA, including interpretation of the results and inclusion of regional andcommunity assessments. Once the HVA is completed, the committee willbe provided with a selection of quality improvement opportunities, such asenhancements to the emergency operations plan, response and functionalannexes, incident management team selection, and general emergencymanagement training. <strong>The</strong> participants will apply the completed HVA tothe development of the annual mitigation, preparedness, and instructionalactivities along with exercise conduct to assess the activities. In addition, thecommittee will prepare an exercise program outline including developingspecific objectives for a functional exercise about a scenario involving asurge of patients entering the facility. At the conclusion of this workshop, thecommittee will host a brief exercise after action review and describe whatis to be included in the improvement plan and ultimately how to reevaluatethe HVA to demonstrate organizational risk reduction. Practical exampleswill be used throughout this session that will be available to participants foradoption or modification in their own facilities.Learning Objectives:u Explain how the hospital HVA is the cornerstone of building acomprehensive emergency management program (EMP).u Identify specific components and steps for incorporating the HVA intothe EMP.u Discuss how to evaluate organization risk reduction through theseactivities.Intended Audience: Emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, industrial hygienists, medical administrators, nurses, physicians,respiratory therapistsWorkshop F: Certified Healthcare EmergencyProfessional (CHEP)Presenters: Jerry Anderson, MS, FAACP, FAAMA, CHEP;Paul Richter, MA, FASHE, CHEP, CHSPTime: 0800-1700 hrs (16-hour workshop,continued Tuesday, May 22, 0800-1700 hrs)Room: Bayou A<strong>The</strong> Certified Healthcare Emergency Professional (CHEP) credential wascreated especially for healthcare emergency executives, managers,coordinators, and associates. Unlike other healthcare certifications, the CHEPis not clinically or first-responder oriented. It was designed specifically forthe emergency professional working in a healthcare setting. Someone witha CHEP credential has demonstrated knowledge of information, standards,and best practices <strong>from</strong> reliable sources: the National Fire ProtectionAssociation (NFPA), Joint Commission, Department of Homeland Security(DHS), Occupational Safety and Health Administration (OSHA), FederalEmergency Management Agency (FEMA), Environmental Protection Agency(EPA), American Society for Testing and Materials (ASTM), and others.<strong>The</strong> certification examination also covers areas with which a healthcareemergency manager should be familiar, such as the Incident CommandSystem, National Incident Management System, hazard vulnerabilityanalysis, accreditation standards, safety, and the handling of chemicals. Thisclass is not for beginning emergency professionals but for individuals whohave in-depth experience through time, knowledge, or both. <strong>The</strong> workshopconsists of one and one-half days of didactic refresher training and thenculminates on the second day with the certification examination.Learning Objectives:u Evaluate the knowledge and capabilities of practitioners engaged inthe administration of healthcare emergency management practice.u Evaluate competence in the use of management, leadership, andsystem principles by healthcare emergency preparedness professionals.u Provide recognition for individual emergency managementprofessionals who meet certification requirements.Intended Audience: Dentists, emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, industrial hygienists, medical administrators, nurses, physicians,respiratory therapistsWorkshop G: Simulation Training for Disaster Responsein Austere Environments: Fostering TeamworkPresenters: Shannon Manzi, PharmD; Angela Schuman, PharmD;Deb Weiner, MD, PhDTime: 0800-1200 hrsRoom: Ryman Hall C2Disaster responders are frequently challenged to provide clinical care in aforeign environment with other providers <strong>from</strong> other disciplines with whomthey rarely work or have never met. This full-scale, high-simulation workshopwill expand on the simulation course taught at the 2011 Integrated TrainingSummit. In addition to using high-fidelity simulation to prepare providersfor their role in disaster response, particularly in austere environments,the goal for the <strong>2012</strong> Integrated Training Summit course will be to fosterdevelopment of teamwork. Simulations will animate real disaster settingsand scenarios. <strong>The</strong> workshop will provide tools to enhance communicationand effective team dynamics between unfamiliar providers and help createa high-functioning, multidisciplinary, cohesive team using principles of crisisresource management. We will provide a low-risk, highly supportive learningenvironment to encourage all providers to participate, regardless of the level22<strong>2012</strong> Integrated Training Summit
MoNday, May 21, <strong>2012</strong>Workshop Descriptionsof experience. An additional goal of the workshop will be to promote the useof simulation as an adjunct for training our disaster responders. <strong>The</strong> workshopwill consist of an interactive didactic session to discuss general principles andpractices of disaster response, addressing different types of responses andthe integration of NDMS teams with other agencies. Respective Concepts ofOperations (CONOPS), provider mixes, and skill sets will be covered, as wellas the types and levels of care that may be required. In the simulation, we willanimate real pediatric and adult patient scenarios, focusing on illness andinjuries commonly seen in disasters and disaster response. At the end of theworkshop, participants will assess their team experience and demonstratethe effective teamwork concepts learned through the simulation experience.<strong>The</strong> participants will be provided with a high-level overview of the resourcesand skills needed to develop and lead simulation sessions and/or courses tohelp prepare providers for disaster response.Workshop DescriptionsLearning Objectives:u Explain the use of high-fidelity simulation to demonstrate generalprinciples and practices of disaster response.u Discuss how to develop teamwork utilizing effective team dynamicsand the concepts and practices of crisis resource management.u Practice providing patient care in scenarios designed to simulate anaustere environment setting.Intended Audience: Dentists, emergency physicians, EMT/paramedics,healthcare executives, health education specialists, medical administrators,nurses, physicians, respiratory therapistsWorkshop H: Using HSEEP Tools to Develop EffectiveHospital ExercisesPresenter: Mary Massey, BSN, MATime: 1300-1700 hrsRoom: Bayou BThis workshop provides participants with the tools and techniques todevelop an effective exercise program consistent with the HomelandSecurity Exercise Evaluation Program (HSEEP). <strong>The</strong> workshop will discusshow to design effective exercises while addressing and coordinatingregulatory, grant, and accreditation requirements. <strong>The</strong> workshop ispresented in a flexible, instructor-led format with hands-on training thatutilizes reference materials and activities-based applications. <strong>The</strong> workshopis customized for healthcare use while maintaining consistency with HSEEPprinciples. <strong>The</strong> workshop guides participants in the customization of partnerorganizations and regional and statewide exercises to meet hospital-specificneeds. Components of the workshop include exercise design, development,conduct, evaluation, and improvement planning. Workshop activities includewriting effective and measurable objectives that test the components of acomprehensive emergency management program, developing a MasterScenario Events List that coordinates with your objectives, and writing anImprovement Plan to facilitate better response capabilities within yourorganization and with other partners.Learning Objectives:u Demonstrate how to develop objectives that are simple, measurable,realistic, and task-oriented.u Demonstrate the process to coordinate healthcare regulatory,accreditation, and grant exercise requirements.u Demonstrate the process to develop an exercise Improvement Plan.Intended Audience: Emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, industrial hygienists, medical administrators, nurses, physicians,respiratory therapistsWorkshop I: SuturingPresenters: Paul Alleyne, MD; Garrick Clouden, MD; Kevin Locke, MDTime: 0730-0930 hrsRoom: Bayou DThis hands-on workshop introduces wound evaluation, cleaning, numbing,and closure techniques to healthcare providers who are inexperienced insuturing. Pig’s feet will be used to practice various suturing techniques.This workshop is designed primarily for the non-physician. This workshopcan be used as part of an ongoing training program to gain wound closureprivileges.Learning Objectives:u Identify lacerations, cuts, and wounds that are amenable to simpleclosure.u Describe proper wound cleaning and preparation for closure.u Explain selection of appropriate suture material.u Describe the indications for the use of simple interrupted, running,and mattress stitches.u Demonstrate the above suturing techniques for skin closure.Intended Audience: EMT/paramedics, nursesWorkshop J: SuturingPresenters: Paul Alleyne, MD; Garrick Clouden, MD; Kevin Locke, MDTime: 1000-1200 hrsRoom: Bayou DIntended Audience: EMT/paramedics, nursesSee above for workshop description and objectives.<strong>2012</strong> Integrated Training Summit 23
MoNday, May 21, <strong>2012</strong>Workshop DescriptionsWorkshop DescriptionsWorkshop K: SuturingPresenters: Paul Alleyne, MD; Garrick Clouden, MD; Kevin Locke, MDTime: 1300-1500 hrsRoom: Bayou DIntended Audience: EMT/paramedics, nursesSee page 23 for workshop description and objectives.Workshop L: SuturingPresenters: Paul Alleyne, MD; Garrick Clouden, MD; Kevin Locke, MDTime: 1530-1730 hrsRoom: Bayou DIntended Audience: EMT/paramedics, nursesSee page 23 for workshop description and objectives.Workshop M: Where <strong>The</strong>y Are @: Utilizing SocialNetworking to Communicate Prevention, <strong>Preparedness</strong>,Response, and <strong>Recovery</strong> InformationPresenters: James Garrow, MPH; Kim Stephens, MPATime: 0800-1200 hrsRoom: Bayou BLearn how Facebook, Twitter, blogs, and RSS feeds can enhance traditionalcrisis communications in every phase of the emergency managementcontinuum—prevention, preparedness, response, and recovery—with aparticular focus on reaching underserved and vulnerable populations. Bestpractice examples will be referenced to provide a framework for discussionon how hospitals and public agencies are currently using social media to theirfullest potential before, during, and after disasters to boost resiliency. Specificconsideration will be given to the following: establishing your agency’s goalsand objectives; policies and issue considerations specific to social mediaand other interactive web-based platforms; resources and training necessaryfor implementation; integrating your social media communications into theJoint Information System as part of Unified Command.Learning Objectives:u Analyze and discuss the benefits and challenges associated withemploying social media technologies in public health and crisiscommunications.u Define ways to utilize social media to reach underserved andvulnerable populations, particularly during the critical prevention andpreparedness phases.u Describe the steps needed to integrate these new communicationtools into current public health emergency managementcommunications plans, policies, and procedures and assess how theyfit into the Joint Information System.Intended Audience: Certified counselors, dentists, emergency physicians,EMT/paramedics, environmental health personnel, healthcare executives,health education specialists, industrial hygienists, marriage & familytherapists, medical administrators, morticians, nurses, physicians, socialworkers, veterinarians24Workshop N: Disaster Response: Are You Ready forthe Kids? A Refresher on Basic Pediatric MCI Triageand CarePresenters: Carolyn Blayney, RN; Mary Alice King, MD, MPH;Kathryn Koelemay, MD, MPH; Vicki Sakata, MD, FACEPTime: 1300-1700 hrsRoom: Delta DIn any disaster situation, the pediatric population will be among the mostvulnerable victims. In most situations they will be cared for not by pediatricspecialists in a pediatric specialty hospital, but by primarily adult trainedmedical personnel. As is demonstrated by population and resource studiesdone in King County, WA and in neighboring Pierce County by the HealthcareCoalition Pediatric Taskforce, the majority of the pediatric populations livewell away <strong>from</strong> pediatric specialty care facilities and closer to communityhospitals, urgent care centers, and private practices. <strong>The</strong>refore, consistentand regular pediatric training is vital to maintaining the necessarymanagement skills and knowledge base. This workshop is primarily directedto non-pediatric care providers and emergency management personnelinterested in developing or refreshing basic pediatric skills and knowledge.<strong>The</strong> workshop will be divided into two sections. <strong>The</strong> first is a brief clinicalreview of basic pediatric triage, assessment, and treatment with emphasison a length-based color coding system and the Pediatric AssessmentTriangle. <strong>The</strong> three main MCI triage protocols (START, JumpSTART, and SALT)will be reviewed but with an eye toward specific pediatric needs. <strong>The</strong> secondhalf is intended to be interactive and provide the audience with practiceusing the previously described techniques and knowledge. Participants willpractice MCI triage and basic pediatric stabilization using both mock patientprofiles and actual patient encounters <strong>from</strong> field experience in Haiti in 2010.Training tools and just-in-time training techniques will be provided so thathospitals, DMAT, EMS, air transport personnel, and MRCs will be ready tomanage pediatric disaster victims.Learning Objectives:u Describe the three basic MCI triage systems and the benefits andpitfalls of each when triaging pediatric patients with informationbased on field experience in Haiti in 2010.u Accurately calculate pediatric dosages, sizes, and initial resuscitationtechniques needed in a disaster and in austere environments.u Review take-home tools, pearls, and just-in-time training resources toimplement in the participant’s home environment.Intended Audience: Dentists, emergency physicians, EMT/paramedics,health education specialists, nurses, pharmacists, physicians, respiratorytherapistsWorkshop O: MedMap DiscussionPresenter: Robert M. Shankman, GISPTime: 0900-1100 hrsRoom: Bayou CMedMap is a secure Geographic Information System (GIS) based, electronic,interactive mapping application. This application incorporates information<strong>from</strong> numerous sources both internal and external to HHS and other Federal<strong>2012</strong> Integrated Training Summit
MoNday, May 21, <strong>2012</strong>Workshop Descriptionsand public agencies into a single visual environment for enhanced situationalawareness, assessment, and management of resources for planning as wellas for response to a natural, man-made, or pandemic event. This systemsupports functions such as policy analysis, planning, course of actioncomparison, incident management, and training. It supports the needs ofdecision makers at various levels of management within HHS and otherFederal agencies to provide enhanced situational awareness at a levelof granularity needed for all responders, including regional emergencycoordinators and teams in the field. It is also able to display and providedetails on medical care sites, resources, and mobilization points and provideanalytical tools for planning and preparedness efforts. During a large eventsuch as an improvised explosive device (IED) or hurricane, there is the needto immediately determine medical care sites, resources, and mobilizationpoints and modify needed data as it becomes available and changes.Rapidly changing conditions and the need for a large regional and nationalresponse require extensive preplanning and a highly flexible system as wellas the ability for data <strong>from</strong> the field to seamlessly get to leadership removed<strong>from</strong> the scene and aid in the planning of the event’s response. MedMap isable to display many different datasets and data feeds, including local datafeeds, to help all involved work with a more complete aggregation of data.With a fully customizable interface, individual users are able to define thedata layers that they need for a specific event or need. Accounts to accessMedMap are created on an individual basis (no group access accounts).External user accounts will become available in the first quarter of 2011.Learning Objectives:u Access the application and utilize the tools within MedMap.u Explain how to add and display data within the interface, while alsobeing able to perform simple spatial analysis.u Demonstrate how to export tables, PDF maps, and JPGs for useoutside of MedMap.Intended Audience: Certified counselors, dentists, emergency physicians,EMT/paramedics, environmental health personnel, healthcare executives,health education specialists, industrial hygienists, marriage & familytherapists, medical administrators, morticians, nurses, physicians, socialworkers, veterinariansWorkshop P: MedMap Hands-OnPresenter: Robert M. Shankman, GISPTime: 1300-1500 hrsRoom: Bayou C<strong>The</strong>re is no fee to attend this two-hour discussion/workshop. Space islimited! This workshop will be a hands-on demonstration of the MedMapand will complement the 0900-1100 hrs discussion. You may register forboth sessions.MedMap is a secure Geographic Information System (GIS) based, electronic,interactive mapping application. This application incorporates information<strong>from</strong> numerous sources both internal and external to HHS and other Federaland public agencies into a single visual environment for enhanced situationalawareness, assessment, and management of resources for planning as wellas for response to a natural, man-made, or pandemic event. This systemsupports functions such as policy analysis, planning, course of actioncomparison, incident management, and training. It supports the needs ofdecision makers at various levels of management within HHS and otherFederal agencies to provide enhanced situational awareness at a levelof granularity needed for all responders, including regional emergencycoordinators and teams in the field. It is also able to display and providedetails on medical care sites, resources, and mobilization points and provideanalytical tools for planning and preparedness efforts. During a large eventsuch as an improvised explosive device (IED) or hurricane, there is the needto immediately determine medical care sites, resources, and mobilizationpoints and modify needed data as it becomes available and changes.Rapidly changing conditions and the need for a large regional and nationalresponse requires extensive preplanning and a highly flexible system as wellas the ability for data <strong>from</strong> the field to seamlessly get to leadership removed<strong>from</strong> the scene and aid in the planning of the event’s response. MedMap isable to display many different datasets and data feeds, including local datafeeds, to help all involved work with a more complete aggregation of data.With a fully customizable interface, individual users are able to define thedata layers that they need for a specific event or need. Accounts to accessMedMap are created on an individual basis (no group access accounts).External user accounts will become available in the first quarter of 2011.Learning Objectives:u Access the application and utilize the tools within MedMap.u Explain how to add and display data within the interface, while alsobeing able to perform simple spatial analysis.u Demonstrate how to export tables, PDF maps, and JPGs for useoutside of MedMap.Workshop X: Mass Casualty Incident ManagementPresenter: A.J. Heightman, MPA, EMT-PTime: 0800-1700 hrs(16 hour course, continues Tuesday, May 22, 0800-1700 hrs)Room: Governor’s BThis workshop is designed for anyone involved in delivering emergencyservices as a result of a mass casualty incident (MCI). A community’s EMS,fire, rescue, police, aeromedical, fire-police, emergency department, anddispatch center personnel should attend since joint response and coordination<strong>2012</strong> Integrated Training Summit 25Workshop Descriptions
Tuesday, May 22, <strong>2012</strong>Workshop DescriptionsWorkshop Descriptionsare crucial to the successful managing of any multiple-victim incident. Thisworkshop offers an equal amount of didactic and practical demonstrationsto the participants, ensuring that the students understand and appreciatethe proper principles and procedures for successful management of masscasualty incidents. Participants will be provided with factual and graphicinformation along with examples of how to manage and/or functioncooperatively at actual, or potential, mass casualty incidents. Participantswill also learn the roles and responsibilities of each key command officerand participating agency at mass casualty incidents. Emphasis will beplaced on procedures and techniques that can be implemented easilyand inexpensively to expedite patient care, identification, removal, anddistribution <strong>from</strong> the scenes encountered.Methods will be presented for:❖ Establishment and identification of incident command❖ Rapid scene assessment, reports, triage, and treatment❖ Use of preplans and checklists to ensure implementation andcompletion of key objectives❖ Staging of emergency vehicles and personnel❖ Use of limited/abbreviated communications and optimal relay ofinformation to:• Incoming and on-scene units and key personnel• Communications centers• Hospital emergency departmentsProblems encountered at actual MCI scenes will be explored, along withsteps that can be taken by individuals and agencies to correct system errorsor deficiencies and improve their overall management of mass casualtyincident scenes.Learning Objectives:u Explain important MCI scene command and control considerations.u Discuss ways to integrate EMS command aspects into the overall ICsystem.u Recite how to prearrange and deploy EMS task forces in the field.u Discuss the importance of reliable communications at an MCI scene.u Describe critical scene safety aspects, security concerns, and hazardcontrol.u Identify the roles and responsibilities of EMS sector officers.Intended Audience: Dentists, emergency physicians, healthcareexecutives, health education specialists, medical administrators, nurses,physicians, pharmacistsTuesday, May 22, <strong>2012</strong>Workshop Q: Emergency Management Programs forHealthcare Systems: Program DevelopmentPresenters: Arnie Bierenbaum, BS, MS; Mike Boucher, BSN, MSN;Pete Brewster, BSTime: 0800-1200 hrsRoom: Bayou E<strong>The</strong> purpose of this workshop is to improve the ability of participants todevelop and maintain comprehensive emergency management programs attheir hospitals. <strong>The</strong> content used in the delivery of this session integrates thevarious standards and regulations into a simple process that can be appliedat any hospital. Presenters will provide practical tips for implementation ofthis process.Learning Objectives:u Identify the various standards and regulations that relate toemergency management programs for hospitals and health systems.u Cite the steps in a generic program development process.u Describe some of the major outcomes <strong>from</strong> this development process.Intended Audience: Emergency physicians, healthcare executives,health education specialists, medical administrators, nurses, pharmacists,physicians, respiratory therapistsWorkshop R: Emergency Management Programs forHealthcare System: Program EvaluationPresenters: Arnie Bierenbaum, BS, MS; Mike Boucher, BSN, MSN;Pete Brewster, BSTime: 1300-1700 hrsRoom: Bayou E<strong>The</strong> purpose of this workshop is to enhance participants’ understanding ofprogram and performance evaluation for emergency management programsin healthcare settings. <strong>The</strong> content is based on past and current researchand programs, including the Veterans Health Administration’s CapabilityAssessment Program, which has created a comprehensive set of targetcapabilities, measures, methods, and scoring profile for use in hospitals.Learning Objectives:u Describe some of the findings <strong>from</strong> past and current approaches toemergency management for health systems program evaluation.u Explain one framework for hospital emergency managementcapabilities.u Describe some of the approaches that can be used for evaluationmeasures, methods, and scoring to reach the overall goal of qualityimprovement.Intended Audience: Emergency physicians, healthcare executives,health education specialists, medical administrators, nurses, pharmacists,physicians, respiratory therapists26<strong>2012</strong> Integrated Training Summit
Tuesday, May 22, <strong>2012</strong>Workshop DescriptionsWorkshop S: Advanced Airway Management inAustere ConditionsPresenters: Leon Dent, MD, MS; Howard Klausner, MD, BSE IOE, FACEP;Marc S. Rosenthal, PhD, DO, FACEPTime: 0800-1200 hrsRoom: Canal BMost patients presenting to an emergency department or a DMAT medicalstation do not require advanced or even simple airway managementtechniques. However, a significant number of patients could require airwayintervention, and for about 5 percent of these patients, based on emergencydepartment experience, advanced airway techniques will be needed tosecure an airway. Unfortunately, while most emergency physicians haveexperience in advanced airway intervention, most family practioners,internists, and others do not have this experience. Should a presentingpatient require advanced airway intervention that cannot be provided, thepatient will most likely die. This end point can potentially be preventedby training DMAT physicians in advanced airway techniques and havingthem practice these techniques in a safe environment. <strong>The</strong> objective of thisworkshop is to provide advanced methods to establish an airway in thedifficult patient. <strong>The</strong> course will cover most advanced airway options, even ifDMATs do not provide the equipment. This approach will further develop theprovider’s skills and improve their ability to establish an airway when theyhave limited resources. In addition, the participants will develop a betterknowledge base on airway anatomy, medications used for intubation, thevariety of approaches that can be used, and simple steps to determine if thepatient will have a difficult airway. With the pathophysiology presented andthe clinical skills taught, participants should improve their ability to establishan airway in a difficult patient with equipment at hand. <strong>The</strong> participantswill develop improved skills for obtaining and securing airways usingadvanced intubation and airway management techniques. <strong>The</strong> participantswill practice these skills during the workshop. Participants will developfurther understanding of difficult airway issues and develop better methodsto determine if a patient will require advanced airway techniques prior toestablishing a secure airway. Finally, the participants will be encouraged tothink outside the box to develop other techniques to establish an airway aswell as to maintain adequate oxygenation and ventilation in patients underaustere conditions.Learning Objectives:u Improve your skill set for emergency airway management.u Develop a better understanding of difficult airways and be able toanticipate a difficult airway.u Develop a better understanding of airway anatomy and currentequipment available to establish an airway.Intended Audience: Emergency physicians, EMT/paramedics, healtheducation specialists, nurses, physicians, respiratory therapistsWorkshop T: Using HSEEP Tools to Develop EffectiveHospital ExercisesPresenter: Mary Massey, BSN, MATime: 0800-1200 hrsRoom: Bayou BSee page 23 for workshop description and objectivesIntended Audience: Emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, industrial hygienists, medical administrators, nurses,pharmacists, physicians, respiratory therapistsWorkshop U: Psychological First Aid (PFA)Presenters: Merritt Schreiber, PhD; Sandra Stark Shields, LMFT,ATR-BC,CTSTime: 0800-1200 hrsRoom: Bayou CThis workshop will present the American Red Cross workshop PsychologicalFirst Aid: Helping Others in Times of Stress. This workshop consists of fiveseparate segments and a series of tabletop exercises and practical tips forproviding basic psychological first aid by non-mental-health providers topatients and team members. <strong>The</strong> workshop provides a framework for practicalunderstanding of the factors that affect stress responses in disaster reliefworkers and the disaster patients they serve. In addition, it provides practicalsuggestions about what you can say and do as you practice the principlesof psychological first aid in real-world disaster settings with culturallydiverse populations. <strong>The</strong> purpose of this workshop is to prepare all nonmental-healthresponders and American Red Cross workers in a common,interoperable model of psychological first aid to provide basic care, comfort,and support to people who are experiencing disaster-related stress.Learning Objectives:u Describe how to recognize the signs of stress in clients, coworkers,and yourself.u Apply psychological first aid principles to provide immediate supportto people who may be experiencing stress.u Describe how to obtain additional mental health support for yourself,coworkers, and disaster victims or clients.Intended Audience: Dentists, emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, industrial hygienists, medical administrators, morticians, nurses,pharmacists, physicians, respiratory therapists, veterinarians<strong>2012</strong> Integrated Training Summit 27Workshop Descriptions
Tuesday, May 22, <strong>2012</strong>Workshop DescriptionsWorkshop DescriptionsWorkshop V: Practical Medication Management inDisastersPresenters: Shannon Manzi, PharmD; Angela Schuman, PharmDTime: 1300-1700 hrsRoom: Canal BThis workshop will offer a practical, hands-on medication preparationand administration course. All types and levels of practitioners who mightbe required to prepare and administer medications on deployment areencouraged to attend. All too often, pharmacists, nurses, and paramedicsmust acquire these unique skills while deployed “in the heat of the battle.”Participants in this workshop will practice medication preparation andadministration skills that may be required in a disaster setting. In additionto the practical skills of dilution, aseptic technique, and compounding,participants will learn about weight-based dosing and pharmaceuticalpreparation relevant to the safe provision of medications in pediatricpopulations <strong>from</strong> neonates to adolescents. Appropriate oral dosage forms,intravenous preparations, IV administration, and IM injection techniques willbe reviewed. A case-based learning approach will be utilized to encourageparticipants to devise unique formulation and administration strategiesgiven simulated environments and resources.Learning Objectives:u Compound basic oral rehydration solutions, reconstitutions (enteraland injectable), and dilutions (enteral and injectable).u Perform weight-based dosing calculations.u Develop strategies to provide appropriate medication formulations forcase scenarios.Intended Audience: Emergency physicians, EMT/paramedics, nurses,pharmacists, physiciansWorkshop W: Medical Skills in the Disaster SettingPresenters: Tony Dunford, EMT-P, RN; Mike Lambert, EMT-P, AATime: 0800-1700 hrsRoom: Governor’s CDisaster planning and emergency preparedness have never been morecritical to the providers who serve as our front-line response. Today’spandemic threats of global terrorism, disease, and natural disastersmake the development of best practices a necessity for a first respondingworkforce that is adequately prepared to respond to any disaster or publichealth emergency. Many of the lessons learned in response to previousnatural and man-made disasters have magnified the deficiencies in trainingof the medical community. Generally, providers practice under controlledsituations with a plethora of resources at their disposal. This situation isnot possible in a disaster setting, where providers must be able to performunder stressful and often suboptimal conditions. However, the firstresponders possess unique skill sets that allow them to be highly effectivein disaster response, including a diverse knowledge base, assessment skills,and a strong commitment to public welfare. <strong>The</strong> first responder may beinvolved in several roles during a disaster. For example, a responder mayfunction as a triage practitioner. This challenging role requires that multiplevictims be assessed and prioritized quickly to ensure that resources are usedappropriately. In remote areas, treatment of patients may be as brief asstabilization and evacuation to more definitive medical care. For providersnot currently working in the patient care setting, the following items will beincluded in the training as well: vital signs (manual); general assessment;immunization and injections; IV access (different types of catheters); bloodglucose monitoring; airway management; nasal trumpet; non-rebreathers;O2 concentrators and tanks; nebulizers. While this training may not beincorporated into the day-to-day practice setting of most providers, it is ofparamount importance in enabling them to work safely and efficiently toprovide quality medical care in an austere environment.Learning Objectives:u Demonstrate patient history and physical exam and proper assessmentskills in taking vital signs.u Demonstrate the proper technique for basic airway management.u Demonstrate assessment skills used in the disaster setting, properadministration of oxygen, and the use of different basic deliverydevices.u Demonstrate proper splinting and stabilization techniques.u Demonstrate the proper steps in using a glucose monitor in a disastersetting; establish IV access and assess the patency of a pre-existing IV site.Intended Audience: EMT/paramedics, nurses, physicians, respiratorytherapists28<strong>2012</strong> Integrated Training Summit
WEDNESday, May 23, <strong>2012</strong>dMIS Workshop DescriptionsDMIS Training<strong>The</strong> following instructors will present the DMIS Training:Jeremy Barnes, MLA, MS; Martha Bartz, RN, MSN, CCRN; ChristianBoone, BA; Shamera Boone, EMT-P; Tori Chesebrough-Buckles, Esq.;Chris Crabtree, MPA, BA; Kendra Frampton, BBA, MA, MP; JonathanGaddy, NREMT; John Howe Jr.; Alicia Jones, DO; Chuck Knell, BS, BA;Jeannie Krick; Kevin Kupitz, PhD, MS; Joseph Lamana, MPA, RN; CindyLarson; Charles Minor; Jeff Orphal; John Probst; Dan Stoudt, MS; GreggTaggard; Laura Walker, AA; Michael Yamamoto, NREMT, BS; Peter Yang,BS; Beth Zealley, MBA, BSTuesday, May 22, <strong>2012</strong>Workshop Y: Disaster Medical Information Suite (DMIS)Review and Updates for InstructorsINVITATION ONLYTime: 1700-1930 hrsRoom: Ryman Ballroom ABInvitation Only: EMR and JPATS Instructors who have previouslyattended an EMR or JPATS Instructor course.This update is designed for ESF#8 personnel who have previous trainingand experience as an instructor with the Electronic Medical Records (EMR)system and/or the Joint Patient Assessment and Tracking System (JPATS).In this session, participants receive a quarterly update on EMR and JPATS.Updates will include:❖ EMR and JPATS software applications❖ Introduction of new or upgraded hardware❖ Instructor development opportunities❖ Exercise and training participation opportunities❖ Evaluation opportunities❖ Responder E-Learn community updates❖ Responder E-Learn module development status❖ Task force projects❖ New instructor resourcesThis workshop will also include lessons learned <strong>from</strong> the 2011 trainingcalendar and deployment season as well as a discussion about the future ofDMIS applications and programs. Participants will be given the opportunityto ask questions and sign up for new opportunities.Learning Objectives:u Discuss lessons learned <strong>from</strong> previous deployments and trainingvenues.u Explain the DMIS application enhancements with course participantsfor an understanding of how these applications will function for any<strong>2012</strong> disaster situation.u Discuss future enhancements and directions for DMIS applications.u Facilitate a question-and-answer session with DMIS instructors.Intended Audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWEDNESday, May 23, <strong>2012</strong>Workshop Z: Electronic Medical Records (EMR) BestPractices: Pearls of Wisdom to Increase ClinicalEfficiencyTime: 1030-1145 hrsRoom: Ryman Ballroom FOpen to the Public: limited to 60 concurrent usersThis workshop is designed for ESF#8 responders who use EMR in thefield. In this workshop, instructors will present lessons learned and bestpractices derived <strong>from</strong> deployments, training, and exercises. Discussionswill focus on the roles and responsibilities of ESF#8 providers in relation totheir responsibilities for administering, monitoring, supervising, or utilizingEMR. Participants will also learn about EMR business practices that increaseclinical efficiency. Participants will learn:❖ Optimal placement of EMR components for various clinical situationsand operations❖ Personnel placement and utilization for optimal clinical operationof EMR❖ Roles and responsibilities of ESF#8 response personnel in relationto the use of EMR❖ Tips for increasing the quality and quantity of informationentered into EMR❖ How to get the most out of EMRPlease come prepared with your questions and plan to participate in aninteractive question-and-answer session. Bring your team’s best practicesto share with others.Learning Objectives:u Discuss EMR best practices with course participants for anunderstanding of how these practices will increase clinical efficiency.u Cite suggestions of placement of EMR hardware for various types ofclinical situations and operations.u Discuss personnel placement and utilization for optimal clinicaloperation of the EMR application.u Discuss the increased use of the EMR application and how to get themost out of it.u Identify the roles and responsibilities of the various clinical positions inrelationship to the use of the EMR application.Intended Audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop AA: Introduction to Joint Patient AssessmentTracking System (JPATS)Time: 1030-1145 hrsRoom: Ryman Studio MNO<strong>2012</strong> Integrated Training Summit 29DMIS Workshops
WEDNESday, May 23, <strong>2012</strong>dMIS Workshop DescriptionsDMIS WorkshopsOpen Access: limited to 60 participantsThis workshop will provide an overview of JPATS, the HHS web-basedapplication that tracks patients through the Federal patient movementsystem. Participants will review the Federal patient movement system andlearn how JPATS is used to track patients <strong>from</strong> their entry into the systemto their return to origin or final destination. A walk-through of the JPATSsoftware application will include:❖ Creating an account❖ Registering new patients❖ Managing patient dispositions❖ Receiving and updating patients❖ Building manifests❖ Creating reports❖ Using dashboardsInstructors will walk participants through a guided tour of the application.<strong>The</strong>y will also discuss best practices and lessons learned <strong>from</strong> actualdeployments, field exercises, and training.After completing the workshop, participants may attend the JPATS BasicApplication Training workshop or visit the DMIS Hands-On Lab, where theycan gain a better understanding of the JPATS web application throughfacilitated hands-on practice with patient scenarios.Learning Objectives:u Describe the role of JPATS in the Federal patient movement system.u Describe the procedure for registering patients.u Discuss how changes in patient disposition are captured in JPATS.u List and describe the reports available in the JPATS application.u Describe the data elements found on the JPATS dashboard.Intended Audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop BB: Basic Information Technology (IT) forElectronic Medical Records (EMR): Clinical and IT UsersTime: 1315-1430 hrsRoom: Ryman Ballroom DEOpen to the Public: limited to 30 concurrent usersThis workshop will allow participants to become familiar with the basic ITrequirements of the Electronic Medical Records (EMR) system. EMR is theapplication that ESF#8 responders use to capture patient encounters duringa disaster. Participants will participate in a facilitated walk-through of thebasic IT requirements for EMR setup and maintenance. This workshop willalso include:❖ Demonstration of the basic hardware configuration and supportingsoftware infrastructure❖ Instruction on establishing a local area network (LAN)❖ Review of EMR setup in base of operations (BoO)❖ EMR stand-alone setup❖ Hands-on practice with the hardware and networking components❖ Identifying additional IT resources for troubleshooting in the fieldParticipants wanting more experience with the system application shouldconsider attending the Electronic Medical Records Overview workshop.Additional hands-on practice may be gained by attending the DMIS Hands-On Lab.Learning Objectives:u Identify and review EMR hardware and networking components.u Describe the integration of the hardware configuration and thesupporting software infrastructure.u Describe the goals and performance standards associated with EMRsetup in the BoO.u Demonstrate the EMR system and stand-alone setup.u List the resources for obtaining additional IT support in the field.Intended Audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop CC: Joint Patient Assessment TrackingSystem (JPATS) Basic Application TrainingTime: 1315-1430 hrsRoom: Ryman Ballroom ABOpen Access: limited to 30 participantsThis workshop will allow participants to become familiar with the latestversion of the JPATS web application. Following a brief review of theapplication, attendees will participate in instructor-led interactive lessonsand exercises. Participants will learn all of the elements necessary tosuccessfully master the JPATS application and track a patient through theFederal patient movement system. This workshop is geared to the new orinexperienced user. Experienced users may consider attending the JPATSRefresher workshop.Participants wanting a more extensive review of the application beforeparticipating in hands-on training should consider attending the Introductionto JPATS workshop. Additional hands-on practice may be gained by attendingthe DMIS Hands-On Lab.Learning Objectives:u Describe the role of JPATS in the Federal patient movement system.u Demonstrate the procedure for registering patients.u Demonstrate how changes in patient disposition are captured in JPATS.u Generate each type of report and identify the data contained in thereport.u Using the data elements found on the JPATS dashboard, recite a verbalsummary report of patient movement activity at a specific location.u List the resources for obtaining additional IT help in the field.Intended Audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapists30<strong>2012</strong> Integrated Training Summit
ThurSday, May 23, <strong>2012</strong>dMIS Workshop DescriptionsWorkshop DD: Electronic Medical Records (EMR)OverviewTime: 1515-1645 hrsRoom: Ryman Ballroom FOpen to the Public: limited to 40 concurrent usersThis workshop will allow participants to become familiar with v.6 of theElectronic Medical Records (EMR) application. EMR is the application thatESF#8 providers use to capture patient encounters and document patientcare during a disaster. A facilitated review of the EMR application includes:❖ Primary components of EMR❖ Safety features, including mandatory fields❖ User management❖ Provider dashboards❖ Auxiliary devicesParticipants in this workshop will learn how the EMR application isintegrated into DMIS to provide the most complete information about themedical care of patients treated during deployments. Following a facilitatedwalk-through of EMR, participants will have an opportunity for hands-onpractice with the application.Participants wanting more experience with the system setup should considerattending the Basic Information Technology for Electronic Medical Recordsworkshop. Additional hands-on practice may be gained by attending theDMIS Hands-On Lab.Learning Objectives:u Provide a facilitated walk-through of the EMR software application.u Complete an instructor-led, hands-on practice session using targetedpractice scenarios.u Identify and describe the hardware in the EMR cache.u Review the roles and responsibilities of ESF#8 responders.u Discuss the relevance and applicability of EMR in the context of therole of the ESF#8 responder.u Describe how the EMR application is integrated into DMIS to provideinformation during response.Intended Audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapiststhurSday, May 24, <strong>2012</strong>Workshop EE: Joint Patient Assessment TrackingSystem (JPATS) RefresherTime: 0800-1000 hrsRoom: Ryman Ballroom FOpen Access: limited to 40 participantsThis workshop will allow experienced users an opportunity to becomefamiliar with the latest version of the JPATS web application. Following abrief review of the changes in v.4, participants will participate in a hands-on,simulated, patient movement exercise featuring JPATS v.4. Participants willregister and track patients <strong>from</strong> the casualty collection point to definitivecare through return to home. <strong>The</strong> exercise will allow participants to workthrough advanced scenarios and troubleshoot common problems. Newmobile platforms and data capture technology will be featured for use inthe exercise. NDMS participants completing the exercise will satisfy thebiannual refresher requirement for the HHS JPATS Strike Team.This workshop is for the experienced user only. Basic application training willnot be covered in this workshop. Inexperienced or new users may considerattending the Introduction to JPATS and JPATS Basic Application Trainingworkshops.Learning Objectives:u Review the changes in functionality in version 4.u Demonstrate the procedure for capturing and attaching patientphotos.u Set up and demonstrate the barcode scanner.u Complete patient manifests.u Generate each type of report and identify the data contained in each.u Using the data elements found on the JPATS dashboard, recite a verbalsummary report of patient movement activity at a specific location.u List the resources for obtaining additional IT help in the field.Intended audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop FF: Electronic Medical Records (EMR)Best Practices: Pearls of Wisdom to Increase ClinicalEfficiencyTime: 1030-1145 hrsRoom: Ryman Ballroom FSee page 29 for course description.Intended audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsDMIS Workshops<strong>2012</strong> Integrated Training Summit 31
THURSday, May 24, <strong>2012</strong>dMIS Workshop DescriptionsDMIS WorkshopsWorkshop GG: Introduction to Joint Patient AssessmentTracking System (JPATS)Time: 1030-1145 hrsRoom: Ryman Ballroom CSee page 29 for course description.Intended audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop HH: Basic Information Technology (IT) forElectronic Medical Records (EMR): Clinical and IT UsersTime: 1315-1430 hrsRoom: Ryman Ballroom DESee page 30 for course description.Intended audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop II: Joint Patient Assessment Tracking System(JPATS) Basic Application TrainingTime: 1315-1430 hrsRoom: Ryman Ballroom ABSee page 30 for course description.Intended audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapistsWorkshop JJ: Electronic Medical Records (EMR)OverviewTime: 1515-1645 hrsRoom: Ryman Ballroom FSee page 31 for course description.Sharing the Disaster Medical Information Suite (DMIS)applications: Question & Answer SessionTime: 1515-1645 hrsRoom: Ryman Studio MNOMany states, local jurisdictions, and hospitals have expressed interest inobtaining more information about the DMIS applications. In this workshop,participants will get a brief overview of the JPATS implementation process.Attendees will participate in an interactive discussion covering topics suchas compatibility, HL7 requirements, privacy laws, hardware requirements,training, software procurement and customization and many more.Presenters will also share lessons learned <strong>from</strong> experience with Stateimplementations.Please come prepared with your questions and plan to participate inan interactive question and answer session. Copies of the JPATS StateImplementation Guide will be available. Find out how to work with yourHHS Regional Emergency Coordinator to obtain additional informationabout the process specific to your location.friday, May 25, <strong>2012</strong>Workshop KK: Electronic Medical Records (EMR)Best Practices: Pearls of Wisdom to Increase ClinicalEfficiencyTime: 0800-0945 hrsRoom: Ryman Ballroom CSee page 29 for course description.Intended audience: Emergency physicians, EMT/paramedics, nurses,physicians, respiratory therapists32<strong>2012</strong> Integrated Training Summit
SessionDescriptionssession Descriptions<strong>2012</strong> Integrated Training Summit 33
wednesday, May 23, <strong>2012</strong>Session Descriptionssession DescriptionsWEDNESday, May 23, <strong>2012</strong>Session 01: Opening CeremonyTime: 0830-0900 hrsRoom: Delta A BallroomSession 02: <strong>Preparedness</strong> and Professionalism inPublic Health and Disaster Management: HistoricalReflectionsPresenter: Dale Smith, PhDTime: 0900-1000 hrsRoom: Delta A BallroomFocus Area: General SessionIn 1793 the ports of the United States were hit by a terrible yellow feverepidemic. In the new nation’s largest city, Philadelphia, this epidemic hadmany effects that have attracted the attention of historians, and one ofthe most far-reaching was the argument, eventually successful, made byBenjamin Rush that members of a profession had a responsibility to thelarger community, not just their paying customers. In the centuries thatfollowed, in epidemic and disaster, the health and safety professionshave discovered many individual and important tools and techniques tomanage disasters, some of which will be highlighted. However, the costsof preparedness are real and immediate, as Ibsen noted in An Enemy ofthe People: “the majority never have right on their side.” As a result, mostpreparedness is achieved after the fact of a disaster for which the communitywas inadequately prepared. As the flu threat and immunization campaign of1976 demonstrated, preparedness without disaster can lead to significantpublic criticism. Perhaps most importantly, as many new environmentalthreats emerged and independent professional traditions evolved in thetwentieth century, it became clear that interprofessional education andcooperation would be crucial to future progress in the management of andrecovery <strong>from</strong> disasters and public health emergencies.Learning Objectives:u Outline the development of the professional obligation to thecommunity.u Provide three examples of learning preparedness <strong>from</strong> disasters.u Recognize and outline the importance of different skill sets andprofessions in response to late twentieth-century domestic disasters.Session 03: Integrating Resilience intoDisaster Medical CarePresenters: LCDR Meghan Corso, PsyD; CAPT David Morrissette, PhD,LCSWTime: 1030-1145 hrsRoom: Bayou CDFocus Area: Healthcare Systems<strong>The</strong> panel will present a model of disaster medical care that integratesbehavioral health into overall physical and emotional health and buildsresilience among survivors of disasters. This model drastically changes theoften stigmatizing approach of traditional mental health and its applicationto a disaster response. Specifically, this model focuses on a whole-personwellness approach to behavioral health care delivery in a disaster response.Survivors are solicited for common physical, emotional, or behavioralconcerns and briefly treated in conjunction with the medical care services.<strong>The</strong> goal is to augment the medical services being delivered as well as providebehavioral health care that is less stigmatized and addresses the needs ofthe whole person including adjustment to the disaster, grief, mental illness,or substance abuse. Lastly, this model will assist the survivors in buildingresilience through education and encouragement of healthy behaviors. <strong>The</strong>panel will present an urgent care scenario in which a behavioral healthteam deployed a Wellness Center to augment medical care. Using selfreferral and physician referral forms citing common reactions to disaster, ie,eating, sleeping, emotional stress, substance use, and isolation, patients areprovided with brief counseling and education. As a result, more than one outof every four sought behavioral health consultation and without disruptionor delay to the provision of other health services. <strong>The</strong> panel will present aresilience model that is particularly well suited to a disaster response to:integrate behavioral health with medical services through education andcounseling on self-care; address common behavioral reactions to disasterand loss; normalize common responses to trauma exposure and buildresilience; create opportunities to screen and assess for suicide, depressionand acute stress response; destigmatize mental health and substance abusescreening, treatment, and referral.Learning Objectives:u Explain the concept of wellness in improving resilience and how it canbe implemented in a medical disaster response.u Operationalize concepts for implementation in a medical disasterresponse.u Describe clear roles for behavioral health providers in medical settings.Intended Audience: Certified counselors, emergency physicians, EMT/paramedics, healthcare executives, health education specialists, industrialhygienists, marriage & family therapists, medical administrators, nurses,pharmacists, physicians, social workersSession 04: Palliative Care Considerations inDisaster SituationsPresenters: Carma Erickson-Hertz, MS; Marianne Matzo, PhD, GNP-BC,FPCN; Tia Powell, MD; Jon Surbeck, MATime: 1030-1145 hrsRoom: Bayou EFocus Area: Healthcare SystemsPalliative care has implications during disasters. While we routinely improvethe quality of life and mitigate suffering for people facing serious illness,our disaster preparedness planning efforts often fail to account and planfor those patients who will die <strong>from</strong> illness, injury, or lack of access to lifesavingresources during disasters. In mass casualty events, it is likely therewill be more patients who require care than we have resources to treat.Those patients will require palliative care techniques, like pain and symptommanagement. Secondly, we will need to maintain services for those receivingpalliative care services at the time of the disaster. Advanced illness and endof-lifecare pose particular challenges during health emergences, givencomplex care needs and the often competing demands for trained providers,34<strong>2012</strong> Integrated Training Summit
wednesday, May 23, <strong>2012</strong>Session Descriptionsmateriel, and space. This session will present and compare existing nationalguidelines for health emergency response, focusing on issues related topalliative and end-of-life care. Special attention will be given to the surgecapacity planning needs of hospice and palliative care providers and toproviding tools for leveraging their expertise to maximize care for patientswith serious, advanced illness.Learning Objectives:u Discuss Health and Human Services (HHS) templates for states,emergency medical services (EMS) systems, hospitals, and individualclinicians to guide decision making when implementing crisisstandards of care that can be easily read, understood, and executedduring an incident.u Explain existing guidelines for scarce resource allocation and crisisstandards of care, and their implications for surge capacity planningfactors for hospice and palliative care providers.u Identify potential disaster scenarios that might be faced at the localand state level, requiring palliative care services.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,pharmacists, physicians, psychologists, social workersSession 05: Passing the Torch: Succession PlanningDone Right?Presenter: Teddy Rogers, MSA, NREMT-PTime: 1030-1145 hrsRoom: Delta CFocus Area: LeadershipOne of the primary tasks of any quality leader is the continual and progressivework around succession planning. <strong>The</strong>re are those who say a great leadermay not be replaceable, and then there are those who say a great leadershould have prepared for such a transition. <strong>The</strong> successful leader’s roleis to literally plan to be replaced! <strong>The</strong> welfare of any great organizationdepends upon this premise. <strong>The</strong> primary acts that a great leader performs toprepare for successful transitions are casting vision, planting and guardingthe organizational culture, and fostering an environment where subordinateleaders can perform in a fail-safe manner, free to make mistakes and learnwithout sinking the organization as a whole. This session will center onthese three primary acts that, if done correctly and proactively, will lay theframework for a successful transition in any organization. Finally, the greatleader must learn firsthand that the success or failure of such a transition liescompletly within. Ego management, overconfidence or lack of confidence,and personal motives and behaviors are all critical in any leadershiptransition. If you are in a leadership position, you have a job to do. Planto leave the day you are hired, because you will leave whether you wantto or not!Learning Objectives:u Describe the intrinsic value of performing the three acts of successionplanning offered in this course and how to do them.u Discuss the importance of looking within in order to successfully passthe torch. Ironically, what’s inside you will come out when you leave,like it or not.u Demonstrate the process of passing the torch!Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinariansSession 06: Chaplaincy Support for DisasterDeployment ResponsesPresenter: Catherine Witte, RPh, MDivTime: 1030-1145 hrsRoom: Delta DFocus Area: LeadershipAs stated by Dr. George Everly, Co-Founder and Chairman Emeritus of theInternational Critical Incident Stress Foundation, “It has been commonlyobserved that in times of crisis and disaster, many individuals seek outreligious or spiritual leaders,” but it it has only been within the last 10 or15 years that spiritual care has been formally integrated into many types ofdisaster response missions. <strong>The</strong> provision of spiritual and emotional supportin a timely and appropriate manner to those impacted by disasters has thebenefit of mitigating short and longer-term distress (emotionally, spiritually,and physically) for individual survivors, communities, first responders, andothers involved in providing disaster relief. Chaplains with specialized trainingtypically use various methods and approaches in providing spiritual careservices in disaster response, and examples of these will be discussed. Aswith other components within disaster response, spiritual care is a field thatis growing and adapting to most effectively meet the needs and challengesof diverse communities. Encouraging collaborative partnerships in providingspiritual care within communities and across agencies serving those in needwill be essential for the success of the overall disaster response mission.Learning Objectives:u Discuss a history and overview of spiritual care services as a formalcomponent in disaster response.u Define the role and function of chaplains and others providingspiritual care within the incident command and disaster responseoperation.u Describe planning, methods, and execution of spiritual care servicesas an integrated component of USPHS and other agency disasterresponse missions.Intended Audience: Certified counselors, emergency physicians, EMT/paramedics, healthcare executives, health education specialists, marriage& family therapists, medical administrators, morticians, nurses, physicians,social workers<strong>2012</strong> Integrated Training Summit 35session Descriptions
wednesday, May 23, <strong>2012</strong>Session Descriptionssession DescriptionsSession 07: DRAT! (Disaster Readiness Actions forTeens) and North Minneapolis Tornado <strong>Recovery</strong>Presenters: Nancy Carlson, BS, CFT, CFE; Michael Thomas, PsyD, LPTime: 1030-1145 hrsRoom: Governor’s AEFocus Area: Public HealthOn May 22, 2011, the worst tornado to hit Minneapolis in 30 yearspummeled the north side of Minneapolis in a high-poverty area with a highpercentage of rental property, multifamily homes, and subsidized (morethan 80% in some areas) housing. A Behavioral Health <strong>Recovery</strong> Committeewas developed, consisting of Hennepin County, City of Minneapolis, Healthand Family Support, North Point Center for Health & Wellness, and MNDepartment of Health (MDH), through grant funding by the MN Departmentof Human Services. Our focus was on youth recovery, since we knewthat in working with the children we would also help tornado-impactedfamilies and communities to recover. <strong>The</strong> MDH DRAT! Disaster ReadinessActions for Teens program was chosen as our vehicle for postemergencypreparedness education. DRAT! is a youth emergency preparedness trainingprogram specifically geared for tweens (ages 10-12) and teens with the goalof engaging, educating, and empowering youth to respond safely duringcritical incidents such as natural disasters, man-made incidents, publichealth emergencies, and school threats. <strong>The</strong> DRAT! program name and logowere determined by surveying MN youth aged 10-18 via word of mouth andwith an online Twitter and Facebook survey. A youth focus group was utilizedto review content and ensure that it connected with our population and metthe program goal of engaging, educating, and empowering youth to respondsafely during crises and disasters. <strong>The</strong> program contains six modules: WhyPrepare, Stay Safe, Make a Plan, Make a Kit, Stay Calm, and Celebration ofKnowledge. Our initial goal consisted of training 100 youth by providingfive 1½-hour training sessions to groups consisting of 25 tweens/teens. Wedetermined that due to the potentially traumatized and disaster-impactednature of our audience, we would focus mainly on the modules discussingmaking plans, staying safe, and staying calm. Our trainers consisted of alicensed mental health professional to teach the youth psychological firstaid (PFA) module teamed with a peer trainer for the preparedness content.This session will discuss the need for a youth focus in disaster recovery andreview: the DRAT! training modules; emergency preparedness kit; youthpsychological first aid training and Youth PFA card; our training plan andhow we adapted and implemented the program; effectiveness based ontrainer debriefing and participant evaluations; and next steps in youth andcommunity recovery and resilience building.Learning Objectives:u Describe how to use a youth emergency preparedness program as acommunity disaster recovery tool.u Discuss how to implement psychological first aid training for youth asa means to reduce disaster stress symptoms and encourage ongoingdaily stress reduction and healthy self-care behavior.u Assess the effectiveness of youth emergency preparedness planningin youth disaster behavioral health recovery and overall communityresilience building.Intended Audience: Certified counselors, emergency physicians, EMT/paramedics, healthcare executives, health education specialists, marriage& family therapists, medical administrators, morticians, nurses, physicians,psychologists, social workersSession 08: Medication Needs of Survivors with ChronicConditions to Prevent Deterioration During ShelteringPresenter: Charles Stewart, MD, EMDM, MPH(c)Time: 1030-1145 hrsRoom: Bayou ABFocus Area: Public Health<strong>The</strong> recent Japanese earthquake and subsequent tsunami, HurricanesKatrina, Ike, and Gustav, and the Indian Ocean tsunami have focused ourattention on the need for disaster preparedness and mitigation. Large cities,such as Tokyo, New York, San Francisco, and St. Louis, remain at high riskfor catastrophic loss of life <strong>from</strong> weather, earthquake, or man-made disaster.Such large-scale disasters affect every segment of society, though it is clearthat some segments are more vulnerable than others. Treatment of thepatient who is injured in a disaster is a well-considered part of the overallplans by the emergency manager and the medical community at large.Other populations, such as children, nursing home residents, prisoners,pregnant women, respirator-dependent patients, those on dialysis, the frailelderly, and chronically disabled individuals, have been identified in othervenues. Extensive research has been published on disasters, health caredisparities, and medically underserved populations, but little attention hasbeen paid to those with chronic diseases who will decompensate withouttheir medications or treatments. A major category of vulnerable childrenand adults includes those with chronic treatable illnesses such as diabetes,COPD, seizures, hypertension, heart disease, and even chronic painsyndromes. This population may normally lead productive lives with littleor no external signs of disability. Given a few days without their supportivemedication, however, they may require intensive care and consume preciousmedical resources. If these people are displaced abruptly <strong>from</strong> their home orworkplace, their medications may be left behind or destroyed in the disaster.We attempted to compile a list of medications that should be consideredfor those planning shelters or nonemergent care facilities in the wake of adisaster. What medications will urgent care providers (in shelters or similarsituations) need to provide these patients to prevent deterioration of theircondition? To create a meta-analysis, the authors reviewed literature <strong>from</strong>2000-2011 using the key words “chronic,” “disaster,” “disease management,”“planning,” and “preparedness.” Searches were performed using Google,Google Scholar, and PubMed for medications required in the first week ofsheltering in disasters.Learning Objectives:u Identify those chronic diseases that will require additional attention toprevent decompensation during sheltering operations.u Explain why prompt intervention in chronic disease care in shelteredpatients will decrease the burden on overtaxed medical resources.u List chronic disease medications that emergency planners shouldconsider in arranging stockpiles, caches, and deployment packages.36<strong>2012</strong> Integrated Training Summit
wednesday, May 23, <strong>2012</strong>Session DescriptionsIntended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,pharmacists, physicians, social workersSession 09: Triage in the Field: Taking It to theNext LevelPresenters: LT Christine Collins, BSN, MA; Jerardo Gomez, BSOE, AAS;David Torres, AASTime: 1030-1145 hrsRoom: Governor’s CFocus Area: Resource Management and Patient MovementTriage is a process for prioritizing the treatment and movement of casualtiesin order to provide the greatest care to the greatest number, achieving thebest possible outcomes. Effective triage and appropriate patient classification(Minimal=Green, Delayed=Yellow, Immediate=Red, and Expectant=Black)will maximize the life and limb-saving capabilities of medical personnel,equipment, and facilities. Providing hands-on, case-based scenarios withthe use of a human patient simulator will facilitate a comprehensive trainingenvironment, meeting the needs of all skill levels. <strong>The</strong> human patientsimulator is a computer-driven, multidiscipline tool that will demonstratea variety of human physiologic conditions related to injuries sustained <strong>from</strong>mass casualty events. Participants will be given instant and post-simulationfeedback during their demonstration of triage classification and medicalinterventions based upon the patient’s initial assessment and mechanism ofinjury. Since real-world emergency situations provide no room for error, thisparticular virtual learning environment will promote improved real-worldtriage care and increase the confidence of our medical responders.Learning Objectives:u List and define the four categories and colors of triage.u Verbalize and demonstrate the ability to properly triage and explainthe mechanism of injury with appropriate lifesaving intervention.u Recite appropriate physiologic theoretical data on virtual humanpatient simulator casualties and place them in their respectivecategories.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,pharmacists, physicians, respiratory therapistsSession 10: ESF#8 Patient Tracking Force MultiplierPresenters: Knox Andress, RN, BA, AD; John Donohue, BS, EMT-P;Timothy Grapes, BA; Joe Lamana, MA, BA; Paul Petersen, PharmD, BCPSTime: 1030-1145 hrsRoom: Governor’s DFocus Area: Resource Management and Patient MovementMonitoring interstate and multi-jurisdictional patient movement duringemergencies has historically presented great challenges. Over the past twoyears, the Department of Homeland Security, the Department of Healthand Human Services, and their partners have worked collaboratively toidentify and develop holistic solutions that address tracking of patientswhile improving the overall situational awareness. This truly interactivesession will monitor the movement of the session participants in real timeas they are tagged (banded), registered, and moved among “locations” inthe room representing four disparate systems. Participants will be able to seethemselves being simultaneously transferred between systems and locationsas “emergency patients.” This session will include solutions for tracking bothNational Disaster Medical System (NDMS) and non-NDMS patients. Trackingsystems discussed and utilized will include those <strong>from</strong> Louisiana, Maryland,Tennessee, and the NDMS Joint Patient Assessment and Tracking System(JPATS). Overviews will include Federal, state, and local system roles andrelationships across the patient tracking continuum, including the TranscomRegulating and Command & Control Evacuation System (TRAC2ES) and others.This session will demonstrate how easily crucial information concerning thecare and tracking of patients can now occur to provide 360-degree situationalawareness during an emergency. Longitudinal patient tracking informationcan be maintained. <strong>The</strong> ability to electronically receive data-rich manifestsallows responders to lean forward and assist in ways never possible before inmass patient evacuation emergencies. With the aggregate data <strong>from</strong> thesecombined tracking systems, Department of Health and Human Services, theOffice of the Assistant Secretary for preparedness and Response (HHS/ASPR)can be fully aware of the locations and conditions of people, enabling a moredirected response while improving the ability of locating missing persons.Participants will be introduced to emerging data exchange standards,methods to seamlessly track patients in emergencies, bar coding technology,use of triage tagging systems, and mobile software applications. <strong>The</strong> sessionwill also delineate for participants implementation options available to theirorganization, provide step-by-step instructions, and identify organizationaland technology impediments to successful implementation. <strong>The</strong> session willalso introduce participants to the use of the National Health InformationNetwork (NHIN) and FEMA Integrated Public Alert and FEMA IntegratedPublic Alert and Warning System (IPAWS).Learning Objectives:u Describe the emerging data exchange architecture that is beingestablished to provide patient tracking in a timely and meaningfulfashion for future emergencies.u Explain how patient tracking systems and secure message routing canbe used for critical situational awareness during emergencies involvingmultiple jurisdictions and states.<strong>2012</strong> Integrated Training Summit 37session Descriptions
wednesday, May 23, <strong>2012</strong>Session Descriptionssession Descriptionsu Assess the ability of the participants’ current organization,infrastructure, and communications capability to support effectivepatient tracking during emergencies.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, industrial hygienists, marriage & family therapists, medicaladministrators, nurses, physicians, social workersSession 11: Zombie Emergency: All-Hazards Emergency<strong>Preparedness</strong> InstructionPresenter: Jeffrey Bratberg, MDTime: 1030-1145 hrsRoom: Delta BFocus Area: Response Integration/Operational MedicineIn May 2011, the Centers for Disease Control (CDC) Health Matters Blogposted one of the most commented-upon and viewed posts on all-hazardspreparedness, <strong>Preparedness</strong> 101: Zombie Apocalypse (http://blogs.cdc.gov/publichealthmatters/2011/05/preparedness-101-zombie-apocalypse/). In thespring of <strong>2012</strong>, the University of Rhode Island College of Pharmacy organizedan elective class, Public Health Consequences of Infectious Diseases, onemerging infectious diseases, including a practical component on all-hazardsemergency preparedness and response. While the didactic portions of theclass involved student groups researching and presenting past responsesto actual emerging infectious disease outbreaks, the practical responseinvolved students planning and testing a new College of Pharmacy buildingas a primary point of dispensing (POD) during an outbreak of a hypotheticalinfection that creates zombies, thus mimicking an outbreak of an unknown,yet highly communicable and terrifying infectious disease. Using borrowedsignage and materials <strong>from</strong> the state health department’s Center forEmergency <strong>Preparedness</strong> and Response (CEPR) municipal POD Go-Kit, thestudents set up a POD in real time and recruited faculty, staff, and studentsas volunteers to attend the POD, serve in the POD, and attack the POD aszombies. Evaluators <strong>from</strong> other universities, cities and towns, and the statewere able to view the POD flow and activities through the glassed-in roomsused in the POD. This activity was also combined with a student pharmacist–run repackaging exercise in association with CEPR, providing “Zombiecycline”for dispensing in the POD. Evaluators also observed the activity. Finally, fourgroups of student pharmacists in the elective class produced public serviceannouncements outlining the mitigation, preparedness, response, andrecovery <strong>from</strong> the zombie apocalypse, with guidance <strong>from</strong> the CDC PublicHealth <strong>Preparedness</strong> and Response Zombie Task Force. It is hoped that thePOD location will be used for future actual and exercise responses, potentiallyincluding pharmacist-administered influenza immunizations to the staff,faculty, and students at the university as a pandemic influenza exercise.Learning Objectives:u Define the value of collaboration of university health professionalschools, CDC, and state health departments in emergency responsetraining activities.u Evaluate the effectiveness and pitfalls of using a technologicallyadvanced university building as a POD site staffed by studentvolunteers.u Develop a plan to enhance higher education and public healthcollaboration for all-hazards preparedness and response.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, industrial hygienists, marriage & family therapists, medicaladministrators, nurses, pharmacists, physicians, social workersSession 12: Operational Medicine: Past, Present,and FuturePresenters: CAPT Allen Dobbs, MD; David Marcozzi, MD, MHS-CL,FACEP; Sean Siler, DOTime: 1030-1145 hrsRoom: Governor’s BFocus Area: Response Integration/Operational MedicineWhat is operational medicine? Operational medicine (OPMED) is definedas care provided in an unconventional setting where access to traditionalresources may be significantly limited. This can include working with limitedsupplies, staffing, or time as well as under extremes of climate, location, orenvironment. OPMED includes components of disaster, military, wilderness,frontier, emergency, pre-hospital, tactical, and international medicine.<strong>The</strong> concept of OPMED, perhaps best defined by the military experience,resonates with the emergency preparedness and response community.“Good medicine under challenging conditions” is an appropriate phrase<strong>from</strong> Afghanistan to Joplin. Whether <strong>from</strong> war or disaster, the practice ofmedicine in an affected community will be significantly different comparedto one that is intact. Poor environmental conditions, limited supplies, longhours, and high patient volumes are common variables regardless of thesetting. However, fundamental differences exist between the military andcivilian practice of OPMED. <strong>The</strong>se differences will shape the delivery of carein the civilian disaster environment.<strong>The</strong> presenters will introduce examples of OPMED missions, discuss howOPMED principles may differ <strong>from</strong> the typical care delivered in the UnitedStates, and emphasize the opportunities for ESF#8 responders to benefit<strong>from</strong> the lessons learned across the other disciplines of OPMED <strong>from</strong> aroundthe globe. This session will serve as a kickoff lecture to frame the othersessions in the new OPMED track at the <strong>2012</strong> Integrated Training Summit.This session will explore many of the issues faced by civilian practitionersin the disaster environment and address how they may be able to adaptsome of the principles of OPMED to help them carry out their mission. Inparticular, the panel will discuss how the concepts of OPMED have beenand will be incorporated into the ESF#8 response to disasters and publichealth emergencies. <strong>The</strong> presenters have experience in civilian and militarymedicine under a wide range of environments.Learning Objectives:u Define what the specialty of operational medicine is and the role ofoperational medicine in ESF#8.u Explain common conceptual approaches to operational medicinepatients, and then define how the environment of care requiresvariations.38<strong>2012</strong> Integrated Training Summit
wednesday, May 23, <strong>2012</strong>u Provide examples of how the priorities of delivering care in a resourcechallengedenvironment may differ <strong>from</strong> the delivery of care undernon-challenged environments.u Describe how physiology rather than resources defines healthcare, andidentify two approaches that differ <strong>from</strong> traditional care.u Describe an example of lessons learned <strong>from</strong> military medicinethat would benefit civilian ESF#8 medical personnel operating in aresource-challenged environment.Intended Audience: Emergency physicians, EMT/paramedics, nurses,pharmacists, physiciansSession 13: Advancements in HPP Regional HealthcareCoalitions: Utah’s ExperiencesPresenters: Kevin McCulley, BS; Sara Sinclair, RN, CNHA, FACHCATime: 1315-1430 hrsRoom: Bayou CDFocus Area: Healthcare Systems<strong>The</strong> ASPR Hospital <strong>Preparedness</strong> Program provides a framework and minimalset of objectives for the development of regional healthcare coalitions, whileappropriately leaving important coalition structural and functional decisionsto states. <strong>The</strong> State of Utah, through partnerships between the Departmentof Health and its local health districts, have developed a successful coalitionmodel that utilizes local health districts as hosting agencies for coalitions.<strong>Through</strong> this partnership, critical community linkages have been sustained,new collaborative partners have been identified, and preemptive preparationsfor the alignment of CDC PHEP and ASPR HPP have been completed. Thissession will provide an overview of the strategies, methods, and challengesrelated to partnering with local health departments for regional healthcarecoalition hosting. <strong>The</strong> session will address the processes utilized to developproject objectives, timelines, and funding allocations. Structural topics willbe reviewed, including the identification, recruitment, and retention ofcoalition partners, the development of core program documents includingMOU/A, coalition charters, and regional response plans. <strong>The</strong> target audiencefor this session will be local, district, and state level staff involved in theimplementation and development of regional healthcare coalitions.Learning Objectives:u Design a plan to determine the regional healthcare coalition structurethat will be successful in the participant’s state, and identify localpartners that will contribute to successful outcomes.u Compare the benefits and challenges of utilizing local health districtsas hosting agencies for coalitions.u Analyze the process of coalition objective development, and determinehow these objectives could be implemented in other states.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,physiciansSession DescriptionsSession 14: Emergency Planning for Safe andAppropriate Management of Behavioral HealthPatients During DisastersPresenters: Diane Angelico, Cassandra Suzette WilsonTime: 1315-1430 hrsRoom: Bayou EFocus Area: Healthcare SystemsAs a part of the Florida Department of Health efforts to continue to expandand improve partnerships and joint efforts with health care system partners,the Medical Surge Program has explored a number of approaches to engagepartners. In August 2011, a short survey was sent to hospital and hospitalsystem partners. <strong>The</strong> purpose of the survey was to determine the level ofinterest in short, scheduled, virtual meetings for the exchange of information.<strong>The</strong> distribution lists included 175 unduplicated email addresses. Ninetynineresponses were received with only one negative response. As a result ofthis initial interest, a number of short programs will be offered. <strong>The</strong> programcontent is based on an assessment and prioritization by the target audience,our hospital partners at the direct service level. <strong>The</strong> role of the department isto facilitate and promote participation. To make the sessions more attractiveto participants, continuing education credit is offered as appropriate. <strong>The</strong>presenters come <strong>from</strong> the disciplines that have the highest level of expertisefor the subject area. For example, some sessions, such as safety and securityor active shooter, include a law enforcement component. Use of virtualmeeting technology allows us to have statewide participation. Participantsreceive announcements, registration information, and program materialselectronically. Much of the material and samples shared can be downloadedand customized for site-specific use. <strong>The</strong> initial plan was to limit participationto about 50 sites or participants. <strong>The</strong> first program offered was “UsingDisaster Core Competencies for Hospital Personal.” <strong>The</strong> presenters includeda nurse <strong>from</strong> a small critical access hospital with 25 beds in a rural areaof Florida, a representative <strong>from</strong> a medium hospital with 250 beds, and aphysician <strong>from</strong> a 700+ facility in a large urban area. We were also fortunateto have a hospital health care system rep who addressed how he was able touse the competencies in his system. <strong>The</strong> exchange of information connectedproviders that had not previously had contact and led to a commitmentto share sample materials such as memorandums of agreement. <strong>The</strong> finalcount for the webinar was 64 participants. <strong>The</strong> number may be higher asmore than one person could view and participate in the program once a sitewas logged in. <strong>The</strong> evaluations have been very favorable and a number oftopics have been suggested for future programs.Learning Objectives:u Provide an overview of using short JIT information sharing andtraining programs to address emerging preparedness issues for healthcare system providers.u Demonstrate improved and increased sharing of information and bestpractices between hospitals and health care system partners.u Describe examples of increased engagement of hospitals andstrengthened partnerships between the department and hospitals.session DescriptionsIntended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,physicians<strong>2012</strong> Integrated Training Summit 39
wednesday, May 23, <strong>2012</strong>Session Descriptionssession DescriptionsSession 15: Engaging Youth: A Key Component ofSuccession PlanningPresenters: Ada Dieke, MPH, DrPH(c); Jimmy Koeninger, PhD;CAPT Robert Tosatto, RPh, MPH, MBATime: 1315-1430 hrsRoom: Delta CFocus Area: Leadership<strong>The</strong> next generation of medical, public health, preparedness, and responseleaders will emerge <strong>from</strong> today’s youth. It is essential that programs existto effectively engage, mentor, and develop youth now, so when the timecomes, they are ready to strengthen the local public health system, improveresponse capabilities, and build community resiliency. Youth engagement is akey component of succession planning. <strong>The</strong> Division of the Civilian VolunteerMedical Reserve Corps (DCVMRC), the U.S. Public Health Service (PHS)and HOSA–Future Health Professionals have established a close workingrelationship in order to further youth engagement and to foster mentoringand youth development opportunities. HOSA is a national organization thatprovides a unique program of leadership development, motivation, andrecognition for health science education students and serves as a modelof how students can engage in public health and preparedness volunteeractivities. Recent research for a doctoral thesis was conducted to explore thechallenges and benefits that an MRC unit may experience when engaginghigh-school-age youth. <strong>The</strong> investigator, along with leaders <strong>from</strong> HOSA, PHS,and DCVMRC, will highlight the importance of youth engagement, identifysome challenges regarding youth involvement, and lead discussion aboutways to overcome the barriers. Real-life examples of how HOSA, PHS, andMRC have partnered to provide opportunities for students will be presented.Learning Objectives:u Describe the importance of youth engagement as a component ofsuccession planning.u Discuss potential barriers to youth engagement and involvement, andidentify ways to overcome the barriers.u Explain opportunities to engage youth in public health, preparedness,and response activities.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinariansSession 16: <strong>The</strong> New Normal? Managing the Rise ofIncivility in Today’s DeploymentPresenter: Dennis Michael Baker, MA, LPCTime: 1315-1430 hrsRoom: Delta DFocus Area: LeadershipCivility is fundamental in any business, including disaster response. Peopletend to do business with those who grant them respect and make themfeel good. Similarly, civility among disaster team members fosters smoothrelationships within the team, promoting harmony and goodwill. When40civility is absent, team relations are strained. Rude treatment can makemembers unhappy, leading to cynicism, aggressive behavior, higher teammember turnover, lower team performance, and team conflict. Uncivilbehavior makes the deployment unpleasant, and it can negatively affecta team’s primary mission. When we are deployed, we sense it before wecan name it. Your team commander rolls his eyes, then sighs, “I alreadytold you what I wanted”; your team partner feigns deafness to your pleasto turn down her radio; a colleague ignores your emails and dodgesyour calls regarding progress on an important project. <strong>The</strong>se otherwiseeveryday interpersonal exchanges become conspicuous and memorableto us. <strong>Through</strong> other people’s body language, facial expressions, actions,omissions, mindlessness, and apparently demeaning remarks, we sizeup the interaction and feel diminished. We absorb these cues throughsituations and behaviors embedded in very narrow slices of our deploymentexperiences. We recognize in an instant a phenomenon called incivility.Given the speed, frequency, and complexity of deployment interactions intoday’s high-tech and global world, behavior has more nuances. Simply put,there are many more ways to show disregard for fellow team members.While much has been written about the hardships of deployment, it is oftenthe subtle things about the deployment that take the biggest toll. Cautionarytales <strong>from</strong> past events will be discussed to highlight “best practices” forimplementing corrective actions. This “New Normal?” session offers practicaland simple solutions to common errors in team interactions, leadership, andcommunication. When disaster strikes and teams are sent, we want to becertain we are sending the right message to our personnel. This session usesevidence-based practices to show you how to develop civility within yourteam structure and offer clear behavioral directives to your personnel.Learning Objectives:u Cite several examples of incivility that occur on deployment anddescribe how these incivilities hamper mission goals.u Identify low-intensity, discourteous behaviors that occur ondeployment and their effects on team performance.u Cite several examples of behaviors that leaders and team memberscan deploy to improve civility within a team structure.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinariansSession 17: 36-Hour Exercise, Ventura’s Story:Operation Medical Shelter 2011Presenters: CDR Patrick Denis, MBA, RN; Barry Fisher, MA, BA;Norm Plott; Chris RosaTime: 1315-1430 hrsRoom: Governor’s AEFocus Area: Public HealthThis session will provide concepts <strong>from</strong> the national health security strategypractically applied in a field setting. <strong>The</strong> logistics related to medical surge areevaluated by integrating hospitals into the field environment. This ongoingannual exercise requires significant coordination with numerous operational<strong>2012</strong> Integrated Training Summit
wednesday, May 23, <strong>2012</strong>Session Descriptionsarea partners, which ultimately results in increased community resilience.Previous after-action reports identified the need for increased coordinationamong emergency response groups. <strong>The</strong> presenters developed aninterdisciplinary response exercise with the goal of integrating professionalresponders as mentors to volunteers in ICS positions to manage the exercise.This served to demonstrate the resourcefulness of our operational areahealthcare system. <strong>The</strong> session will examine the practical components ofa robust 36-hour sustained exercise that demonstrated the involvementof multiple response partners (“silos”—aka “cylinders of excellence!”),including public health, fire, EMS, hospitals, military, law enforcement,medical reserve corps units, American Red Cross, and animal control. <strong>The</strong>execution of this type of exercise requires the public health responder towork in a “boots on the ground” scenario with volunteers and professionalresponders in a field setting.Learning Objectives:u Apply ideas and concepts in creating HSEEP-compliant exercises tobuild resiliency in the community.u Describe the practical components and specialized features of anintegrated 36-hour sustained exercise as a force multiplier.u Analyze methods utilized to integrate professional responders asmentors to staff and MRC volunteers in ICS positions to manage theexercise.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, nurses, pharmacists, physicians,social workers, veterinariansSession 18: Heat Emergency Response Plans andImplementationPresenters: Carl Adrianopoli, PhD, MS; Joseph H. Annelli, MS, EMT-B,BS; Paul A. Biedrzycki, MPH, MBA,CIHTime: 1315-1430 hrsRoom: Bayou ABFocus Area: Public HealthThis session highlights the importance of planning for heat-related morbidityand mortality during extreme heat events (EHE), which can result in moremortality and morbidity than all other natural hazards combined, includingcatastrophic flooding, tornadoes, and hurricanes. A snapshot review ofMaryland’s local health department’s plans and protocols revealed thatthere is little consensus on who should be responsible for heat planning andwhether heat planning efforts are even necessary. <strong>The</strong> review prompted theMaryland Department of Health and Mental Hygiene (DHMH) to developthe State Heat Emergency Plan in 2011 to provide planning guidance onpossible steps at the state and local level to prevent heat-related morbidityand mortality. <strong>The</strong> emergency plan guides DHMH’s actions during anextreme heat event, defined in the plan as a day when the heat index isexpected to reach 105ºF or the ambient temperature is expected to exceed100ºF. During these events, DHMH would issue a heat advisory to notifystate and local partners of the potential dangers associated with extremeheat events. <strong>The</strong> plan provides guidance for local health departments(LHDs) by providing suggested actions and public messaging resources.Weekly reports with information on temperature, emergency departmentvisits, deaths, and demographics were issued to provide locals with datato refine their planning efforts. Included in the planning efforts was a stateheat-related illness website, which provided public messaging with basicinformation on how individuals can be protected <strong>from</strong> the heat, links toadditional materials, contact information for local health departments,and weekly surveillance reports. This session is designed to share DHMH’sbest practices in developing a statewide plan and providing the necessaryguidance to a diverse mix of jurisdictions with different needs. We willexplore the various heat planning efforts at the local level, ranging <strong>from</strong>public education campaigns to jurisdictional heat emergency declarationsand sheltering programs. In addition, the issues presented will be highlightedwith a case study of a field trip that resulted in heat-related morbidity duringan extreme heat event. <strong>The</strong> session will conclude with the lessons learned,best practices, and issues raised during the 2011 extreme heat season.Learning Objectives:u State an understanding of the role of public health in a heat emergency.u Explain the development and composition of extreme heat eventresponse plans.u Identify partners for heat planning to address outreach, provide coolenvironments, and supply water to at-risk populations.u Describe urban heat island factors and how they affect extreme heatevents.u Discuss the types of communities that are most vulnerable to extremeheat events, and how to mitigate the resulting mortalityand morbidity.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, nurses, pharmacists, physicians,social workersSession 19: Veterinary Resources: First Aid forNon-Vets and Disaster Animal HealthPresenters: Marie Kerl, DVM, MPH, BS; R. Douglas Meckes, DVMTime: 1315-1430 hrsRoom: Governor’s C<strong>2012</strong> Integrated Training Summit 41session Descriptions
wednesday, May 23, <strong>2012</strong>Session Descriptionssession DescriptionsFocus Area: Resource Management and Patient MovementWorking dogs are likely to respond early in a disaster, before the deploymentand arrival of veterinary personnel. This talk will provide a review of basicfirst aid and medical care for working dogs utilizing supplies <strong>from</strong> a basichuman medical cache or first aid kit, and also discuss aspects of the handlerdogrelationship. Target audience for this session will be EMT/ paramedics,physicians, nurses, and other allied healthcare responders.Canine resources have been used to search for missing people in varioustypes of search and rescue responses. This session will describe thecapabilities, skills, and certification credentials of Federal EmergencyManagement Agency (FEMA) Urban Search and Rescue (USAR) teams—thecanine search specialists and their canines—and explain how to best utilizethis specialized canine resource on a search mission. A description of casestudies of actual searches and lessons learned will be included.Learning Objectives:u Describe similarities and differences in human and veterinary first aid.u Explain the role of FEMA USAR canines.u Identify early-onset medical conditions and environmental injuries forwhich field care can be initiated.u Describe FEMA USAR canine abilities and appropriate use of FEMAUSAR canines in a disaster situation.u Recognize partnerships that can be formed with the handlers, dogowners, medical personnel, and veterinary responders.Intended Audience: Dentists, emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, medical administrators, nurses, physicians, veterinariansSession 20: Hurricanes, Earthquakes, and Patients...OH MY! A Peek behind the USTRANSCOM CurtainPresenters: Lisa DeDecker, MS; Lt Col Heidi Hastings, FACHETime: 1315-1430 hrsRoom: Governor’s DFocus Area: Resource Management and Patient Movement<strong>The</strong> United States Transportation Command (USTRANSCOM), a combatantcommand of the Department of Defense, is the sole provider of patientmovement in support of Defense Support of Civil Authorities (DSCA). Thissession will outline the Joint Patient Movement Team (JMPT) and JointPatient Reporting Team (JPRT), who facilitate patient movement during DSCAresponse efforts. Unlike a no-notice event, pre-hurricane patient movementrequires a certain lead time for success. <strong>The</strong> use of pre-scripted missionassignments (PSMAs) and the critical timeline for DOD involvement will bedelineated. <strong>Through</strong>out this session, success stories and lessons learned<strong>from</strong> exercises and real-world events such as Operation Unified Response(Haiti) will be discussed. As planning has evolved over the past three yearsfor events such as those described in the National Response Plan, twocritical elements have been identified: the increased reliance on a strongDOD/DHHS partnership and the need for compatible information systems.<strong>The</strong> DOD/DHHS partnership of the Disaster Aeromedical Staging Facility(DASF) with the Mobile Acute Care Strike Team (MAC-ST) will be highlighted.42Technological advances in data capture and transfer could benefit patientmovement in the DSCA environment. An example of this would be theexpanding use of the Joint Patient Assessment and Tracking System (JPATS).<strong>The</strong> new disaster patient movement request forms will be demonstrated andfeedback requested. Annual interagency training opportunities are beingprojected and standardized training plans are being developed.Learning Objectives:u Describe the timelines required and capabilities for a DOD DSCAresponse.u Analyze the cooperative DASF/MAC-ST initiative between DOD andHHS.u Compare the DOD and DHHS patient tracking systems used duringpatient movement.u Illustrate required training needed for DSCA patient staging andevacuation.Intended Audience: Certified counselors, emergency physicians, EMT/paramedics, healthcare executives, health education specialists , marriage& family therapists, medical administrators, nurses, physicians, socialworkersSession 21: A Military and Public Health Joint TrainingModel that CaresPresenters: Charles R. Bauer, MD, CPE, FACS; CAPT Sean Boyd, MPH;CAPT Steven Hirschfeld, MD, PhD; Brian Smith, MD, MPHTime: 1315-1430 hrsRoom: Delta BFocus Area: Response Integration/Operational Medicine<strong>The</strong> United States Public Health Service (USPHS) Commissioned Corpsparticipated in Operation Lone Star (OLS), a joint services exercise toprovide medical care to the underserved community in South Texas. <strong>The</strong>experience required integration of three USPHS response teams with theTexas State Guard (TXSG), members of the Texas National Guard (TXNG),and the Texas Department of State Health Services (DSHS). <strong>The</strong> resultsof this fully integrated, local, state, and Federal mission for patient careand disaster preparedness, including potential future deployments, willbe the focus of this session. This exercise provided a unique opportunityto implement a new deployment model for PHS, which involved dividingassets into multiple operational sites, coordinating efforts with state andlocal responders, integrating mental health and social services, and lookingat new ways of collecting and analyzing data. Clinical teams developeda framework and tools whereby clients could become empowered tobecome active in the management of their own healthcare. Services includeimmunizations, preschool physical exams and screening, treatment, andeducation for general medical conditions plus hearing, vision, behavioralhealth, and dental care. A navigator-based system was implemented toprovide permission, education, and tools so that people left the site withan understanding of their health status in several dimensions, includingphysical, mental, emotional, dietary, and safety. Teams provided attentionand focus on the individual and family to plan for health improvement.USPHS and Texas epidemiologists and preventive medicine professionals<strong>2012</strong> Integrated Training Summit
wednesday, May 23, <strong>2012</strong>Session Descriptionsteamed together to collect unique data <strong>from</strong> Operation Lone Star. One armof the epidemiological data collection included a household survey, designedspecifically for the OLS clinic, addressing client characteristics, evacuationpreparedness, immunizations, and OLS marketing efforts. Additionalindividual client data were collected <strong>from</strong> medical charts, including age,gender, height, weight, BMI, and chronic medical history. <strong>The</strong> data analysiswill assist OLS and DSHS in targeting future public health interventions tooptimize impact.Learning Objectives:u Explain the structure and function of USPHS medical response teams.u Develop deployment plans for an integrated disaster response orhumanitarian mission.u Describe lessons learned to integrate response among Federal, state,and military assets supporting Operation Lone Star.u List and present suggested remedies for multiple potential problemsencountered during planning, deploying, performing duties, andreturn to station.u Identify best practices that can be applied as a new response modelfor the future.Intended Audience: Dentists, emergency physicians, EMT/paramedics, healthcare executives, health education specialists, medicaladministrators, nurses, physiciansSession 22: <strong>The</strong> HHS Disaster Behavioral HealthCONOPS: Optimizing Public Health and MedicalResponse and <strong>Recovery</strong> for Survivors and RespondersPresenters: Darrin Donato, BA; Rachel Kaul, LCSW, CTS;A. Thomas Mignone, Jr, MPH, REHSTime: 1315-1430 hrsRoom: Governor’s BFocus Area: Response Integration/Operational MedicineDisaster behavioral health is an integral part of the overall public health andmedical preparedness, response, and recovery system. It includes the manyinterconnected psychological, emotional, cognitive, developmental, andsocial influences on behavior, mental health, and substance use/abuse, andthe effect of these influences on preparedness, response, and recovery <strong>from</strong>disasters or traumatic events. Historically, the coordination and effectiveintegration of numerous and diverse behavioral health stakeholders andproviders into the larger health and medical response has been a challengeat Federal, state, and local levels. In December 2010, the Office of theAssistant Secretary for <strong>Preparedness</strong> and Response (ASPR) within the U.S.Department of Health and Human Services (HHS) initiated the HHS DisasterBehavioral Health Concept of Operations (DBH CONOPS) Working Group.<strong>The</strong> working group was comprised of agency representatives across HHSand aimed to develop a CONOPS to provide coordination and guidancefor HHS Federal-level behavioral health preparedness, response, andrecovery action for disasters and public health emergencies. Developmentof a DBH CONOPS is a recommendation of both the National BiodefenseScience Board and the National Commission on Children and Disasters.Effective and well-coordinated behavioral health preparedness, response,and recovery can mitigate or prevent more serious behavioral healthproblems in disaster survivors and responders and promote individual andcommunity resilience. <strong>The</strong> DBH CONOPS describes the overarching conceptualframework that HHS uses to coordinate HHS-wide preparedness, response,and recovery activities in concert with its authorities and responsibilities.<strong>The</strong> goal of the DBH CONOPS is to improve coordination of departmentalpreparedness, response, and recovery efforts concerning behavioral healthin support of state, territorial, tribal, and local efforts in a manner consistentwith the National Response Framework and the National Disaster <strong>Recovery</strong>Framework. Facilitated discussion about state and local response andrecovery activities and how these are supported through the DBH CONOPSwill also be a focus of the session. This interactive session will allowparticipants with and without behavioral health expertise to considerhow disaster behavioral health preparedness efforts can support existingoperational guidance at the Federal level and can enhance and informoverall emergency response and recovery at Federal, state, and local levels.Learning Objectives:u Identify the most common evidence-informed disaster behavioralhealth activities and interventions used to support survivors andresponders at the Federal, state, and local levels.u Describe the key elements of the Disaster Behavioral Health CONOPSand identify key roles and responsibilities of HHS operating and staffdivisions in disaster behavioral health response and recovery.u Discuss how the content of the Disaster Behavioral Health CONOPScan inform and optimize overall public health and medical responseand recovery <strong>from</strong> disasters and public health emergencies.Intended Audience: Certified counselors, emergency physicians, EMT/paramedics, healthcare executives, health education specialists, marriage& family therapists, medical administrators, nurses, physicians, socialworkersSession 23: Responder Risk in Crisis Standards of CarePresenters: Dan Hanfling, MD, FACEP; CAPT Kenneth Harman, MD;Fred Henretig, MD; Merritt Schreiber, PhDTime: 1515-1645 hrsRoom: Delta BFocus Area: Joint SessionRecently, the Institute of Medicine (IOM) released reports andrecommendations on implementing crisis standards of care (CSC) in healthemergencies. One cross-cutting component of the IOM recommendationsis the need to address the impact of implementing CSC on healthcareworkers. Although many healthcare workers confront life and deathdecisions on a daily basis, the nature of crisis standards of care involvesfundamental differences in both the qualitative and quantitative aspectsof many healthcare stressors. Consequently, the IOM Committee on CrisisStandards of Care has developed a number of key force health protectionactions involving leadership of diverse healthcare systems and healthcareworkers themselves. <strong>The</strong> recommendations will be presented and reviewedby several members of the IOM CSC, including the primary developer of theforce mental health protection recommendations.session Descriptions<strong>2012</strong> Integrated Training Summit 43
wednesday, May 23, <strong>2012</strong>Session Descriptionssession DescriptionsLearning Objectives:u Identify the potential range of mental health risks in crisis standards ofcare.u Review recent real-world events involving the need to implement crisisstandards of care.u Explain the IOM CSC recommendations to enhance resilience inhealthcare workers via key leadership actions of healthcare systems.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, pharmacists,physicians, respiratory therapists, social workers, veterinariansSession 24: Developing Guidance to Support Allocationby HHS of Scarce Federal Resources in DisasterSettings: An Opportunity for Stakeholder InputPresenters: Marion Danis, MD; Cynthia Hansen, MD, MPH;RADM Ann R. Knebel, RN, DNSc, FAANTime: 1515-1645 hrsRoom: Delta DFocus Area: Joint SessionHealth and Human Services (HHS) is developing guidance to assist with itsdecisions about allocation of resources in disaster settings. <strong>The</strong> intent of thisguidance is to offer key decision makers (1) a set of fundamental ethicalprinciples and values to consider when making decisions about allocation ofscarce Federal resources, and (2) a set of evaluation criteria that are ethicallyappropriate for considering specific allocation decisions. HHS is committed todeveloping and clearly communicating Federal resource allocation processesand criteria in advance of a disaster. To that end, HHS is seeking individualinput <strong>from</strong> stakeholders regarding the fundamental ethical principlesand values and the allocation criteria that HHS is developing to guide itsdecisions about allocation of resources in disaster settings. This session willprovide an opportunity for stakeholders attending the Summit (e.g., local,state, regional, tribal, and territorial) to review, evaluate, and rate proposedallocation criteria. An overview of the initiative to date, including backgroundon draft criteria, will commence the session. Various disaster scenarios willthen be presented to set the context for participants to think through issuesthat may be faced related to the decision-making process for allocation.Participants will then have an opportunity to provide stakeholder input onthe proposed criteria. Participants will engage in discussions regarding thescenarios and rating the criteria. A re-rating process will follow the discussionto aid in a final assessment of the proposed criteria. This stakeholder inputwill be considered as HHS finalizes guidance to support decision makingrelated to the allocation of scarce Federal resources in disaster settings.Learning Objectives:u Discuss the possible resource limitations that may be faced inallocating Federal resources during emergencies.u Identify various ethical values that might be appropriate for fairallocation of limited Federal resources.u Compare the relevant perspectives regarding criteria for distributinglimited Federal resources to states in emergency situations.Intended Audience: Certified counselors, emergency physicians,EMT/paramedics, healthcare executives, health education specialists,marriage & family therapists, medical administrators, nurses, physicians,psychologists, social workersSession 25: Implications of New InternationalAgreements on Public Health <strong>Preparedness</strong> andResponsePresenters: Nigel Lightfoot, MSc, FRCPath, FFPH; Maria JuliaMarinissen, PhD; <strong>The</strong>resa Wing Sze Tam, MBBS (UK), FRCPCTime: 1515-1645 hrsRoom: Delta CFocus Area: Joint SessionIn the past year, several new international commitments have beenundertaken by the U.S. and Canadian governments. Among them are theNorth American Plan for Animal and Pandemic Influenza (NAPAPI), releasedin November <strong>2012</strong> by the prime minister of Canada and the presidents ofMexico and the United States. Additionally, Canada and the United Stateshave come to agreement on the implementation plan and steps for theBeyond the Border Agreement. <strong>The</strong> panel session will first highlight whythese two agreements are so important for both countries and then sharewith participants the actionable steps that both countries have agreed totake.Learning Objectives:u Describe an understanding of the NAPAPI and Beyond the Borderagreements.u Analyze how international agreements strengthen domestic resiliency.u Demonstrate knowledge of the complexity of putting together andcarrying out binational plans to increase medical and public healthpreparedness and response activities.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinarians44<strong>2012</strong> Integrated Training Summit
Thursday, May 24, <strong>2012</strong>Session DescriptionsThursday, May 24, <strong>2012</strong>Session 26: Ethics of Altered Standards of Care in aDisaster ResponsePresenters: John Donohue, BS EMT-P; Andy Garrett, MD, MPH;Margaret Moon, MD, MPH; CDR Paul Reed, MD;Mardrah Starks-Robinson, MPA, BATime: 0830-0945 hrsRoom: Delta A BallroomFocus Area: General SessionDisasters are characterized by an overwhelming imbalance between needsand resources. In the face of this imbalance, difficult decisions aboutallocation of resources have to be made and implemented by policy makers,public health officials, and clinicians caring for victims at the bedside. <strong>The</strong>sedecisions have important ethical content and can generate tremendousmoral distress. We do not, however, have a clear and coherent frameworkto guide ethical decision making in the setting of acute disasters. Thissession will include an overview of important ethical challenges in disasterresponse and discuss work on the development of a framework that canhelp responders and policy makers avoid the most recognizable mistakes.Case studies will be used to gather audience input and comment <strong>from</strong> apanel of response experts.Learning Objectives:u Discuss some of the typical ethical dilemmas that occur in the wake ofa disaster, including the implications of triage and bedside rationing.u Explain how advance preparation and discussion may mitigate moraldistress during a disaster.u Describe a set of ethical principles that could help to shape decisionmaking in disasters.Intended Audience: Dentists, emergency physicians, EMT/paramedics,environmental health personnel, healthcare executives, health educationspecialists, industrial hygienists, medical administrators, nurses,pharmacists, physicians, respiratory therapistsSession 27: Successful Strategies in VolunteerIntegrationPresenters: Cheryl Schmidt, PhD, RN, CNE; Janice Springer, BSN, MAOL;Sharon Stanley, PhD, RN; Debra Wagner, CVA, NREMTTime: 1015-1130 hrsRoom: Bayou CDFocus Area: Healthcare SystemsVolunteers can be critical to a successful public health response, bututilizing them effectively in a way that is beneficial to everyone can be achallenge. Placing volunteers in healthcare or public health responsesettings requires attention to credentialing, training, and clinical skills. Inaddition, effective volunteer managers must not only fill positions to be suretasks are completed, but also meet the needs of the volunteers in terms ofmotivation and recognition. This session will explore potential barriers tointegration and provide examples of innovative strategies that have workedwell, including integration of veterinary and mental health volunteers.Learning Objectives:u Discuss current trends in volunteerism, and describe elements ofvolunteer program management.u Cite specific examples of how to successfully engage volunteers inspecific settings.u Identify common obstacles to volunteer integration and discussstrategies to overcome them.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, nurses, physicians, respiratorytherapists, social workers, veterinariansSession 28: Veterans Health Administration Officeof Emergency Management (VHAOEM) PerformanceImprovement Management SystemPresenters: Mary Connelly, BS; Jeanne M. McBride, MS, BS;Bonnie McGuffin, MSTime: 1015-1130 hrsRoom: Bayou EFocus Area: Healthcare SystemsIt’s time-consuming and costly to develop exercises that test specificcapabilities, provide consistent evaluation criteria, ensure compliance withmultiple requirements, and systematically identify corrective actions, not tomention the need to effectively develop and manage improvement plans.This session will demonstrate the web-based Performance ImprovementManagement System (PIMS) used by the Veterans Health Administration(VHA) to systematically plan, develop, and evaluate emergency exercisesand drills and to manage both single-year and multiyear improvement plans(IPs) for healthcare systems. Actual events and incidents may also be enteredinto the system to evaluate event response and develop corrective actionsand IPs. <strong>The</strong> system provides a consistent, efficient, and cost-effectiveapproach to ongoing performance improvement throughout the VHA andenables multilevel participation and collaboration. PIMS integrates an EventScheduler, an Event Builder, and an After Action Report/Improvement Plan(AAR/IP) Builder with a robust Performance Improvement Database. EventScheduler centralizes all VHA exercise and event information; allows usersto share information on exercise planning and real response experiences;provides user-customized views of all VHA events; and generates alertsfor exercise planning team meetings and IP action items. Event Builderstandardizes exercise development; provides step-by-step guidance fordeveloping exercise documentation [e.g., Exercise Plan, Controller/EvaluatorHandbook, Timeline/MSEL, and Exercise Evaluation Guides (EEG)]; allowsmultiple hazard selection linked to predetermined Veteran Integrated ServiceNetwork and Veteran’s Administration Medical Center (VAMC) capabilities;links capabilities to the Joint Commission and National Fire ProtectionAssociation standards; and is consistent with the Homeland Security Exerciseand Evaluation Program (HSEEP). AAR/IP Builder systematically capturesstandardized EEG data; standardizes exercise and real incident AAR andIP development; includes TJC and NFPA standards; and easily incorporatesprevious IP action items that need to be re-exercised. It also enables VAMCssession Descriptions<strong>2012</strong> Integrated Training Summit 45
THURsday, May 24, <strong>2012</strong>Session Descriptionssession Descriptionsto demonstrate compliance with regulatory and oversight standards andcaptures and documents emergency preparedness strengths, areas forimprovement, and best practices.Learning Objectives:u Discuss the advantages of using a web-based automated performanceimprovement management system.u Identify three cost-effective processes included in the VHA PIMS.u Compare current processes used at the participant’s facility with thefeatures and functions demonstrated in the session.Intended Audience: Certified counselors, emergency physicians, EMT/paramedics, healthcare executives, health education specialists, industrialhygienists, marriage & family therapists, medical administrators, nurses,pharmacists, physicians, social workersSession 29: Likability and LeadershipPresenter: Lorie LiptakTime: 1015-1130 hrsRoom: Delta CFocus Area: LeadershipFrom as far back as we can remember, we are taught to make certain everyonelikes us and to do and say things to please others. After all, life is just onebig popularity contest, right? So it is not surprising that we tend to couplelikability with effective leadership. However, a leader’s job is not to build ateam of people who like and are committed to him or her, but to build a teamthat is committed to following him or her in the pursuit of accomplishing aparticular task. Likability lets us be champions for our cause, but can hindergood decision making and effectiveness as a leader. This session will helpparticipants understand the link between likability and effective leadershipand provide ideas for harnessing the power of likability.Learning Objectives:u Identify the traits of a likable person and an effective leader.u Explain the link between likability and effective leadership.u Describe how to develop the traits of likability to improve leadershipskills.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,physicians, social workers, veterinariansSession 30: Listen, Protect, ConnectPresenters: Merritt Schreiber, PhD; LT CDR Anthony Tranchita, PhD, MSTime: 1015-1130 hrsRoom: Delta DFocus Area: LeadershipListen, Protect, Connect (LPC) is a psychological first aid (PFA) model that wasdeveloped specifically for use by community members to enhance resilience.Listen, Protect and Connect uses only non-mental-health responders withversions that focus on children, parents, family, and the community. Thismodel, when used by responders, can build community resiliency forcommunity disaster victims and responder-to-responder peer support. Thisis a key component of the “Anticipate, Plan and Deter” Responder ResilienceSystem in use in Los Angeles County hospitals and clinics and in the Stateof Minnesota. In this course, participants will receive training on using theNeighbor to Neighbor/Responder version of the Listen, Protect, and ConnectPFA model. This session will also highlight the successful use of LPC PFA bythe U.S. Public Health Service Mental Health Team 2 and the adaptation ofLPC PFA for healthcare workers by Los Angeles County and the Los AngelesCounty Department of Public Health. This LPC PFA model can be foundat http://www.cdms.uci.edu/protect.pdf and http://www.ready.gov/sites/default/files/documents/files/LPC_N2N_508.pdf. By the end of this session,participants will be able to apply and use Listen, Protect and Connect PFAin their daily lives and in disaster response with patients, family members,and other responders.Learning Objectives:u Recite varied approaches to psychological first aid.u Explain the use of the Listen, Protect and Connect PFA model foremergency responsers.u Describe how the USPHS and Los Angeles County Departmentof Public Health and Emergency Medical Services Agency havesuccesfully applied LPC to real-world experiences.u Apply and use Listen, Protect and Connect psychological first aid.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, pharmacists,physicians, social workers, veterinariansSession 31: Animals and Nuclear Accidents:Lessons Learned <strong>from</strong> JapanPresenter: Richard Green, EdDTime: 1015-1130 hrsRoom: Governor’s AEFocus Area: Public Health<strong>The</strong> 9.0 earthquake off the Pacific coast of Tohoku occurred at 14:46 JSTon Friday, 11 March 2011. It was the most powerful known earthquake tohit Japan and one of the five most powerful earthquakes in the world. <strong>The</strong>earthquake triggered extremely destructive tsunami waves of up to 133 feetand in some cases traveling up to six miles inland. In addition to loss of lifeand destruction of infrastructure, the tsunami caused a number of nuclearaccidents, primarily the ongoing level 7 meltdowns at three reactors in theFukushima I Nuclear Power Plant complex and the associated evacuationzones affecting hundreds of thousands of residents. <strong>The</strong> Japanese NationalPolice Agency confirmed 15,790 deaths, 5,933 injured, and 4,056 peoplemissing across eighteen prefectures, as well as over 125,000 buildingsdamaged or destroyed. Residents within a 12-mile radius of the FukushimaI Nuclear Power Plant and a 6.2-mile radius of the Fukushima II NuclearPower Plant were evacuated. Unfortunately, those animals that could notbe carried were left behind. Literally tens of thousands of animals remained46<strong>2012</strong> Integrated Training Summit
THURsday, May 24, <strong>2012</strong>Session Descriptionsin the “no-go” zone. On 2–3 May, a group of radiation and animal rescueexperts <strong>from</strong> the United States and Japan convened to discuss the currentcrisis and develop steps to provide aid to animals inside the evacuationzone. <strong>The</strong> committee included representatives <strong>from</strong> the Japanese Ministry ofEnvironment, United States Department of Agriculture (USDA), United StatesArmy Veterinary Corps, veterinary and toxicology experts, academicians,and representatives <strong>from</strong> the International Fund for Animal Welfare. <strong>The</strong>goal of this session will be to present the response procedures and protocolsdeveloped during the Summit to monitor, evacuate, and treat animalscontaminated by radiation.Learning Objectives:u Discuss how to include animal decontamination protocols in trainingand response plans.u Apply recommendations and protocols <strong>from</strong> the Japan experience tothe participant’s comprehensive emergency management plans.u Develop protocols for recognizing safe levels of radiation whenworking with animals in or around nuclear evacuation zones.Intended Audience: Environmental health personnel, industrialhygienists, veterinariansSession 32: Cultural Components of ResponsePresenters: Debra Kreisberg, PhD, MA, BA; Guadalupe Pacheco Jr., MSWTime: 1015-1130 hrsRoom: Bayou ABFocus Area: Public Health<strong>The</strong> health sector in the United States is struggling to meet daily demandsfor service, particularly to underserved and marginalized populations.Disasters and mass casualty events exacerbate the existing strain on localhealth infrastructure. Currently, health disparities perpetuate conditions inwhich many people in need cannot access adequate healthcare, creatingdisparities that are magnified in the event of a disaster. Evidence indicatesthat diverse communities suffer disproportionately, in both physical andmental health, at every stage of a disaster. Understanding how socioculturalfactors affect the way people access healthcare systems and utilize resourcesinforms how hospitals and communities can prepare to address theseculturally-specific needs of vulnerable populations. This is fundamental to aresilient community and a sustainable health response system and must bethe foundation of public health preparedness and healthcare and hospitalresponse planning. Taken together, a robust, mixed-methods approach forcomprehensively incorporating marginalized and vulnerable populationsinto public health and hospital disaster planning is necessary, particularlyif offering a model that could promote integration between public health,hospitals, and emergency management. In addition, the implementationof culturally and linguistically appropriate services across the public health,medical, and emergency management aspects of disaster preparedness andresponse helps ensure the provision of quality emergency health services.Cultural and linguistic competency is thereby an important tool for addressingdisparities. <strong>Preparedness</strong> and response efforts should fit the varying culturalcontexts of their community. <strong>The</strong> session will demonstrate the HHS Office ofMinority Health’s Cultural Competency Curriculum for Disaster <strong>Preparedness</strong>and Crisis Response (DPCR) as an effective and adaptable learning tool forcultural competency and improving services to culturally and linguisticallydiverse populations. <strong>The</strong> DPCR is an accredited online continuing educationprogram that equips disaster personnel with the knowledge, awareness, andskills needed to provide emergency health services to diverse populations.Learning Objectives:u Examine the relevance and diversity of vulnerable populations.u Demonstrate the need for cultural and linguistically appropriateservices in disaster preparedness and crisis response.u Identify the cultural and linguistic competency concepts in disasterpreparedness and response.u Analyze common models and best practices for assessing socialvulnerability and evaluate the pros and cons of various approaches.u Discuss a video case study in terms of providing culturally andlinguistically appropriate services during a disaster.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,physicians, psychologists, social workersSession 33: Leveraging Health Information Exchangefor Disaster <strong>Preparedness</strong> and Response to ImprovePatient CarePresenters: Alison Banger, MPH; LT CDR Samuel Schaffzin, MPA;Christopher Sullivan, PhD, MATime: 1015-1130 hrsRoom: Governor’s CFocus Area: Resource Management and Patient MovementDisasters often cause the displacement of patients and providers who crossstate borders to seek safety. While people move, their medical records donot. This creates major problems in accessing and delivering ongoing healthcare. <strong>The</strong>refore, the need for integrated health information exchange, intimes of disaster and in its aftermath, is critical. In 2010, the SoutheastRegional HIT-HIE Collaboration (SERCH) initiated a Health InformationExchange (HIE) Disaster Planning Project. This project was conductedthrough the State Health Policy Consortium (SHPC), an activity of theOffice of the National Coordinator for Health Information Technology. <strong>The</strong>SHPC is funded by the Health Information Technology for Economic andClinical Health (HITECH) Act, enacted as part of the American <strong>Recovery</strong> andReinvestment Act of 2009. <strong>The</strong> primary goal of the project is to define aset of strategies for sharing health information data among the southeastand gulf states, including Alabama, Arkansas, Florida, Georgia, Louisiana,and Texas, during and following a declared disaster. <strong>The</strong> SERCH project isusing lessons <strong>from</strong> disasters such as Hurricane Katrina and more recentlythe tornadoes in Joplin, Missouri, and Tuscaloosa, Alabama, to develop astrategic plan to allow physicians and patients to access medical recordsfor healthcare treatment during and after a disaster. <strong>The</strong> SERCH team hasprepared a white paper that provides guidance and recommendationsto states who wish to understand how to integrate HIE and emergencypreparedness activities to improve patient care during a disaster. <strong>The</strong> whitepaper addresses both legal and technical issues pertaining to cross-border<strong>2012</strong> Integrated Training Summit 47session Descriptions
THURsday, May 24, <strong>2012</strong>Session Descriptionsexchange of medical records in the context of a disaster. It also proposesnew functions for the ESF#8 agencies to engage HIEs and other healthcaredata sources. During this session, members of the SERCH team will providean overview of the Health Information Exchange framework and how itapplies to disaster preparedness and response. <strong>The</strong>y will also discuss theDisaster Planning Project in detail and use the session as an opportunity togather ESF#8 stakeholder feedback and input on next steps.Learning Objectives:u Describe the special needs/vulnerable population.u Analyze the current triage systems and demonstrate new approaches.u Explain the rapid assessment tool for identifying level of care needsand how this can be used to identify resources needed.u Discuss an integrated approach and how to put it all together.session DescriptionsLearning Objectives:u Describe the general Health Information Exchange (HIE) frameworkand environment and how it applies to disaster preparedness andresponse activities.u Explore Emergency Support Function (ESF#8) approaches to seamlessinterstate response before, during, and in the aftermath of a declareddisaster and how these practices can facilitate HIE.u Identify potential overlap between ESF#8 response and HIE activitiesand how this can be leveraged to improve patient care.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,physicians, social workersSession 34: Triage, Evaluation, and Care of SpecialNeeds/Vulnerable Populations: Putting It All TogetherPresenters: CAPT Steven Hirschfeld, MD, PhD;LCDR Tiffany Moore RN, BSNTime: 1015-1130 hrsRoom: Governor’s DFocus Area: Resource Management and Patient Movement<strong>The</strong> care needs of clients entering a response care facility such as a Federalmedical station will have a direct impact on the resources required andthe resource allocation. During Hurricane Ike in 2008, a field medicalstation was opened to receive special needs medical evacuees <strong>from</strong> thehurricane evacuation zone. Upon arrival, evacuees were classified usingthe conventional triage system for acuity. Most were classified under theMinimal Needs–Green triage code. However, as the shelter populationgrew to include over 300 special needs/vulnerable population evacuees,this classification did not accurately represent the resources needed. <strong>The</strong>U.S. Public Health Service Rapid Deployment Force-1 developed and fieldtestedduring deployment a rapid screening tool to assign clients during thetriage process to one of the five Center for Medicare and Medicaid Servicescare categories. Once the level of care was identified, discharge planningwas then able to focus on the discharge and/or transfer of the higher levelof care patients and additional resources needed could be identified. <strong>The</strong>tool was validated using multiple assessors and was particularly valuable inallocating resources and prioritizing discharge planning. During this session,participants will be instructed on this new rapid assessment tool for use withspecial needs or vulnerable populations during situations when the level ofcare needs must be identified. <strong>The</strong> session will conclude with discussing anintegrated approach to this special population during disasters and how toput it all together.48Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,physicians, respiratory therapists, social workersSession 35: Health System Response to Rapid Restorationof Medical Services after the Joplin TornadoPresenters: Paul Carlton, Jr, MD, FACS; Glenn Mitchell, MD, MPHTime: 1015-1130 hrsRoom: Delta BFocus Area: Response Integration/Operational MedicineThis session will describe the health system response to the total destructionof its 348-bed general hospital in Joplin, Missouri, on May 22, 2011. Athree-phased approach to immediate restoration of hospital services,including inpatient and outpatient behavioral health services, will bedescribed, and the strengths and weaknesses of the approach taken will bediscussed. An improved scheme for rapid setup of full-service hospital andclinic facilities based on lessons learned will be presented with significanttime and overall cost savings in return to full-service healthcare delivery in asuperior operational structure.Learning Objectives:u Describe the health system–level response to the Joplin tornado’sdestruction of the hospital.u Describe the sequential response for reinstitution of hospital servicesin Joplin.u Apply lessons learned in providing temporary hospital facilities toother field situations.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,pharmacists, physicians, respiratory therapistsSession 36: Workforce Health ProtectionPresenters: Linda Cashion, RN; Joseph Cocciardi, PhD, MS, CSP;CAPT Timothy Davis, MD, MPH, USPHSTime: 1015-1130 hrsRoom: Governor’s BFocus Area: Response Integration/Operational Medicine<strong>The</strong> National Disaster Medical System (NDMS) responds to public healthevents of consequence both nationally and internationaly. Challengesfaced during 2011 deployments included safety issues related to ionizingradiation, extreme heat events experienced during multiple field trainingexercises, and health- and safety-related airborne exposures in theaftermath of flood response activities. Evolving missions, novel requests<strong>2012</strong> Integrated Training Summit
THURsday, May 24, <strong>2012</strong>Session Descriptions<strong>from</strong> U.S. Government agencies, and an ever-increasing and sophisticatedtalent pool among disaster healthcare responders added unique missionspreviously unconsidered. Novel assignments deployed in under 48 hoursincluded rail-transport medical teams, public health assessment teamsdeployed to wide areas, and the development and integration of safetyand health systems for oil cleanup workers. Subsequently, the health andsafety system has grown through response, learning that their protectivemeasures were captured within the products provided by the OperationalMedicine Program: the Hazard Evaluation Risk Assessment (HERA) tool, theHealth and Safety Plan (HASP) template, and various safety and healthrelatedprograms and operating procedures. This session examines eachof these unique hazards that presented during the NDMS 2011 responseseason. It describes the protocol identified to address them and examineshow these protocols are being institutionalized, with emphasis on rapidand light response capabilities. <strong>The</strong> Office of the Assistant Secretary for<strong>Preparedness</strong> and Response (ASPR)/NDMS protocols now include responderand environmental measurements and prescreening, retrospective exposureassessments, and integration of health and safety response assets personnel<strong>from</strong> other deployed agencies. Communication of these products andprocedures is now occurring electronically.Learning Objectives:u Identify special hazards associated with response to potentialradiological hazardous situations, thermal extremes, long-termdeployments, and long-term public health hazards.u Identify the special hazards associated with rapid and light NDMSdeployment activities.u Identify NDMS force protection programs and their components inplace to protect responders <strong>from</strong> the hazards of ionizing radiation,temperature extremes, and post-disaster public health hazards, inboth traditional and rapid deployment scenarios.u Explain the worker safety and health requirements that new faster,lighter, smaller, specialty response teams will create, as well asremedies.u Utilize and retrieve information <strong>from</strong> the NDMS Force Protection,Health and Safety E-Learning Site (online), and use the site to accessprotective measures.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,respiratory therapists, social workers, veterinariansSession 37: In the Line of Fire: How to Prepare for,Respond to, and Recover <strong>from</strong> a Shooting IncidentPresenters: Craig DeAtley, MSHSc; Mark Potter;Mitch Saruwatari, PhD, EMT, MPHTime: 1300-1415 hrsRoom: Bayou CDFocus Area: Healthcare SystemsOver the past few years, media reports regarding workplace violenceoccurring in healthcare facilities have become far too common. Forexample, within the last year, there have been shootings at hospitals inBaltimore and suburban Washington, DC, and in a long-term-care facilityin North Carolina. For many facilities, the risk of an active shooter incidenthas subsequently become a priority risk in their hazard vulnerability analysis(HVA). This requires an increased need for a carefully thought-out responseplan that is fully integrated within the various levels of the healthcare facilityas well as among area law enforcement professionals. This session will focuson planning considerations for an active shooter <strong>from</strong> three perspectives:law enforcement early recognition and response recommendations, hospitalemergency management concerns for preparing a response plan, andhealthcare community response issues for supporting a facility impacted bythis type of incident.Learning Objectives:u Discuss early recognition and de-escalation activities for reducing therisk of hospital-based workplace violence.u Cite specific response considerations once an active shooter incidentbecomes imminent.u Outline the issues an emergency manager faces in writing an activeshooter response plan.Intended Audience: Certified counselors, emergency physicians,EMT/paramedics, healthcare executives, health education specialists,nurses, marriage & family therapists, medical administrators, physicians,respiratory therapists, social workersSession 38: Identifying the Factors: Evacuation of theMedically DependentPresenters: Bill Halstead, MPA, CEM; Jeffrey Schlegelmilch, MPH, MEPTime: 1300-1415 hrsRoom: Bayou EFocus Area: Healthcare SystemsUnder a contract with the Federal Emergency Management Agency, YaleNew Haven Health Systems (YNHHS) Center for Emergency <strong>Preparedness</strong>and Healthcare Solutions (CEPHS) (www.ynhhs.org/chs) conductedextensive research into the evacuation and sheltering needs of the medicallydependent population. A medically dependent individual can be definedas a person requiring a caregiver, medications, or specialized medicalequipment to sustain life or quality of life. Based on this research, numerousissues were identified as affecting the decision to evacuate or shelter-inplacethis population. It is vital that state and local emergency managementofficials and agencies involved in disaster planning be capable of identifyingthese factors and their effect on the determination to evacuate or shelterthis population in place. Based on their ability to recognize and considerthese issues, planners may then weigh and include them when developingor updating state, county or local emergency management plans.Learning Objectives:u Explain the difference between a population with special needs andthose considered to be medically dependent.session Descriptions<strong>2012</strong> Integrated Training Summit 49
THURsday, May 24, <strong>2012</strong>Session Descriptions<strong>The</strong> infant, child, and adolescent are all parts of the vulnerable pediatricpopulation. Based upon anatomical, physiological, developmental,and psychosocial differences, the pediatric patient must be consideredseparately <strong>from</strong> adults in terms of disaster planning. Unique pediatric issuesof mitigation, preparedness, response, and recovery do exist. <strong>The</strong> mostchallenging is the proactive nature of mitigation. A key aspect of mitigationis identifying the pediatric population and its relationship to various hazards.Routinely, a hazard vulnerability analysis (HVA) is performed in a welldefinedcommunity. <strong>The</strong> community, in turn, is defined by key stakeholdersincluding, but not limited to, public safety and security, public works,public health, schools, colleges and universities, housing, utilities, healthcare providers, industry, service and religious organizations, and Federallyfunded local response initiatives. Other key elements to be consideredinclude geography, residential patterns, highways or other infrastructure,and climate. Once completed, the HVA will allow an institution to compilea list of potential hazards. Hospitals will then be able to prioritize planningefforts to deal with the top ten hazards and develop their preparednessefforts accordingly. However, children are a unique population, and there islittle evidence on how to perform a pediatric hazard vulnerability analysis(PHVA). This is quite concerning, especially since about 25% of the U.S.population fits into the pediatric age range. <strong>The</strong>refore, we applied basichazard vulnerability principles to develop a novel PHVA tool using a websessionDescriptionsu Explain the difference between a “no notice event” requiringevacuation or sheltering-in-place versus an “event with notice” and beable to provide examples.u List a minimum of five factors to consider when determining whetherto evacuate or shelter-in-place individuals with medical dependencies.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,pharmacists, physicians, respiratory therapists, social workersSession 39: A Training Primer: Leaders UsingOrganizational Building BlocksPresenter: Teddy Rogers, MSA, NREMT-PTime: 1300-1415 hrsRoom: Delta CFocus Area: LeadershipThis session will focus on the three primary pillars that support anyorganization and the three things a leader must be in order to successfullylead. All organizations are grounded in leadership, training, and resources.A great leader must be a servant, a teacher, and a vessel. Leadershipand training are inextricably interconnected and then blended into theorganization’s total resources, which of course include the people. Leadersand trainers are both in the “people business,” and a failure to thrive inthis arena will lead to dismal organizational performance, if not failure.Successful leaders and trainers place the resources of an organization intoan environment and mind-set that require creating expectations and thenmanaging those expectations. <strong>The</strong> actions of successful leaders and trainerscan be compared to heavy equipment as they may function as cranes,bulldozers, and tow trucks or a combination of all when leading and trainingtheir groups. <strong>The</strong> success or failure of an organization is a direct reflectionon the proper use of the three pillars, the three things, and the three actionsthat leaders and trainers must understand, be, and use.Learning Objectives:u Explain the concept of the three pillars of an organization.u Discuss the concept of the three things that a leader or trainermust be.u Explain the heavy equipment analogy to identify the three actions thata leader or trainer must use.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, morticians,nurses, marriage & family therapists, medical administrators, physicians,social workers, veterinariansSession 40: Integrating Your Team with <strong>The</strong>ir TeamPresenter: Tom Lawrence, NREMT-PTime: 1300-1415 hrsRoom: Delta DFocus Area: Leadership50<strong>The</strong>re are many occasions when a cohesive, well-practiced response teammust work uncomfortably close with a comparable team. Given humannature, combined with the fact that these teams are often made up ofsuper Type A personalities, the management skills of their leaders will beseverely tested. Experience in these situations may be the best teacher.This session will offer the lessons identified by a team leader who hasfrequently encountered this situation and has blended teams, had his teamsupplemented by others, and supplemented others with his own. <strong>The</strong> resultsdemonstrate that with careful coordination, mutual respect, and awarenessof the potential pitfalls these scenarios often present, successful integrationof efforts is not only possible but quite likely.Learning Objectives:u Describe two scenarios in which teams must be integrated.u Describe the challenges to the integration of a cohesive team intoanother.u Discuss three techniques for the integration of one team with another.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,psychologists, social workers, veterinariansSession 41: Performing a Pediatric Hazard VulnerabilityAnalysis Utilizing a Web-Based Interface: <strong>The</strong> ChicagoExperiencePresenter: Paul Severin, MD, FAAPTime: 1300-1415 hrsRoom: Governor’s AEFocus Area: Public Health<strong>2012</strong> Integrated Training Summit
THURsday, May 24, <strong>2012</strong>Session Descriptionsbased interface. <strong>The</strong> setting of our PHVA was the city of Chicago. <strong>The</strong>process details probability, risk, and preparedness for human, technological,and natural events that may occur within a hospital’s area of operationswith a focus on the pediatric population. <strong>Through</strong> a web-based interface,supplemental information and reference material assist subject matterexperts as they prepare their PHVA report. This process will step the usersthrough the PHVA, so at the conclusion they will have a digital, printabledocument containing the required PHVA tables. User-based profiles willallow specified users to initiate their individual reports, save their work, andreturn to update, review, and print their PHVA report as needed. Our majorgoal is to demonstrate the PHVA process and provide lessons learned.Learning Objectives:u Demonstrate the utility of geographic information systems whenperforming a pediatric hazard vulnerability analysis.u Implement a web-based approach to performing a hospital pediatrichazard vulnerability analysis.u Apply lessons learned when considering the performance of apediatric hazard vulnerability analysis.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,physicians, respiratory therapistsSession 42: Partnering between Tribal and Local PublicHealth <strong>Preparedness</strong> and ResponsePresenters: Jason Debronz, MA; Sandy Evans, MPH, RN;<strong>The</strong>rese Quinn, BA; Lee ShipmanTime: 1300-1415 hrsRoom: Bayou ABFocus Area: Public HealthPresenters will provide information about collaborative efforts in WashingtonState and Okeechobee County, Florida. <strong>The</strong> emergency management director<strong>from</strong> the Shoalwater Bay Indian tribe and the emergency managementoperations manager for the Seminole tribe of Florida will join the MedicalReserve Corps (MRC) coordinators <strong>from</strong> the Tulalip tribes and SnohomishCounty. Three members of the panel <strong>from</strong> Washington State will discusshow they have worked together on public health preparedness andresponse with a focus on participation in the regional healthcare coalitions.Healthcare coalitions are regional partnerships that work to improve ourability to meet the dramatically increased demand for medical care that isexpected during a major health emergency. Healthcare coalitions consist ofrepresentatives <strong>from</strong> public health, hospitals, tribal health clinics, healthcareproviders, emergency medical services, home health care, long-term care,mental health, MRC, and emergency management. <strong>The</strong> panel member <strong>from</strong>the Seminole tribe of Florida will discuss how the tribe has worked withlocal, state, and Federal agencies for emergency preparedness and responsebefore, during, and after any disaster. He will also discuss the relationshipthat was built with the Okeechobee Medical Reserve Corps during the H1N1pandemic. <strong>The</strong> sessions will focus on the collaboration between tribes,counties, city, and state entities with an emphasis through the work of theMRC. Audience members will be encouraged to share their challenges andsuccesses in similar efforts in their local community. <strong>The</strong> presenters willfacilitate a conversation to explore ways that tribal, county, city, and stateorganizations can work together to benefit public health preparedness andresponse.Learning Objectives:u Describe the importance of partnering between tribal, local, and statejurisdictions for public health preparedness.u Identify stragegies to jointly build resilience that will be successful forparticipants in the local community.u Examine the benefits to both tribal and local jurisdictions ofpartnership in public health preparedness.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, healthcare executives, health educationspecialists, marriage & family therapists, medical administrators, nurses,physicians, psychologists, social workersSession 43: Where the Public Is @: Or How I Learned toStop Worrying and Love Social MediaPresenter: James Garrow, MPHTime: 1300-1415 hrsRoom: Governor’s CFocus Area: Resource Management and Patient MovementCrisis communication today is a vastly different animal than it was just fiveyears ago. <strong>The</strong> average time it takes for a story to be picked up and splayedacross the media has shrunk <strong>from</strong> days to minutes. <strong>The</strong> very definitionof who is a member of the media has changed. Many government andhealthcare communicators are struggling to keep up with the changesand feeling overwhelmed by the greatly expanded demands placed ontheir office due to these “new media.” This session will feature a tour ofthe most important social media websites and allow for discussion of therelative benefits—and shortcomings—of each. Examples will be woventhroughout the session to give guidance on how, and how not to, integratesocial media into an agency’s or organization’s crisis communication plans.Special attention will be paid to satisfying those in an organization who areuncomfortable with using social media, and techniques for addressing thoseconcerns will be developed and provided. Specific considerations that willbe addressed include: policy, goals, and procedures development; precrisisand crisis messaging; tailoring messages for different audiences, especiallyvulnerable and underserved populations; opportunities to continue learningabout social media.Learning Objectives:u Describe the relative benefits and shortcomings of four social medianetworks and how each can be used before, during, and after a crisis.u Describe how to integrate social media into communications plans,policies, and procedures, with a special focus on liability concerns.u Describe two best practice examples that demonstrate how socialmedia can effectively reach and engage traditionally vulnerable andunderserved populations.session Descriptions<strong>2012</strong> Integrated Training Summit 51
THURsday, May 24, <strong>2012</strong>Session Descriptionssession DescriptionsIntended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinariansSession 44: Train as You Respond: Integration of MilitaryFirst Responders and the Forgotten HeroesPresenters: Akiko Berkman, MPH, MPA; MAJ Micah Goettl, BSTime: 1300-1415 hrsRoom: Governor’s DFocus Area: Resource Management and Patient MovementRecent history has shown repeatedly that during periods of crisis andnatural disasters the National Guard and civilian agencies are virtuallyalways involved and tend to work well together, even if impromptu.However, those of us in the domestic operations community realize thatalthough such impromptu relationships are essential, they are never goingto be able to fully develop a well planned and exercised relationship. <strong>The</strong>forgotten heroes during a domestic crisis are the civilian volunteers andnongovernmental agencies (NGOs). However, those personnel are typicallyan afterthought in developing relationships down on the ground level,especially during military exercises. In the military there is a saying “Trainas you fight.” To actually live up to that mantra, the military must continueto foster relationships with civilian volunteers and NGOs since that is theway we would fight in military support to domestic agencies. One of thenewest developing capabilities of the National Guard to start getting somegreater public awareness are the CBRNE Enhanced Response Force Package(CERFP) and Homeland Response Force (HRF). <strong>The</strong> medical capability ofthe CERFP and HRFs is certainly equivalent to the DMAT teams, which areone of the better known and capable medical response teams. However, inaddition to the DMAT teams, Medical Reserve Corps are capabilities thatwould certainly be available in a domestic crisis. Awareness alone does notbuild the relationships necessary; teams need to understand each other’scapabilities and deficiencies prior to a crisis in order to be successful. Inlocal, county, state, and national level exercises, there is always going tobe an opportunity to incorporate volunteer teams such as Medical ReserveCorps and NGOs to conduct side-by-side training. Understanding the natureof volunteer teams and organizations requires that planning be flexibleand creative with scenarios that will allow the participation of volunteerorganizations. Understanding legal limitations or requirements for bothcivilian volunteer teams and military personnel can also be used as aguideline when developing training and standard operating procedures. Inthis session we will explore the planning and implementation of a jointexercise that involved MRC/ESAR-VHP/American Red Cross and militarypartners and the lessons learned.Learning Objectives:u Explain the capabilities and limitations of National Guard firstresponders such as the CBRNE Enhanced Response Force Package(CERFP).u Evaluate and refine potential best practices for integration of NationalGuard first responders and Medical Reserve Corps volunteers duringdisaster responses.u Evaluate and refine best practices for integration of National Guardfirst responders and civilian healthcare providers at the pointof impact, including triage, stabilization, and patient trackingmechanisms.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, nurses,marriage & family therapists, medical administrators, physicians, socialworkersSession 45: Mass Fatality Event: Responding to theReno Air Race TragedyPresenters: Christina Conti, MPPA; Betsy Hambleton, BA;Aaron KennestonTime: 1300-1415 hrsRoom: Delta BFocus Area: Response Integration/Operational MedicineOn September 16, 2011, the National Championship Air Races and AirShow in Reno, Nevada, quickly transformed <strong>from</strong> a renowned air showinto a horrific war scene after veteran pilot Jimmy Leeward crashed hisvintage P-51 Mustang on the tarmac just feet away <strong>from</strong> the VIP box seats.Immediately, the Regional Emergency Medical Services Authority (REMSA)personnel, along with the Reno and Airport Authority Fire Departmentsand a host of volunteers, responded to the dozens of injured spectators.Within 62 minutes REMSA had transported 54 injured people to threearea hospitals. After REMSA’s transport was completed, the secondaryphase of the tragedy began. Although the injured were being treated athospitals, the tarmac resembled a war zone, with debris and human remainsscattered across the tarmac. Not only were there nearly a dozen fatalities,but the sudden and violent nature of the deaths completely shocked thespectators, responders, and everyone else at the scene throughout the first48 hours. <strong>The</strong> Washoe County Health District (WCHD) began its responseimmediately on Friday following the crash and became more involved asthe incident unfolded. Saturday morning, when the medical examiner askedfor support recovering remains <strong>from</strong> the tarmac, the Medical Reserve Corps(MRC) provided four medical volunteers to walk the tarmac and recoverremains. Additionally, another group of MRC volunteers worked with theUnified Victim Identification System (UVIS), inputting data to help identifythe recovered remains. This assistance expedited the medical examiner’stask of making positive identifications of the victims to bring familiesresolution. Based on the severity of the situation, the decision was made toopen a family assistance center (FAC) to obtain the UVIS information andto provide resource assistance to the families of the injured and missingwho were arriving in Reno. <strong>The</strong> Washoe County Public Health EmergencyResponse Coordinator, working with the Regional Emergency OperationsCenter, set up the FAC, which was operationally ready by 11 a.m. the dayfollowing the crash. Utilizing 10 mental health volunteers <strong>from</strong> the MRCalong with volunteers <strong>from</strong> supporting agencies, the FAC served 17 familiesimpacted by the event. In total, the WCHD worked with 19 other agenciesand organizations to support the overwhelmed medical infrastructure,providing services to the medical examiner, the victims’ families, the NationalTransportation and Safety Board, and the local community.52<strong>2012</strong> Integrated Training Summit
THURsday, May 24, <strong>2012</strong>Session DescriptionsLearning Objectives:u Describe the types of emergency response and medical infrastructureinvolved in a mass fatality event; identify their roles in the ICS UnifiedCommand System. Based on the acuity of a mass fatality event,forecast the types of services needed.u Explain the basic equipment and training needed for staff andvolunteers to meet the needs of essential agencies (MedicalExaminer’s Office, Airport Authority, local hospitals, call centers) aswell as serving the needs of the community.u Analyze the events and identify goals and objectives for a multifacetedmass fatality response plan.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workersSession 46: Animal Health Impacts on Human Responseand <strong>Recovery</strong> EffortsPresenters: Lori Gordon, DVM; Lisa Murphy, VMD, DABT;Charlotte Spires, DVM, MPH, DACVPMTime: 1300-1415 hrsRoom: Governor’s BFocus Area: Response Integration/Operational MedicineThis session will include discussion of a risk-based algorithm for decisionmaking in the disaster sheltering of special medical evacuees presentingwith their companion animals to a U.S. Health and Human Services Federalmedical station (FMS) established in College Station, Texas, in the wake ofHurricane Ike in 2008. <strong>The</strong> FMS was established at Texas A & M Universityand was managed by a USPHS Rapid Deployment Force 1 team of U.S.Public Health Service commissioned officers. Particular emphasis will beplaced on the special human-animal bond issues associated with individualswith special physical or mental health needs who seek disaster sheltering forthemselves and their pets. Many of these evacuees had lost beloved pets inprior evacuations due to their inability to control the management of theiranimals and a lack of physical, mental, and/or monetary resources to facilitatereturn of their animals to them at the conclusion of the evacuation.This session will also include information about the most common types ofinjuries and illnesses experienced by USAR dogs during deployment. <strong>The</strong>potential for injuries and illnesses is an important concern when personnelare deployed <strong>from</strong> the United States to respond to disasters in foreigncountries, particularly because of the unique challenges that exist withrespect to environmental and endemic hazards. <strong>The</strong> only disasters for whichthere are injury and illness data for FEMA USAR dogs was the OklahomaCity bombing of April 19, 1995, and the World Trade Center disaster ofSeptember 11, 2001. Little is known of injury or illness for deploymentsoutside the United States. <strong>The</strong> recent international responses in Haiti andJapan highlighted this problem, as well as the need for standard operatingprocedures, potential human health concerns for both response personnel andmembers of the general public who may come in contact with contaminatedanimals, and the current absence of trained animal decontamination teamsable to respond at local, state, Federal, and international levels.Learning Objectives:u Apply appropriate interaction of veterinarians, medical health, mentalhealth, and other public health professionals in the postdisastermanagement of high medical risk disaster evacuees who evacuatewith their companion animals.u Identify the injuries and illnesses experienced by the USAR dogs thatdeployed to Haiti following the earthquake of January 12, 2010.u Utilize a methodical approach to determining the best disastermanagement options for special medical needs disaster evacueeswho present with companion animals to which they are particularlybonded.u Utilize the injury and illness information to guide responders in what isneeded for deployment.u Discuss current resources and procedures for animal decontaminationand what is still needed.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, morticians,nurses, marriage & family therapists, medical administrators, physicians,social workers, veterinariansSession 47: Bioterrorism and the Emerging InfectiousDisease Threat: <strong>Preparedness</strong> and Response Are CriticalPresenter: Jerry Jaax, DVMTime: 1500-1630 hrsRoom: Delta BFocus Area: Joint Session<strong>The</strong> session will provide a fast-paced overview of the bioterrorist and emerginginfectious disease threat, addressing both public heath and agriculturalvulnerabilities. To characterize the threat and the daunting researchchallenges we face, the presenter will draw upon his extensive experiencein high-consequence pathogen research at U.S. Army Medical ResearchInstitute of Infectious Diseases (USAMRIID); biological arms control treatyand Trilateral Agreement compliance; and offensive biowarfare programcounterproliferation efforts in the former Soviet Union. <strong>The</strong> session will alsodescribe issues and challenges associated with updating critical researchinfrastructure in the United States by highlighting the recent selection ofManhattan, Kansas, as the replacement site for the Plum Island AnimalDisease Center with the $700 million National Bio and Agrodefense Facility.Additionally, the session will recount personal experiences and emergencyresponse lessons learned during the 1990 Reston Ebola outbreak, recountedin the #1 New York Times best seller <strong>The</strong> Hot Zone by Richard Preston.Learning Objectives:u Discuss bioterrorism and the challenges associated with adequateprevention and development of countermeasures and responsestrategies.session Descriptions<strong>2012</strong> Integrated Training Summit 53
THURsday, May 24, <strong>2012</strong>Session Descriptionssession Descriptionsu Explain lessons learned <strong>from</strong> an emergency response to the emergenceof the exotic Ebola virus in nonhuman primates in the United States.u Assess the dimensions of Cold War offensive biowarfare programs andtheir troubling legacy for today’s world.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, nurses, pharmacists, physicians,respiratory therapists, social workersSession 48: When Leadership Goes AskewPresenter: RADM Boris Lushniak, MD, MPHTime: 1500-1630 hrsRoom: Delta CFocus Area: Joint SessionLearning about leadership and the qualities inherent in a leader can stem<strong>from</strong> many sources, including (1) the observation of great leaders in action(role models) and, to some extent, the opposite extreme of dealing with“nonleaders” in leadership roles; (2) the personal lessons learned <strong>from</strong> beingplaced in leadership positions, and (3) good old-fashioned “book work”and reading about leadership. This session will emphasize ten qualities ofleadership that when lacking or inappropriately implemented would leadto leadership going askew. <strong>The</strong>se qualities are the following: (1) a leaderkeeps calm and cool; (2) a leader is a good communicator; (3) a leaderprovides perspective and context; (4) a leader makes decisions; (5) a leaderis adaptable; (6) a leader is a role model; (7) a leader sets a high ethicaltone; (8) a leader delegates appropriately; (9) a leader builds and supportsteamwork and cooperation; (10) a leader is positive, encouraging, andrealistically optimistic. Methods of dealing with leadership going askew willbe discussed in an open forum.Learning Objectives:u List five qualities of a leader.u Describe the 4 Ds of leadership.u List three examples of how to deal with leadership going askew.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,respiratory therapists, social workers, veterinariansSession 49: <strong>The</strong> Regional Sandbox ExperienceTime: 1500-1700 hrsRooms:Region 1Region 2Region 3Region 4Region 5Governor’s AEGovernor’s CGovernor’s BGovernor’s DDelta DRegion 6Region 7 & 8Region 9Region 10Focus Area: Joint SessionBayou ABBayou DBayou ECanal B<strong>The</strong>se regional meetings are intended to provide a forum for informationexchanges that will align and integrate regional players, and better informfuture planning and deployments. Each regional meeting will be uniquelyconstructed to encourage coordination between local, state and Federalparticipants and explore ways our agencies might work together. It will bean opportunity to reconnect with old teammates and meet new players.Friday, May 25, <strong>2012</strong>Session 50: <strong>The</strong> Joplin TornadoPresenters: Jason Henry, RN, EMT, BA; Robert Patterson; Leslie Porth,RN, BSN, MPH; Regina ThomasTime: 0830-0945 hrsRoom: Bayou CDFocus Area: Healthcare SystemsAt 5:41 p.m. on May 22, 2011, St. John’s–Mercy Hospital in Joplin, Missouri,took a direct hit <strong>from</strong> an EF-5 tornado. Immediate activation of a statewidehospital mutual aid agreement (MAA) enabled efficient and effectivehospital response prior to Federal declarations and state executive orders.<strong>The</strong> mutual aid agreement provided the framework for hospitals acrossMissouri to immediately respond with regional assets for communicationand medical surge while providing the structure and documentation neededfor Federal reimbursement. <strong>The</strong> tornado completely destroyed one hospital,requiring the evacuation of 183 patients within 90 minutes of impact.Emergency medical services <strong>from</strong> four states quickly responded to begintriage, treatment, and transport of patients and victims. <strong>The</strong> resulting surgeduring the next 12 hours at the neighboring hospital required treatment ofapproximately 500 patients in the emergency department; treatment andrelease of 400-600 patients in established triages; and the provision of about400 CT scans and 22 critical surgeries. <strong>The</strong> secondary location for patientand victim transport was about 75 miles away. Two acute care hospitalsin this community each received about 125 patients and victims throughvarious modes of transportation. <strong>The</strong> statewide approach to emergencypreparedness planning utilizing funds <strong>from</strong> the ASPR Hospital <strong>Preparedness</strong>Program and adopting the medical surge capability and capacity tierstructure provided the foundation for an effective response. However,despite an overall successful response, debriefings and after-action reportsidentify lessons learned and opportunities for improvement. This panelsession will focus primarily on the following lessons learned and subsequentplanning and preparedness policy changes: developing a chain-of-custodydocumentation system to accompany any resources provided through theMAA; developing a process, separate <strong>from</strong> technology and tools, to tag andtrack patients in a mass casualty event; procedures need to be developed fora back-up plan for receiving hospitals to initiate patient tracking to supportthe efforts of impacted hospitals; continuing to refine redundant systems for54<strong>2012</strong> Integrated Training Summit
THURsday, May 24, <strong>2012</strong>Session Descriptionscommunication to increase likelihood of tactical communication capabilitieswith massive infrastructure loss; continuing to refine mass casualty plans forsudden, catastrophic surge and basic field triage.Learning Objectives:u Summarize the regional hospital response through the statewidemutual aid agreement.u Identify specific lessons learned for managing an immediate surge oftrauma patients during a mass casualty event.u Identify specific lessons learned for managing patient identificationand tracking during a mass casualty event.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,physicians, respiratory therapistsSession 51: What Do You Mean “No Notice?”Presenters: Jonathan Ban, MA; Arthur Kellermann, MD; Gregg Margolis,PhD, NREMT-P; Christopher Nelson, PhDTime: 0830-0945 hrsRoom: Bayou EFocus Area: Healthcare SystemsNumerous challenges face hospitals preparing for disasters and public healthemergencies, including rampant emergency department (ED) crowding,routine “boarding” of admitted patients in ED, frequent diversions ofinbound ambulances, packed ICUs, and diminishing numbers of specialistswilling to take ED call. All of these issues have an effect on the surge abilityof a healthcare facility. While every healthcare facility needs to be able toincrease capacity quickly, the ability to do so is rarely quantified. <strong>The</strong> JointCommission requires hospitals to periodically conduct disaster drills, butthese events are usually scheduled and often highly choreographed. Thispreparation can provide a falsely reassuring view of surge capacity. As a result,healthcare organizations may be caught off guard during true emergencieswhen readily foreseeable bottlenecks compromise their ability to managea sudden influx of patients. To fill this gap, HHS/ASPR is collaborating withRAND Health to develop a no-notice assessment tool (including a scenarioand performance metrics) that hospitals and healthcare coalitions can useto assess their operational capability to surge in response to a mass casualtyincident. <strong>The</strong> overall goal is to create a simple and inexpensive assessmentthat can be used by a wide variety of hospitals on a regular basis to identifyoperational challenges and spur improvement. This session will present anoverview of the assessment tool, including its intent and key features, andprovide participants the opportunity to offer feedback to HHS on the design,use, and possible expansion of the tool.Learning Objectives:u Describe the challenges of measuring surge at the healthcareorganization level.u Discuss and weigh the advantages and disadvantages of a no-noticesurge assessment.u Construct improvements to the current draft of a hospital surgestress test.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,physicians, respiratory therapistsSession 52: Leadership: When It Counts the MostPresenter: CAPT Mark Libby, MSN, ARNPTime: 0830-0945 hrsRoom: Delta CFocus Area: LeadershipYou’ve been tapped to lead an urgent, large-scale disaster response to ahard-hit community across the country–or across the world. <strong>The</strong> missionis difficult; the consequences are high. You have just a few hours to turnhundreds of team members into an effective and cohesive high-speedorganization. Where do you start? This session will discuss strategies usedby ASPR regional emergency coordinators who lead the Federal medicalresponse in the field. How to “stand up” a command element, how to createand share a leadership presence and vision will also be discussed. Thissession will explore how to establish a shared mission culture that projectsintegrity, confidence, and competence and will look at the importantdifference between talking and doing in leaders who have the courage toact decisively. Finally, we will discuss the concept of “servant leadership”and how it empowers team commanders and responders to create the bestpossible outcomes for those in their care while still caring for their ownresponders.Learning Objectives:u Explain the differences between coordination, management,command, and leadership. What is the right approach to direct,motivate, or inspire?u Discuss how to lead when you’re not in charge.u Explore tools and techniques to coordinate leadership efforts acrossthe theater of operation and encourage leadership at all levels.u Discuss how to recover <strong>from</strong> challenges and setbacks, and how tocelebrate successes.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,respiratory therapists, social workers, veterinariansSession 53: Emergency Management DilemmaPresenter: CAPT Kenneth Harman, MDTime: 0830-0945 hrsRoom: Delta DFocus Area: LeadershipThis session will view emergency and disaster preparedness, response, andrecovery <strong>from</strong> a leadership perspective. It will argue that response is theleast important, least successful, and most expensive aspect of emergencymanagement and that preparedness and mitigation are the cornerstones ofa robust emergency management program. PREPAREDNESS: Emphasis willsession Descriptions<strong>2012</strong> Integrated Training Summit 55
FRIday, May 25, <strong>2012</strong>Session Descriptionssession Descriptionsbe placed on the critical role of preparedness and what leaders should bedoing at the community and regional level to facilitate resiliency. This willinclude the need for better public education that addresses historic andcultural bias about disaster and how these inaccurate perceptions positioncommunities for catastrophe. RESPONSE: Best leadership practices forresponse will focus on the presenter’s personal experiences. Emphasis willagain focus on response preparation and the realities of leadership duringcrisis. RECOVERY: <strong>The</strong> idea of viewing disaster as a cyclic and inevitableoccurrence will be introduced. From this perspective the opportunitiesassociated with recovery that positively affect community resiliency andpreparedness will be discussed.Learning Objectives:u Describe emergencies and disasters as a cyclic phenomenon withpredictable stages (event, response, recovery, preparation).u Explain why disasters are a social construct with roots in the culture,economics, and government of the affected community.u Discuss the negative consequences of limiting emergency and disasterleadership to response.u List the most effective leadership strategies for nurturing disasterresiliency within a community.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinariansSession 54: Five Feet High and Rising: <strong>The</strong> GaylordOpryland Response to the 2010 Tennessee FloodPresenter: Brian Abrahamson, BATime: 0830-0945 hrsRoom: Governor’s AEFocus Area: Public HealthOn May 3, 2010, the Music Valley neighborhood of Nashville, including theentire Opryland Hotel complex and its surrounding campus, was floodedwith 5 to 10 feet of water. <strong>The</strong> overflow of the Cumberland River, which isnow being recognized as a 1000-year flood, had jumped its banks after twodays of rain. Prior planning had identified the Opryland complex as a “not atrisk” location and a potential resource for the community. However, this wasnot the case and local, large-scale response challenges emerged. “Five FeetHigh and Rising” is a Johnny Cash song about flooding and the progressionof increased intensity. <strong>The</strong> Opryland Hotel needed to move 1500 guests toanother area and ensure their safety. This session will focus on the dynamicdecisions and the strategic response of the Gaylord Opryland staff. Beyondthe response, new ideas and planning concepts have been implementedbased on this firsthand experience.Learning Objectives:u Discuss the Gaylord Opryland response to the 2010 flood, both beforeand after the disaster.u Describe the lessons learned for evacuating a large hotel.56u Review the business end of hazard and risk mitigation.u Discuss the necessity of new local partnerships in large-scale disasters.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,social workers, veterinariansSession 55: U.S. EPA: A National to Local Look atHow Emergency Response and Cleanup Activities AreConductedPresenter: Steve Spurlin, BSTime: 0830-0945 hrsRoom: Bayou ABFocus Area: Public Health<strong>The</strong> U.S. Environmental Protection Agency (EPA) mission is to respond toimmediate threats <strong>from</strong> releases of hazardous substances and oil. <strong>The</strong> firstpriority is to eliminate any danger to the public. By the end of 2007, EPA hadconducted over 9,400 removal actions at more than 6,900 sites. Over thelast 40 years, the nature of the contaminants, the number of responses bypotentially responsible parties, and the capacity and capability of states havevaried. Each of EPA’s 10 regional offices has developed a strong emergencyresponse and removal program, tailored to work with and complement thevarying capabilities of local and state agencies for responding to the typesof oil and hazardous substances releases that occur in its region. Each EPAregion deals with a unique mix of industries, geography, and state and localresponse agencies. Still, the program acts as a Federal safety net to allow forresponse to immediate threats when such response is necessary (e.g., whenthe nature, size, or complexity of a spill is beyond the capacity or capabilitiesof the state or local responders). Each year, more than 20,000 emergenciesinvolving the release (or threatened release) of oil and hazardous substancesare reported in the United States, potentially affecting both communitiesand the surrounding natural environment. Emergencies range <strong>from</strong> smallscalespills to large events requiring prompt action and evacuation of nearbypopulations. EPA coordinates and implements a wide range of activities toensure that adequate and timely response measures are taken in communitiesaffected by hazardous substances and oil releases where state and localfirst responder capabilities have been exceeded or where additional supportis needed. EPA’s emergency response program responds to chemical, oil,biological, and radiological releases and large-scale national emergencies,including homeland security incidents. EPA conducts time-critical and nontime-criticalremoval actions when necessary to protect human health andthe environment by either funding response actions directly or overseeingand enforcing actions conducted by potentially responsible parties. <strong>The</strong>Stafford Act (PL-93-288) provides the authority for the Federal governmentto respond to disasters and emergencies in order to provide assistance tosave lives and protect public health, safety, and property.Learning Objectives:u Explain how EPA works with state, local, and tribal governments,along with other Federal agencies, who play a critical role inpreventing, preparing for, and responding to emergencies of all kinds.<strong>2012</strong> Integrated Training Summit
FRIday, May 25, <strong>2012</strong>Session Descriptionsu Discuss how the Stafford Act (PL-93-288) provides the authority forthe Federal government to respond to disasters and emergencies inorder to provide assistance to save lives and protect public health andsafety.u Recite an overview of the more than 20,000 emergencies involving therelease (or threatened release) of oil and hazardous substances thatare reported in the United States every year.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, pharmacists,physicians, social workersSession 56: Working Together! Integration ofVolunteers with ARC, MRC, and ESAR-VHP Partnersduring the Recent Hurricane ResponsesPresenters: Mary Casey-Lockyer, RN, BSN, MHS; Judy Homer, RN;Leigh Ann Scheider, BA, EMTTime: 0830-0945 hrsRoom: Governor’s CFocus Area: Resource Management and Patient MovementThis session will include local, state, and national perspectives of volunteerutilization in disaster events. <strong>The</strong>re will be a brief overview of the New YorkState event and Medical Reserve Corp/ Emergency System for AdvanceRegistration of Volunteer Health Professionals (MRC/ESAR-VHP) andAmerican Red Cross (ARC) involvement. Participants will be able to identifythe ServNY program/structure, the conditions that led up to the need forthe deployment of volunteers in the state, the state’s implementation ofthe response, the challenges and the lessons learned <strong>from</strong> the volunteerdeployment, and the changes that will need to be more successful for afuture deployment plan of operations. From the local perspective, presenterswill focus on the local response and how the local structures that are alreadyin place responded to and partnered with ARC and state involvement. <strong>The</strong>rewill also be information <strong>from</strong> the American Red Cross national health servicesoperations in general and the enhanced service delivery model (scope ofpractice) and functional needs support services. Presenters will focus onlessons learned and challenges such as type of storm, rolling event, start ofARC operations in New York City, and the public health role.Learning Objectives:u Describe the challenges of multi-level response and interagency andgovernmental partnerships.u Explain the ARC enhanced service delivery model (scope of practice)and functional needs support services and how they fit in with MRCand ESAR-VHP.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, marriage & family therapists,medical administrators, nurses, physicians, psychologists, social workersSession 57: “In the Eye of the Storm”: A Proven Systemof Safe, Integrated, Multiregional Patient EvacuationPresenters: DeAnne Seekins, MBA; Benita Stoddard, MHA, FACHE;Shedale Tindall, RN, MSNTime: 0830-0945 hrsRoom: Governor’s DFocus Area: Resource Management and Patient MovementThis session will identify a system of advanced preparation and coordinationfor safe evacuations of a Federal healthcare facility with a clinically complexpatient population. It will describe geographic challenges and provideexamples of integrated emergency management systems. <strong>The</strong> presenters willdiscuss recommendations for increasing resiliency and ensuring sufficientlogistical and clinical systems for shelter-in-place versus evacuation. Patientsafety protocols will be examined for shelter-in-place and evacuation of acutepsychiatry, chronic spinal cord injury, palliative care, and homeless patients.This session includes an application of social media for employee, patient,and community information in real-time format. <strong>The</strong> presenters give seniorexecutive perspectives that will demonstrate systems of communicationproven to be successful in sustaining operations and recovering staff andpatients during and after hurricane events in an integrated multiregionalmarket.Learning Objectives:u Cite real-life cases of evacuations and shelter-in-place due toprojected direct impact storms.u Discuss utilization of patient safety systems before, during, and afterevacuations.u Assess perspectives of senior leadership team and incident commandleaders in sustaining facility operations and completing successfulrecovery efforts.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, nurses, pharmacists, physicians,social workersSession 58: A Comparison of U.S. and CanadianEmergency Support Functions: Public Health, Medical,and Human ServicesPresenters: CAPT Brad Austin, MPH, FACHE; LCDR Steven Kempton;André La PrairieTime: 0830-0945 hrsRoom: Delta BFocus Area: Response Integration/Operational MedicineBoth Canada and the United States have adopted national emergencyresponse systems that incorporate the use of emergency support functions(ESFs). ESFs provide the mechanisms for grouping functions most frequentlyused in providing Federal support to states, provinces, territories, andother Federal departments and agencies prior to or during an emergency.ESFs describe the roles and responsibilities of Federal departments andagencies and are allocated to Federal government institutions in a mannersession Descriptions<strong>2012</strong> Integrated Training Summit 57
FRIday, May 25, <strong>2012</strong>Session Descriptionssession Descriptionsconsistent with their respective mandates, policies, and legislation. Whilethe ESF architecture used in the United States and Canada is similar, thereare significant and important variations between the two countries wherethe delivery of public health, medical, and human services is concerned. InCanada, the Public Health Agency of Canada is assigned the lead for ESF-5 ofthe Federal Emergency Response Plan, “Public Health and Essential HumanServices.” In the U.S. National Response Framework, the Department of Healthand Human Services is assigned as the ESF coordinator as well as the primaryagency for ESF#8, “Public Health and Medical Services.” In this session, thetwo complementary ESFs will be compared and contrasted to provide ananalysis of the similarities and differences regarding their scope, conceptsof operations, and delivery arrangements, and the session will also highlightany perceived gaps in emergency planning in the public health and medicalfields. Participants at this session will gain a better understanding of the ESFconcepts in both countries, as well as learn how the two ESFs are expected tointeract during a cross-border emergency where public health, medical, andhuman services are involved. In addition, both countries are in the beginningstages of working out the details of how both medical personnel and medicalcountermeasures could be shared with the other country. An update on thiswork will also be presented in the context of each country’s ESF.Learning Objectives:u Recite an understanding of how ESFs in Canada and the UnitedStates are structured regarding the Federal response to public health,medical, and human services aspects of an emergency in each country.u List ESF resources used in Canada and the United States and how theymay augment and support the primary Federal government programs,arrangements, and other measures used to deliver ESFs.u Explain how the Canadian and U.S. ESF resources and assets aredeployed and utilized in the event of a cross-border emergency.Intended Audience: Certified counselors, dentists, emergency physicians,EMT/paramedics, environmental health personnel, healthcare executives,health education specialists, industrial hygienists, marriage & familytherapists, medical administrators, nurses, physicians, social workersSession 59: “Survey Says” . . . !Presenter: Gary LindberghTime: 0830-0945 hrsRoom: Governor’s BFocus Area: Response Integration/Operational MedicineThis fun, interactive session will challenge participants to solve problemsfaced during actual responses. Participants will be presented with a challengefaced by ESF#8 responders during a deployment. Participants will then beable to pick one solution, using the audience response system, and see theresponses of other audience members before finding out how the real-liferesponders reacted.Learning Objectives:u Develop problem-solving skills by working through actual challengesfaced on deployments.u Discuss strategies for responding to deployment challenges.u Develop problem-solving skills and new strategies to respond todisasters and public health emergencies.Intended Audience: Emergency physicians, EMT/paramedics, healthcareexecutives, health education specialists, medical administrators, nurses,physicians**Closing Remarks**Presenter: RADM Nicole Lurie, MD, MSPH, Assistant Secretary for<strong>Preparedness</strong> and Response (ASPR)Time: 1015-1045 hrsLocation: Delta A BallroomSession 60: Room for Mistakes: Learning <strong>from</strong>International Disaster ResponsePresenter: Isaac Ashkenazi, MD, MSc, MPATime: 1045-1215 hrsRoom: Delta A BallroomFocus Area: General SessionGlobal disasters during the past decade remind us that catastrophicdisasters, both natural and man-made, continue to claim the lives ofmillions. <strong>The</strong> ability to respond effectively varies substantially betweencitizens, governments, nongovernmental organizations, and internationalorganizations. Dr. Isaac Ashkenazi of the Harvard School of Public Healthhas drawn lessons about training professional responders <strong>from</strong> the recentdisasters, including physicians, nurses, EMT/paramedics, pharmacists, dentists,environmental health personnel, and other allied healthcare professionals.He discusses the limits of government preparedness and the inclusion ofordinary citizens in preparedness planning for disasters. In developingtraining for professional responders, leaders must understand that mistakeswill be made and that they should ensure that the lessons of those mistakesare shared so others can learn <strong>from</strong> them. In an environment demandingperfection, where mistakes are forbidden, mistakes get hidden, and the resultis a culture of blame, not learning. Dr. Ashkenazi’s research has focused onurban terrorism and the increasingly complex role of governmental disasterresponse in foreign crisis situations, such as Haiti’s devastating earthquakeand the Japanese tsunami and earthquake. This session will review his recentresearch, including “Disaster Response: A Decade of Lessons Learned Post9/11” and the speaker’s personal experience of key lessons learned, includingstrategies for future U.S. international engagement.Learning objectives:u Discuss the complexities of international disaster response.u Differentiate the roles of citizens, government-trained responders, andnongovernmental or private sector actors.u Explain general lessons learned and their application for improvedUSG international response.Intended Audience: Certified counselors, dentists, emergencyphysicians, EMT/paramedics, environmental health personnel, healthcareexecutives, health education specialists, industrial hygienists, marriage &family therapists, medical administrators, morticians, nurses, physicians,psychologists, respiratory therapists, social workers, veterinarians58<strong>2012</strong> Integrated Training Summit
Tuesday, May 22, <strong>2012</strong>MRC WorkshopsMRC Workshops1. Unit Activity ReportingPresenters: Dani Holliday; Sonia JordanTime: 0800-0900 hrs – Also offered at 1300-1400 hrsRoom: Ryman Studio JKMRC unit leaders are required to update their unit profiles at least onceevery three months, and one of the most important sections of the MRCunit profile is unit activities. It provides information about the unit’s futureand three most recent activities to current and prospective MRC volunteersand partners. In addition, the DCVMRC uses this information in reports,newsletters, briefings, and sessions to inform senior leaders and stakeholdersabout the breadth and scope of MRC unit activities. By providing meaningful,detailed reports of unit activities, unit leaders help to increase the strengthof the entire MRC network. This workshop will guide participants throughthe process of reporting unit activities on their MRC unit profiles and providethem with examples of useful and informative activity reporting.Participants in this workshop are highly encouraged to bring their ownlaptops for hands-on practical experience.Learning Objectives:u Demonstrate logging into the unit profile.u Distinguish between activity types using the activity report.u Employ the key components of an activity report.2. New Leader WorkshopPresenters: Gary Brown, Sandy Collins; Cathy Flores; Emily NickelTime: 0800-1200 hrs – Also offered at 1300-1700 hrsRoom: Ryman Studio PQRThis workshop will provide new MRC leaders with some basic tips forbuilding and establishing an MRC unit. Division of the Civilian VolunteerMedical Reserve Corps staff and leaders <strong>from</strong> the MRC network willhighlight key points such as the MRC vision, MRC leadership principles,MRC roadmap, community buy-in and participation, a framework of policiesand procedures, network resources, and education and training.Learning Objectives:u Describe the MRC vision, mission, and goals.u Demonstrate leadership principles necessary to obtain communitybuy-in.u Identify education, training, and network resources for unitdevelopment.3. MRC-TRAIN: <strong>The</strong> BasicsPresenter: Erin BougieTime: 0800-1200 hrs – Also offered at 1300-1700 hrsRoom: Ryman Studio LThis interactive workshop will provide a detailed overview of the MRC-TRAINlearning management system. <strong>The</strong> presenter will discuss the groupingstructure, administrative rights, and ways that MRC leaders and volunteerscan best leverage this training resource. Participants will work throughhands-on activities ranging <strong>from</strong> creating a user account and registering fora course to developing and assigning a training plan and accessing cannedreports.Participants in this workshop are highly encouraged to bring their ownlaptops for hands-on practical experience.Learning Objectives:u Create a user account on MRC-TRAIN.u Register for a course on MRC-TRAIN.u Assign a training plan using MRC-TRAIN.4. MRC Seasoned Leader WorkshopPresenters: Becky Beiter; Samantha Brann; Kathleen Conley-Norbut;Sandy MillerTime: 0800-1200 hrs – Also offered at 1300-1700 hrsRoom: Ryman Ballroom EFThis workshop will provide seasoned MRC leaders with tips for strengtheningand sustaining an MRC unit. Division of the Civilian Volunteer MedicalReserve Corps staff and experienced leaders <strong>from</strong> the MRC network willhighlight key topics such as leadership principles, fundamentals of volunteermanagement, training plans, risk reduction methods, strategic roadmappingprocesses, and mentorship models.Learning Objectives:u Design training plans for an established MRC unit.u Propose strategic road-mapping projects for the local unit.u Develop a mentorship program for the local unit.5. Strategic Road-Mapping: Planning for SuccessPresenter: Kristen LeporeTime: 0800-1200 hrsRoom: Ryman Studio MNOMRC Workshops<strong>2012</strong> Integrated Training Summit 59
Tuesday, May 22, <strong>2012</strong>MRC WorkshopsMRC WorkshopsStrategic road-mapping is about best positioning MRC units for success.It is used to maximize available resources, align work, drive consensus,and provide stakeholders with a clear idea of what leaders are looking toaccomplish. Both old and new units alike benefit <strong>from</strong> this approach toprogramming. This workshop will walk participants through a strategicroad-mapping process, enabling them to create a plan of their own. <strong>The</strong>workshop, tailored to MRC units and unit leaders, will emphasize practicalsolutions for planning and provide opportunities for cross-collaboration.Core components of the workshop include conducting pre-plan assessments,developing mission and vision statements, setting goals and objectives,implementation and tracking, and evaluation.Learning Objectives:u Become familiar with the tenets of strategic road-mapping (mission,goals, objectives, etc.).u Assess current MRC operations and identify individual unit areas ofdevelopment.u Create a basic strategic roadmap, and through peer interaction, refinegoals and objectives.6. Volunteer Management: LeadershipPresenters: Jean Roma; Debi WagnerTime: 0800-1000 hrs – Also offered at 1300-1500 hrsRoom: Ryman Studio FGLeaders of local MRC units engage volunteers to strengthen public health,emergency preparedness and response, and community resiliency. <strong>Through</strong>their stewardship, MRC units participate in a variety of activities thatpositively impact their communities. Although each MRC unit is different,with varying missions, organization and composition, and communitiesto support, there are elements common to effective and successful MRCunit leaders. This workshop will provide participants with leadership tips,techniques, and promising practices that will assist them in leading theirvolunteers, managing their MRC units, working with partner organizations,and effectively serving their communities.Learning Objectives:u Demonstrate techniques of effective leadership.u Compare and contrast various leadership styles.u Examine differentiation between internal and external leadership.7. Getting the Word Out: An MRC Messaging WorkshopPresenter: Jennifer FrenetteTime: 0800-1000 hrs – Also offered at 1300-1500Room: Ryman Studio EThis is a fast-paced, interactive, brainstorming approach to configuring anddelivering the right message, to the right audience, using the right medium,for a desired result. <strong>The</strong> workshop will require some creativity. Positivethinking a plus. All will walk away with the tools necessary to present anappropriate message for their organization.Learning Objectives:u Define the strengths and weaknesses of the focus organization.u Identify the most appropriate audience for the intended message.u Create, articulate, produce, and deliver an accurate message, to themost appropriate audience, using the best medium.8. Overview of Disaster Risk ReductionPresenters: Mark Keim; Mollie MahanyTime: 0800-1700 hrsRoom: Ryman Studio ABC<strong>The</strong> UN defines disaster risk reduction (DRR) as “the concept and practiceof reducing disaster risks through systematic efforts to analyze and managethe causal factors of disasters, including through reduced exposure tohazards, lessened vulnerability of people and property, wise management ofland and the environment, and improved preparedness for adverse events.”This workshop will describe key DRR concepts and provide participants withan understanding of the practical applications for developing DRR plans intheir communities. <strong>The</strong> workshop format consists of lectures, discussion,and interactive learning labs.Learning Objectives:u Understand the principles and application of disaster risk reduction.u Enhance the participants’ capability to support and plan DRR activitiesin their communities.9. Elements of Sustainability for GrassrootsOrganizationsPresenters: Liisa Jackson, Stacy Sayre, Loren SteinTime: 0800-1000 hrs – Also offered at 1300-1500 hrsRoom: Ryman Studio HIThis workshop will explore key elements of sustainability and help MRCleaders identify sustainability strengths and challenges. In addition toassisting participants in addressing the identified challenges, the presenterwill provide tips on how to work toward organizational sustainability bykeeping volunteers involved and informed and by engaging key stakeholdersand outside decision makers.60<strong>2012</strong> Integrated Training Summit
Tuesday, May 22, <strong>2012</strong>MRC WorkshopsLearning Objectives:u Identify key elements of sustainability.u Examine elements of organization sustainability.u Design methods for engaging key stakeholders and outside decisionmakers.10. Unit Leader Transition PlanningPresenters: Carla Mitchell; Gail NewellTime: 0900-1000 – Also offered at 1400-1500 hrsRoom: Ryman Studio JKLike any organization, MRC units will experience changes in leadership.This transition can be smooth or tumultuous, depending on how well theMRC unit has planned for transitions in leadership. This workshop will helpparticipants plan for leadership changes and introduce them to the Guide toMRC Unit Leader Transitions, a document designed to make the transitionto a new MRC unit leader as smooth as possible so that an MRC unit cancontinue to develop and grow even during the transition.Participants in this workshop are highly encouraged to bring their ownlaptops for hands-on practical experience.Learning Objectives:u Identify resources for unit leader transitions.u Develop a checklist for outgoing unit leaders.u Demonstrate steps necessary to transition the unit profile <strong>from</strong> oneunit leader to another.11. Diversity of FundingPresenters: Eugene Heighton; Carter PittmanTime: 1000-1100 hrs – Also offered at 1500-1600 hrsRoom: Ryman Studio HIDue to the limited availability of government funding, it is essential for MRCunits to obtain financial and material resources <strong>from</strong> a variety of sources. Thisworkshop will help participants identify potential opportunities for fundingand resources and provide them with creative tips, advice, and guidance forsecuring a variety of different funding and other resources.Learning Objectives:u Describe the importance of a variety of funding sources.u Identify public and private funding sources.u Locate resources to assist with securing funding.12. Volunteer Management: Recruitment and RetentionPresenters: Cheryl Kehnast; Shaila SimmonsTime: 1000-1200 hrs – Also offered at 1500-1700 hrs in both RymanStudio FG and Ryman Studio ERoom: Ryman Studio FGVolunteers are the basis of the MRC. <strong>The</strong> existence of this nationwide,community-based network is due to the willingness of volunteers to serve theircommunities in times of need and to address ongoing public health challenges.Without this generous service, there would be no MRC. Hence, recruitingand retaining volunteers is fundamental to the development, growth, andeffectiveness of any MRC unit. This workshop will provide participants withtools, techniques, and promising practices that will assist them in recruitingand retaining competent, energetic, and motivated volunteers.Learning Objectives:u Examine the importance of recruitment.u Design effective retention programs.u Apply volunteer motivation techniques.13. MRC-TRAIN: Create Training PlansPresenter: Ilya PlotkinTime: 1000-1200 hrs – Also offered at 1500-1700 hrsRoom: Ryman Studio JKThis interactive workshop will demonstrate the following features of theMRC-TRAIN learning management system: becoming a course provider andposting a course or conference, creating and managing a training plan,and creating and running a report. Participants should come equipped withan understanding of MRC-TRAIN and will work through hands-on activitiesthat will range <strong>from</strong> developing and assigning a training plan to creatingand running personalized reports.Participants in this workshop are highly encouraged to bring their ownlaptops for hands-on practical experience.Learning Objectivesu Design a training plan.u Prepare personalized reports.u Manage adding a course or conference to MRC-TRAIN.14. Cultural Efficacy: Putting Cultural Competency toWork in the MRCPresenter: <strong>The</strong>rese QuinnTime: 1000-1200 hrsRoom: Ryman Studio E<strong>2012</strong> Integrated Training Summit 61MRC Workshops
Tuesday, May 22, <strong>2012</strong>MRC WorkshopsMRC WorkshopsThis interactive session will give participants a background in culturalcompetency, beyond ethnicity. Using the Camphina-Bacote model,the workshop will touch on the five constructs of cultural competency:awareness, knowledge, skills, encounters, and desire. Emphasizing thatcultural competency is a lifetime process, the workshop will discuss whatculture is; why cultural awareness is important; why self-awareness isimportant; and how culture is a factor in all phases of public health andemergency management. <strong>The</strong> workshop will also offer a brief discussion ofthe “isms” (i.e., racism, sexism, homophobia, etc.).Learning Objectives:u Describe each participant’s personal culture.u Identify ways to connect with diverse cultures in the community.u Identify ways that MRC units can build community resilience throughcultural efficacy.15. Proposal Development (Awards and Funding)Presenters: Kathy Handra; Kathy KnightTime: 1100-1200 hrs – Also offered at 1600-1700 hrsRoom: Ryman Studio HIA unit leader may often submit an application for a grant or financial awardor may seek to recognize the achievements of an outstanding volunteer. Howdo you write a successful grant proposal or a winning award nomination?Creating an effective write-up may be particularly important due to thelimited availability of funding or in the face of stiff competition <strong>from</strong> peers.This workshop will provide participants with tips, techniques, and strategiesto enhance their ability to craft well-written, superior grant proposals andaward applications.Learning Objectives:u Differentiate between grants and awards.u Identify potential grant and award sources.u Identify resources and guidance for writing a proposal.16. Growing Leaders <strong>from</strong> WithinPresenter: Charlie BryanTime: 1300-1700 hrsRoom: Ryman Studio MNOGiven the limited time and resources available to MRC leaders, more andmore opportunities are becoming available for active MRC volunteers totake on leadership roles. This workshop will provide MRC leaders withtools, techniques, and promising practices that will assist their units inidentifying leadership potential and empowering volunteers to carry outmore responsibilities. <strong>The</strong> presenter will provide tips on how to enhancethe skills and abilities of volunteers who demonstrate the potential to growwithin the unit and housing organization structure.Learning Objectives:u Illustrate the benefits of MRC volunteers taking on leadership roles.u Identify leadership potential among volunteers.u Formulate ways in which to empower volunteers to carry outadditional responsibilities.62<strong>2012</strong> Integrated Training Summit
Continuing Education InformationContinuing EducationInformationTraining Summit Goals<strong>The</strong> goals for the Integrated Training Summit include:1. Deliver an understanding of the health and medical requirementsgenerated by disasters of any origin.2. Provide access to authorities responsible for managing theserequirements.3. Afford opportunities for the delivery of education and the exchange ofideas necessary to the development of capabilities at the local, State,regional, National and international levels.Training Summit Objectives<strong>The</strong> educational program for the Integrated Training Summit will:1. Convey the principles which underlie professional emergency healthand medical service delivery.2. Document the status of the profession as of 2011/<strong>2012</strong>.3. Encourage the participant to engage in continuing education, training,research, and information sharing.<strong>The</strong> <strong>2012</strong> Integrated Medical, Public Health, <strong>Preparedness</strong> and ResponseTraining Summit is sponsored by the U.S. Department of Health and HumanServices (HHS). This Training Summit brings together HHS partners includingthe National Disaster Medical System (NDMS), the Medical Reserve Corps(MRC), the Emergency System for Advance Registration of Volunteer HealthProfessionals (ESAR-VHP), and the United States Public Health Service(USPHS). <strong>The</strong> Integrated Training Summit is co-sponsored by the ChesapeakeHealth Education Program, Inc. (CHEP.INC)This forum permits coordination, collaboration and interaction amongstthe target audience - the leaders and members of these preparednessand response partner organizations. <strong>The</strong> Integrated Training Summit willenhance the knowledge, skills and abilities of participants, which in turn willimprove their capability to deliver public health and medical care servicesduring disasters of any origin. Expert faculty will present on key focus areas;Healthcare Systems & Clinical Care Services, Leadership, Public Health,Resource Management & Patient Movement, and Response Integration.Networking with these expert faculty members and fellow participants, manyof whom are the nation’s leaders in the area of public health emergencies, willprovide insight into the latest information available in the area of emergencyresponse and coordination.Strategic Direction<strong>The</strong> vision for the <strong>2012</strong> Integrated Medical, Public Health, <strong>Preparedness</strong> andResponse Training Summit is to have a robust, well-trained and integratedpool of public health and medical responders who understand their rolesand missions in times of need, as well as those of their response partners, inorder to best serve our communities, states, tribes, and the nation.<strong>The</strong> Integrated Training Summit will achieve this vision by convening aforum for conducting training, discussing issues, sharing information,and networking amongst the constituent groups of various National-levelorganizations involved in preparing for and responding to public health andmedical emergency events. Some specific strategies for <strong>2012</strong> include:❖ Reinforce the relationships between the public health and responsepartner organizations❖ Focus on all-hazards approaches❖ Enable facilitated, interactive learning opportunitiesTarget AudienceSummit is designed for:Certified CounselorsCertified Health Education SpecialistsDentistsEmergency ManagersEmergency Medical Services PersonnelEmergency PlannersEnvironmental Health SpecialistsForensic SpecialistsHealth Care AdministratorsIndustrial HygienistsInfectious Disease Specialists/EpidemiologistsMarriage & Family <strong>The</strong>rapistsMedical AdministratorsMorticiansNursesPharmacistsPhysiciansPsychologistsPublic Health WorkersRespiratory <strong>The</strong>rapistsResponse Team PersonnelSocial WorkersState and Local Public Health OfficialsVeterinariansContinuing Education CreditsFor the <strong>2012</strong> Integrated Training Summit, participants are offered twooptions for completing evaluations in order to receive a continuingeducation certificate/statement of credit. Participants may either visit an onsiteevaluation station or complete evaluations after returning home <strong>from</strong>the conference at http://www.chepinc.org/Certificates/. On-line evaluationstation hours will be prominently posted around the conference center andare included in this manual. <strong>The</strong> stations will be located near the Summitregistration area.PLEASE NOTE: Participants must complete ALL evaluations plus the overallTraining Summit evaluation before a certificate print icon is available.Certificates will be printed <strong>from</strong> your home/office computer. Printers will notbe available at the evaluation stations and no certificates will be mailed.Please confirm your email address with the Summit staff to ensure youreceive the evaluation link and certificate information.Continuing Education info<strong>2012</strong> Integrated Training Summit 63
Continuing Education InformationContinuing Education infoBY COMPLETING THESE EVALUATIONS YOU VERIFY YOUATTENDED EACH SESSION IN ITS ENTIRETY.PLEASE NOTE: Several of the workshops/sessions offered in 2011 arerepeated this year. Participants may not earn CEUs/CMEs for repeatattendance at a workshop / session within a 12 month period.Report of TrainingIt is the program participant’s responsibility to ensure this training isdocumented in the appropriate location according to his/her locallyprescribed process.Certificate of AttendancePLEASE READ THIS IMPORTANT INFORMATION CAREFULLYAll participants seeking continuing education credits must have theirsummit badge scanned by a room administrator outside of eachclassroom. Participants who do not have their badge scanned will NOTreceive credits. It is the responsibility of each attendee to confirm the sessionthey are attending is accredited for their discipline. <strong>The</strong> audience key, whichcan be found in the Agendas-At-A-Glance, provides this information.New ACPE Continuing Education Credit Tracking SystemAll U.S. pharmacists and technicians must obtain an NABP e-Profile IDnumber at www.myCPEmonitor.net. In order to receive ACPE credits forthe <strong>2012</strong> Integrated Training Summit, pharmacists and technicians MUSTprovide your NABP e-Profile ID and date of birth at the registration desk.Your Training Summit attendance data / credits will be transmitted directlyto the Summit ACPE provider who will forward to ACPE / NABP. Once NABPreceives the information, pharmacists and technicians will be able to login to access information about their completed CPE activities. Paper CPEstatements of credits will no longer be distributed.Mandatory meetings and invitational sessions are not eligible for continuingeducation credits.Continuing Education StatementsAAMA: Medical Administrators<strong>The</strong> American Academy of Medical Administrators has approved thisprogram for AAMA continuing education contact hours.Full Training Summit and WorkshopsMaximum of 28.5 HoursAAMA members are responsible for recording and reporting theirown continuing education activities.AARC: Respiratory <strong>The</strong>rapists<strong>The</strong> Continuing Respiratory Education (CRCE) system of the AmericanAssociation for Respiratory Care (AARC) grants approval for the <strong>2012</strong>Integrated Training Summit.Full Training Summit and WorkshopsMaximum of 29.75 HoursAAVSB-RACE: VeterinariansThis program was reviewed and approved by the AAVSB-RACE program for23 hours of continuing education in jurisdictions that recognize AAVSB-RACE approval. Please contact the AAVSB RACE program if you have anycomments or concerns regarding this program’s validity or relevancy to theveterinary profession. AAVSB provider # 74. Program # 74-7866.**CHEP (11E), Building 82H, Perry Point, MD 21902**Full Training Summit and WorkshopsMaximum of 23 hoursABIH: Industrial HygienistsABIH is the certifying body for the Certified Industrial Hygienist (CIH) andCertified Associate Industrial Hygienist (CAIH), the premier occupationalhygiene certifications in the world.Full Training Summit and WorkshopsMaximum of 27.25 hoursIndustrial Hygienists responsible for recording and reporting theirown continuing education activities to ABIH. Obtain an attendanceverification form at each approved workshop / session.ACEP: Emergency PhysiciansApproved by the American College of Emergency Physicians for a maximumof 29.75 hours of ACEP Category I Credit.Full Training Summit and WorkshopsMaximum of 29.75 HoursACHE: Healthcare Executives<strong>The</strong> Chesapeake Health Education Program, Inc. is authorized to award 28.5hours of pre-approved ACHE Qualified Education credit (non-ACHE) for thisprogram toward advancement or recertification in the American College ofHealthcare Executives. Participants in this program wishing to have thecontinuing education hours applied toward ACHE Qualified Education creditshould indicate their attendance when submitting application to the AmericanCollege of Healthcare Executives for advancement or recertification.Full Training Summit and WorkshopsMaximum of 28.5 HoursFor Continuing Pharmacy Education (ACPE)<strong>The</strong> Indian Health Service Clinical Support Center is accredited by theAccreditation Council for Pharmacy Education as a provider of continuingpharmacy educationSession/Workshop ACPE Approval #Session 3Session 4Session 8Session 9Session 11Session 12Session 17Session 180600-0000-12-701-L04-P0600-0000-12-702-L04-P0600-0000-12-703-L04-P0600-0000-12-704-L04-P0600-0000-12-705-L04-P0600-0000-12-706-L04-P0600-0000-12-707-L04-P0600-0000-12-708-L04-P64<strong>2012</strong> Integrated Training Summit
Continuing Education InformationSession 23Session 26Session 28Session 30Session 35Session 38Session 47Session 57Workshop NWorkshop QWorkshop RWorkshop UWorkshop VFull Training Summit and WorkshopsMaximum of 21 hours of creditADA: Dentists, Dental Hygienists0600-0000-12-709-L04-P0600-0000-12-710-L04-P0600-0000-12-711-L04-P0600-0000-12-712-L04-P0600-0000-12-713-L04-P0600-0000-12-714-L04-P0600-0000-12-715-L04-P0600-0000-12-716-L04-P0600-0000-12-717-L04-P0600-0000-12-718-L04-P0600-0000-12-719-L04-P0600-0000-12-720-L04-P0600-0000-12-721-L04-P<strong>The</strong> Chesapeake Health Education Program Inc. is an ADA CERP RecognizedProvider. ADA CERP is a service of the American Dental Association to assistdental professionals in identifying quality providers of continuing dentaleducation. ADA CERP does not approve or endorse individual coursesor instructors, nor does it imply acceptance of credit hours by boards ofdentistry.Concerns or complaints about a CD provider may be directed to the provideror to ADA CERP at ADA.org/goto/cerp.Full Training Summit and WorkshopsMaximum of 28.5 HoursAMA PRA Category 1 Credits TM : PhysiciansChesapeake Health Education Program Inc. is accredited by MedChi, theMaryland State Medical Society, to provide continuing medical educationfor physicians.Chesapeake Health Education Program Inc. designates this educationalactivity for a maximum of 29.75 AMA PRA Category 1 Credits TM . Physiciansshould only claim credit commensurate with the extent of their participationin the activity.Full Training Summit and WorkshopsMaximum of 29.75 HoursANCC: NursesChesapeake Health Education Program Inc. is accredited as a provider ofcontinuing nursing education by the American Nurses Credentialing Center’sCommission on Accreditation.Full Training Summit and WorkshopsMaximum of 29.75 HoursAPA: Psychologists<strong>The</strong> VA Maryland Health Care System is approved by the AmericanPsychological Association to sponsor continuing education for psychologists.<strong>The</strong> VA Maryland Health Care System maintains responsibility for thisprogram and its contents. 8.5 credit hours.Maximum approved credit hours: 8.5Sessions approved: 4, 7, 24, 32, 40, 42, 56, 60CECBEMS: Emergency Medical TechniciansThis continuing education activity is jointly sponsored by UMBC, an accreditedCECBEMS organization. This continuing education activity is approved by theContinuing Education Coordinating Board for Emergency Medical Services(CECBEMS). You have participated in a continuing education programthat has received CECBEMS approval for continuing education credit. Ifyou have any comments regarding the quality of this program and/or yoursatisfaction with it, please contact CECBEMS at 12200 Ford Road, Suite478, Dallas, Texas 75324 (telephone 972-247-4442; lsibley@cecbems.org).CECBEMS represents only that its accredited programs have met CECBEMSstandards for accreditation. <strong>The</strong>se standards require sound educationalofferings determined by a review of their objectives, teaching plan, faculty,and program evaluation processes. CECBEMS does not endorse or supportthe actual teachings, opinions, or material content as presented by thespeaker(s) and/or sponsoring organization. CECBEMS accreditation does notrepresent that the content conforms to any national, state, or local standardor best practice of any nature. No student shall have any cause of actionagainst CECBEMS based on the accreditation of the material.Full Training Summit and WorkshopsMaximum of 29.75 HoursCECBEMS Provider #: UMBC0004CHES: Health Education SpecialistsChesapeake Health Education Program Inc. is designated a provider ofCategory I continuing education contact hours (CECH) in health educationby the National Commission for Health Education Credentialing Inc.28.5 CECH Provider #MEP3783Full Training Summit and WorkshopsMaximum of 28.5 HoursMFT & LCSW: Marriage & Family <strong>The</strong>rapistsLicensed Clinical Social Workers of CaliforniaCourse meets the qualifications for 15.25 hours of continuing educationcredit for MFTs and/or LCSWs as required by the California Board ofBehavioral Sciences #PCE2787.Full Training Summit and WorkshopsMaximum of 15.25 HoursMorticiansThis continuing education program has been approved by the MarylandState Board of Morticians for 19.25 contact hours (1 hour = 1 contacthour).Full Training Summit and WorkshopsMaximum of 19.25 HoursContinuing Education info<strong>2012</strong> Integrated Training Summit 65
Continuing Education InformationNASW: Social WorkersThis program is approved by the National Association of Social Workers(Approval #886496759-9884) for Social Work continuing educationcontact hours.Full Training Summit and WorkshopsMaximum of 15.25 HoursNBCC: Certified Counselors<strong>The</strong> Chesapeake Health Education Program Inc. is approved by theNational Board of Certified Counselors (NBCC) to offer continuingeducation accreditation for national certified and licensed counselors. Weadhere to NBCC Continuing Education Guidelines. Provider #6140.This continuing education program has been approved by the NationalBoard of Certified Counselors for 15.25 contact hours.Full Training Summit and WorkshopsMaximum of 15.25 HoursNEHA: Environmental Health PersonnelThis course has been preapproved for 28.5 continuing education credits bythe National Environmental Health Association (NEHA).Full Training Summit and WorkshopMaximum of 28.5 HoursContinuing Education info66<strong>2012</strong> Integrated Training Summit
Planning CommitteeDawn AnastasiaChesapeake Health Education Program, Inc.DAnastasia@chepinc.orgAndrew Garrett, MD, MPHNDMSAndrew.Garrett@hhs.govJay MorrisHRSAJMorris@hrsa.govJoseph F. Annelli, DVM, MDUSDAJoseph.F.Annelli@aphis.usda.govJane GarrettChesapeake Health Education Program, Inc.JGarrett@chepinc.orgLT Skip Payne, MSPH, REHS/RSProgram OfficerSkip.Payne@hhs.govRoy Ball, ACNP-BC, CCNSR Adams Cowley Shock Trauma CenterRBall@umm.eduLeslie BeckHHS/ASPR/OPEO/NDMSLeslie.Beck@hhs.govCatherine Bennett, RN, MSChesapeake Health Education Program, Inc.CBennett@chepinc.orgAkiko Berkman, MPH, MPAOregon Health Authority Public Health DivisionAkiko.Berkman@state.or.usMike Boucher, RNDepartment of Veterans AffairsMichael.Boucher2@va.govGary W. BrownDivision of the Civilian Volunteer MedicalReserve CorpsGary.Brown@hhs.govJeff BryantCDCiqs3@cdc.govToby Clairmont, RN, CHEPHealthcare Association of HawaiiToby.Clairmont@hhs.govCDR Jeff Coady, PsyDSubstance Abuse and Mental Health ServicesAdministrationJeffrey.Coady@samhsa.govCraig DeAtley, PA-CWashington Hospital Center; NationalRehabilitation Hospitalflightpa.deatley@gmail.comPatrick Denis, MBA, BSN, BSHHS/OS/OASH/OSG/DCVMRCPatrick.Denis@hhs.govMorgan DeWeese, BAChesapeake Health Education Program, Inc.MDeWeese@chepinc.orgJohn Donohue, BS, EMT-PMaryland Institute for Emergency MedicalServices SystemsJDonohue@miemss.orgBonnie Gaughan-BaileyFlorida Department of Health, Bureau of<strong>Preparedness</strong> and ResponseBonnie_Gaughan-Bailey@doh.state.fl.usMark Gentilman, OD, CEM, FACCPOffice of the Assistant Secretary for Defensefor Health Affairs; Force Health Protection andReadiness ProgramsMark.Gentilman@tma.osd.milKatie Hager, BSN, RNDivision of the Civilian Volunteer MedicalReserve CorpsKatie.Hager@hhs.govCarly Hankins, BAChesapeake Health Education Program, Inc.CHankins@chepinc.orgJennifer HannahHHS/ASPR/ESAR-VHPJennifer.Hannah@hhs.govDarryl HardgeHHS/OS/OPEO/ASPR/HPPDarryl.Hardge@hhs.govAntonio HernandezArizona Department of Health Bureau of PublicHealth Emergency <strong>Preparedness</strong>Antonio.Hernandez@azdhs.govGerry Kelly, PhDChesapeake Health Education Program, Inc.GKelly@chepinc.orgDavid Kerschner, RN, MSNHHS/ASPR Region XDavid.Kerschner@hhs.govTom Lawrence, NREMT-PRI Disaster Med. Assistance TeamTLawrence@ridmat.orgLorie Liptakllliptak@aol.comJill LittlefieldHHSJill.Littlefield@hhs.govJillian Maxwell, BAChesapeake Health Education Program, Inc.JMaxwell@chepinc.orgGail Pfouts, RNChesapeake Health Education Program, Inc.GPfouts@chepinc.orgJean Popiak Goodwin, DHA, PMPCDClzp9@cdc.govAnn Potter, RNWashington Hospital CenterAnnmPotter@earthlink.netLCDR Johnnie Purify, MBAUSEPA; Region 4purify.johnnie@epa.govTeddy Rogers, MSA, NREMT-PNDMS/OPEO/ASPR/HHS/TN-1 DMATteddy.rogers@hhs.govHelga Scharf-Bell, MSN, RNHHSHelga.Scharf-Bell@hhs.govKirsten SloweyEastern Bay Event Companykirsten@easternbay.netBenjamin Swig, NREMT-BOS/OASH/OSG/DCCPRBenjamin.Swig@hhs.govCAPT Rob Tosatto, PRh, MPH, MBAHHS/OS/OASH/OSG/DCVMRCRobert.Tosatto@hhs.govCAPT Richard TurnerHISRichard.turner@ihs.govDan Wall, RN, BSN, PANDan.Wall@ventura.orgVentura County Public Health DepartmentDebra Wagner, CVA, NREMTOklahoma Medical Reserve Corps,Oklahoma State Department of Healthdebramw@health.ok.govPlanning CommitteeCAPT Kimberly Elenberg, RN, MS, DNPUSPHS/OFRD/OSGSonda Finley, PHR, MBAState MRC/ESAR-VHP CoordinatorSonda.Finley@tn.govLCDR Tiffany Moore, RN, BSNUSPHS/USMS/POD/OMOTiffany.Moore3@usdoj.gov<strong>2012</strong> Integrated Training Summit 67
Planning SubCommitteeLT Jeffrey BallKrome Service Processing Center/DIHSJeffrey.Ball@dhs.govMillard (Buddy) BellASPR/COO/DWDMillard.Bell@hhs.govCarlton (Skip) BowermanHHS/ASPR/OPEO/TELLCarlton.Bowerman@hhs.govMary Casey-Lockyer, BSN, RN, CCRNAmercian Red Crosslockyerm@usa.redcross.orgLT Christine Collins, RN, BSN, MAHHS/OSGChristinelmer@hotmail.comJamie Davis, PhDVA Maryland Health Care SystemJamie.Davis5@va.govCAPT Timothy Davis, MDHHS/ASPR/NDMSTim.Davis@hhs.govLisa DeDecker, RN, MSHQ AMC/SGKLisa.DeDecker.ctr@ustranscom.milErin Downey, MPH, ScDDepartment of State, INR, Office of theGeographerErinDowney@bellsouth.netTrish Factor, BS, MCHESWood County Health DepartmentTFactor@co.wood.oh.usMick FeeserVA VHA EMSHGMichael.Feeser@va.govKathy HandraDivision of the Civilian Volunteer MedicalReserve CorpsKathy.Handra@hhs.govElleen Kane, MA, APRHHS/ASPRElleen.Kane@hhs.govScott Kirley, RRTRegional Facility – FLDHHS/ASPR/OPEOScott.Kirley@hhs.govJoseph LamanaHHS/ASPR/OPEOJoseph.Lamana@hhs.govThomas MacKAYHHS/ASPR/OPEO/TELLThomas.MacKAY@hhs.govGretchen MichaelHHS/ASPRGretchen.Michael@hhs.govCDR Paul Reed, MDDCVMRC/OSGPaul.Reed@hhs.govMoira Shea, MPAOffice of the Assistant Secretary for<strong>Preparedness</strong> and ResponseMoira.Shea@hhs.govSandra Stark Shields, LMFT, CTSLA County Department of Health ServicesSanshields@dhs.lacounty.govLauren ToomeyASPR/OPEO/DPPLauren.Toomey@hhs.govApril Wood, BSN, RN, NREMT-BAmerican Red Cross National HeadquartersWoodA@usa.redcross.orgPlanning Subcommittee68<strong>2012</strong> Integrated Training Summit
PresentersBrian Abrahamson, BAGaylord EntertainmentBAbrahamson@GaylordEntertainment.comAkiko Berkman, MPH, MPA, BSOregon Health Authority-Pubic Health Dvisionakiko.berkman@state.or.usChristina Conti, MPPA, BAWashoe County Health Districtcconti@washoecounty.usCarl Adrianopoli, PhDHHS/ASPR/OPEOcarl.adrianopoli@hhs.govPaul Clement Alleyne, MDMeharry Medical CollegePalleyne@mmc.eduJerry Anderson, BS, MS, CHEPVW International, Inc.pembsly@gmail.comKnox Andress, RN, BA, ADLouisiana Posion Center; LSU Health - Shreveport,Louisiana; Region 7 Hospital <strong>Preparedness</strong>knoxandress@yahoo.comDiane Angelico, RNLSU Healthdangel@lsuhsc.eduJoseph H. AnnelliMaryland Department of Health and MentalHygiene Office of <strong>Preparedness</strong> and Responsejannelli@dhmh.state.md.usLindsey Anthony, MPA, CEMGeorgia Health Sciences Universitylanthony@georgiahealth.eduIsaac Ashkenazi, MD, MSc, MPACOL (Ret.) Israeli Defense Forces; Ben GurionUniversity of the Negev; Harvard University;International Expert for Crisis Management &LeadershipIsaac_Ashkenazi@KSG01.Harvard.eduCAPT Brad Austin, MPH, FACHEHHS/ASPR; Liaison Officer to the Public HealthAgency of CanadaBrad.Austin@phac-aspc.gc.caDennis Michael Baker, MA, LPCHHS/ASPR/OPEO/NDMS/ComCor, Inc.; NMRT-Central/ DMAT CO-2mbaker@comcor.orgAllison Banger, MPHRTI Internationalabanger@rti.orgCharles Bauer, MD, CPETexas Military Forces, Texas State Guard MedicalBrigade - Camp Mabry, Austin, TXcrbauermd@prodigy.netPaul Biedrzycki, MPH, MBACity of Milwaukee Heath Departmentpbiedrzycki@wi.rr.comArnie Bierenbaum, MSBooz Allen HamiltonBierenbaum_Arnie@bah.comCarolyn Blayney, RNUniversity of Washington Burn Center atHarborview; NDMS/IMSuRT Westcarolyn.blayney@hhs.govMike Boucher, BSN, MSNDepartment of Veterans AffairsMichael.Boucher@va.govCAPT Sean M. Boyd, MPH, USPHSHHS/FDAsean.boyd@fda.hhs.govJef Bratberg, PharmD, BCPSUniversity of Rhode Island; RI-1 DMATjefbratberg@yahoo.comNancy Carlson, BS, CFT, CFEMinnesota Department of HealthNancy.J.Carlson@state.mn.usPaul Carlton, Jr., MD, FACSTexas A&M Health Sciences CenterPkcarlton@tamhsc.eduMary Casey-Lockyer, RN, BSN, MHSAmerican Red Crosslockyerm@usa.redcross.orgLinda Cashion, RN, MSHHSlinda.cashion@hhs.govGarrick Clouden, MDMeharry Medical CollegeCloudeng@gmail.comJoseph Cocciardi, PhD, MS, CSPCocciardi and Assocates, Inc.; IRCTjoseph.cocciardi@hhs.govLT Christine Collins, RN, BSN, MAHHS; Office of the US Surgeon Generalchristine.collins@hhs.govMary ConnellyOak Ridge Institute for Science & Educationmary.connelly@orise.orau.govLCDR Meghan Corso, PsyDUSPHS; Department of Defense US Navy Bureauof Medicine and SurgeryMeghan.Corso@med.navy.milMarion Danis, MDNIHmdanis@nih.govCAPT Timothy Davis, MD, MPH, USPHSHHS/OS/ASPR/OPEO/NDMStim.davis@hhs.govCraig DeAtley, PA-CWashington Hospital Center NationalRehabilitation Hospitalflightpa.deatley@gmail.comLisa DeDecker, RN, MSHQ/AMC/SGKlisa.dedecker.ctr@us.af.milCDR Patrick Denis, MBA, BSN, RNHHS/OS/OASH/OSG/DCVMRCPatrick.Denis@hhs.govLeon Dent, MDMeharry Medical Collegeldent@mmc.eduAda Dieke, MPH, DrPH CUniversity of Arizona, Mel and Enid ZuckermanCollege of Public Health/CDCAdadieke@gmail.comCAPT Herman Allen Dobbs, MDNDMSallen.dobbs@hhs.govJason Dobronz, FPEMSeminole Indian Tribejasondobronz@semtribe.comJohn Donahue, BS, EMT-PMaryland Institute for Emergency MedicalServices Systemsjdonohue@miemss.orgDarrin DonatoHHSdarrin.donato@hhs.govTony Dunford, RNNemours/Alfred I. duPont Hospital for ChildrenDunfordt1@gmail.comCarma Erickson-Hurt, APRN, ACHPNErickson-Hurt Consultingecarma@hotmail.comPresenters<strong>2012</strong> Integrated Training Summit 69
PresentersPresentersSandy Evans, RN, MPHTulalip Tribes Medical Reserve Corpssevans@tulaliptribalpolice.orgBarry Fisher, MPHVentura County Public Health Departmentbarry.fisher@ventura.orgAndrew Garrett, MD, MPHHHS/ASPR/NDMSAndrew.Garrett@hhs.govJames Garrow, MPHPhiladelphia Department of Public Heathjames.garrow@gmail.comMAJ Micah GoettlOregon Army National Guardmicah.goettl@ng.army.milGerardo GomezMedical Readiness Training Center (MRTC)ggomez@icfi.comLori Gordon, DVMMassachusetts Task Force 1 Urban Seacrch andRescue; NVRT-1Jellegl@gmail.comTimothy Grapes, MSOffice of Interoperability and CompatibilityTimothy.Grapes@sesolutions.comRichard GreenASPCAdick.green@aspca.orgDan Hanfling, MDInova Health Systemdan.hanfling@inova.orgCynthia Hansen, PhDHHS/ASPR/OPEOCynthia.Hansen@hhs.govCAPT Kenneth Harman, MDUSCG Aviation Training Centerkenneth.r.harman@uscg.milLT COL Heidi Hastings, FACHEUSTRANSCOMheidi.hastings@ustranscom.milA.J Heightman, MPA, EMT-PJournal of Emergency Medical ServicesA.J.Heightman@Elsevier.comFred M. Henretig, MDChildren’s Hospital of Philadelphiahenretig@email.chop.eduJason E. Henry, RN, EMT, BACoxHealthJason.Henry@coxhealth.comCAPT Steven Hirschfeld, MD, PhDUSPHS/NIH; Eunice Kennedy Shriver NationalInstitute of Child Health and Human Developmenthirschfs@mail.nih.govArchie HirschmannGeorgia Health Sciences Universitypara252@knology.netBen Ho, MDOakland US&R Task Force CATF-4; USARcalsardogs@hotmail.comJudy Homer, RNNY State Department of Health Office of HealthEmergency <strong>Preparedness</strong> (OHEP)jlh20@health.state.ny.usJack HornerNational Disaster Life Support Foundationjhorner@georgiahealth.eduJerry Jaax, DVM, ACLAMKansas State Universityjaax@ksu.eduRachel KaulHHSrachel.kaul@hhs.govArthur Kellermann, MD, MPH, FACEP<strong>The</strong> RAND Corporationalk@rand.org;mdennis@rand.orgLCDR Steven Kempton, CD, MMMPublic Health Agency of Canadasteven.kempton@phac-aspc.gc.caAaron Kenneston, CEMWashoe County Office of EmergencyManagement and Homeland SecurityAKenneston@washoecounty.usMarie Kerl, DVM, MPH, DACVIMUniversity of Missouri; NVRT-3kerlm@missouri.eduMary Alice King, MD, MPHHarborview Medical Center; Seattle Children’s;University of Washington - Seattlemaryking@u.washington.eduHoward Klausner, MD, FACEPHenry Ford Hospital; MI-1 DMAThklausn1@hfhs.orgRADM Ann Knebel, RN, DNSc, FAANHHS/ASPR/OPEO/DPPann.knebel@hhs.govKathryn Koelemay, MD, MPHPublic Health - Seattle & King County/King CountyHealthcare Coalitionkathryn.koelemay@kingcounty.govJimmy Koeninger, PhDHOSAjim.koeninger@hosa.orgDebra Kreisberg, PhDUniversity of Colorado School of Medicinedebra.kreisberg@ucdenver.eduAndré La PrairiePublic Health Agency of Canadaandre.laprairie@phac-aspc.gc.caJoe LamanaHHSjoseph.lamana@hhs.govMike Lambert, EMT-P, AAPrince George’s County Fire/EMS Departmentmedicjack80@Comcast.netTom Lawrence, NREMT-PRI DMAT/RI MRC; RI-1 DMATtlawrence@ridmat.orgThomas LehmanNDLS National Training Center - West; UTSouthwestern Medical Center at DallasThomas.Lehman@UTSW.eduCAPT Mark Libby, RNHHS/ASPR; Region IMark.Libby@hhs.govNigel Lightfoot, MSc, FRCPath, FFPH<strong>The</strong> Globain Health Security InitiativeNigel.Lightfoot@mac.comGary LindberghHHS/ASPR; Division of Workforce DevelopmentEthics Branchgary.lindbergh@hhs.govLorie Liptakllliptak@aol.comKevin Locke, MDIA-1 DMATLocke.Kevin@mayo.eduRADM Boris Lushniak, MD, MPHHHS/USPHSBoris.Lushniak@hhs.govShannon Manzi, PharmDChildren’s Hospital Boston; MA-1 DMATshannon.manzi@childrens.harvard.eduDavid Marcozzi, MD, MHS-CL, FACEPHHS/ASPR/OPEODavid.marcozzi@hhs.govGregg Margolis, PhD, NREMT-PHHS/ASPR; Division of Health Systems and HealthCare Policygregg.margolis@hhs.gov70<strong>2012</strong> Integrated Training Summit
PresentersMary Massey, BSN, MA, MEPCalifornia Hospital Association; CA-1 DMATmsmassey@cox.netMarianne Matzo, PhD, FPCN, FAANUniversity of Oklahoma Health Sciences CenterCollege of Nursingmmatzo@ouhsc.eduJeanne McBride, MS, BSOak Ridge Institute for Science & Educationjeanne.mcbride@orise.orau.govKevin McCulleyUtah Department of Health Bureau of EMS and<strong>Preparedness</strong>kmcculley@utah.govBonnie McGuffinOak Ridge Institute for Science & EducationBonnie.McGuffin@orise.orau.govR. Douglas Meckes, DVMOffice of Health Affairs Department of HomelandSecuritydoug.meckes@dhs.govCAPT A. Thomas Mignone, Jr, MPHHHSthomas.mignone @hhs.govGlenn Mitchell, MD, MPHPhysician Change Managementmitchellmd@aol.comMargaret R. Moon, MD, MPH, FAAPJohns Hopkins School of Medicine, Departmentof Pediatrics and Johns Hopkins Berman Instituteof Bioethicsmmoon4@jhmi.eduLCDR Tiffany Moore, RN, BSNUSPHS; United States Marshals ServiceTiffany.Moore3@usdoj.govCAPT David Morrissette, PhD, LCSWHHS/SAMSHSAdavid.morrissette@samhsa.hhs.govLisa Murphy, VMD, DABTUniversity of Pennsylvania School of VeterinaryMedicine; NVRT-2murphylp@vet.upenn.eduChristopher Nelson, PhDRAND Corporationcnelson@rand.orgRobert D. PattersonMercy EMSRobert.Patterson@mercy.netPaul E. Petersen, PharmD, BCPSTennessee Department of HealthPaul.Petersen@tn.govNorm PlottVentura County Firenorm.plott@ventura.orgLeslie Porth, MPH, RNMissouri Hospital Associationlporth@mail.mhanet.comAnn Potter, RN, CEMWashington Hospital Centerannmpotter@earthlink.netMark Pottermapotter@earthlink.netTia Powell, MDAlbert Einstein College of MedicineMontefiore Medical Centertpowell@bioethics.org<strong>The</strong>rese QuinnSnohomish County Medical Reserve Corpstherese.quinn@snoco.orgCDR Paul Reed, MDDCVMRC/OSGPaul.Reed@hhs.govPaul Richter, MA, FASHE, CHEPVW International, Inc.prichter@scha.orgTeddy Rogers, MSA, NREMT-PNDMS/OPEO/ASPR; TN-1 DMATteddy.rogers@hhs.govChris Rosa, BA, ParamedicVentura County Emergency Medical ServicesChris.Rosa@ventura.orgMarc Rosenthal, DO, PhD, FACEPWayne State University; MI-1 DMATdrmsr@wayne.eduJohn Ryan, GACEMGeorgia Health Sciences Universityjfr.ryan@gmail.comVicki Sakata, MD, FACEP, FAAPUniversity of Washington School of Medicine/MultiCare Health Systems; WA-1 DMATvsakata@msn.comMitch Saruwatari, PhD, MPH, EMTLiveProcess, Inc.msaruwatari@liveprocess.comLCDR Samuel Schaffzin, MPACenters of Medicare & Medicaid ServicesSamuel.Schaffzin@cms.hhs.govJeffrey Schlegelmilch, MPH, MEPYale New Haven Center for Emergency<strong>Preparedness</strong> and Disaster ResponseJEFFREY.SCHLEGELMILCH@ynhh.orgCheryl Schmidt, PhD, RN, CNEUniversity of Arkansas for Medical SciencesCollege of NursingSchmidtCherylK@uams.eduMerritt Schreiber, PhDUniversity of California Irvine School of Medicine;CA-I DMATmds@uci.eduAngela M. Schuman, PharmDChildren’s Hospital Colorado; Childrens HospitalBoston; CO-3 DMATangela.mcintosh@childrenscolorado.orgDeAnne Seekins, MBADepartment of Veterans Affairsdeanne.seekins3@va.govPaul Severin, MD, FAAPStroger Hospital of Cook County/Rush UniversityMedical CenterPaul_J_Severin@rush.eduRobert Michael Shankman, GISPHHS/OS/ASPR/OPEORobert.Shankman@HHS.GOVLeatta ShipmanShoalwater Bay Indian Tribeleshipman@shoalwaterbay-nsn.govSara V. Sinclair, RN, LHFABear River Health Departmentssinclair@brhd.orgBrian Smith, MD, MPHTexas Department of State Health ServicesBrian.Smith@dshs.state.tx.usDale Smith, PhDUniformed Services University of the HealthServicesdcsmith@usuhs.milCharlotte Spires, DVM, MPH, DiplACVPMFDAcharlotte.spires@fda.hhs.govJanice Springer, RN, PHN, DNP(C)American Red CrossSpringerJa@usa.redcross.orgSharon Stanley, PhD, RN, BSAmerican Red CrossStanleyS@usa.redcross.orgSandra Stark Shields, LMFT, ATR-BC, CTSLos Angeles County Department of HealthServices, Emergency Medical Services Agency;CA-9 DMATsanshields@dhs.lacountyMardrah Starks-Robinson, BS, MPALouisiana Department of Health and Hospitalsmardrah.starks@la.gov<strong>2012</strong> Integrated Training Summit 71Presenters
PresentersKimberly StephensiDisaster.wordpress.com; Abt AssociatesKim26stephens@gmail.comCharles Stewart, MD, EMDM, MPHUniversity of Oklahoma; Oklahoma DisasterInstitute; OK-1 DMATcharles-e-stewart@ouhsc.eduBenita Stoddard, FACHEDepartment of Veterans AffairsBenita.Stoddard@va.govChristopher Sullivan, PhDImage Reseach, LLCchristophersullivanphd@comcast.netJon Surbeck, MA, CFO, IMTICOD Consulting Practitioner & ICvistap@lpbroadband.netRay Swienton, MD, FACEPNDLS-F, UTSWbeardogmd@aol.com<strong>The</strong>resa Wing Sze Tam, MBBS (UK), FRCPCPublic Health Agency of Canada<strong>The</strong>resa.Tam@phac-aspc.gc.caRegina Thomas, CBCPFreeman Health Systemrmthomas@freemanhealth.comShedale Tindall, MSN, RNDepartment of Veterans AffairsShedale.Tindall1@va.govDavid J. TorresHQ AETC/SGdavid.torres.12.ctr@us.af.milCAPT Rob Tosatto, PRh, MPH, MBAHHS/OS/OASH/OSG/DCVMRCrobert.tosatto@hhs.govCDR Anthony TranchitaGrand Forks Air Force Base Mental Health ClinicUnited States Air Forceanthony.tranchita.1@us.af.milTrina von Waldner, PharmD<strong>The</strong> University of Georgia College of Pharmacytvonwald@uga.eduDebra Wagner, CVA, NREMTOklahoma Medical Reservce Corps, OklahomaState Department of Healthdebramw@health.ok.govCatherine Witte, RPh, MdivIHScatherine.witte@ihs.govPresenters72<strong>2012</strong> Integrated Training Summit
Presenter DisclosuresAlliance between a speaker, planning memberand any commercial organization must bedisclosed for the purpose of determiningthe presence of bias or influence over theeducational content. <strong>The</strong>se disclosures, if any,are on file in the Chesapeake Health EducationProgram, Inc. office and may be reviewed by thetarget audience upon written request.<strong>The</strong>re are no commercial sponsors for the<strong>2012</strong> Integrated Medical, Public Health, <strong>Preparedness</strong>and Response Training SummitLinda Cashion, RN, MSToby Clairmont, RN, CHEPGarrick Clouden, MDCDR Jeff Coady, PsyDLT Christine Collins, RN, BSN, MAMary ConnellyChristina Conti, MPPA, BALCDR Meghan Corso, PsyDMarion Danis, MDDan Hanfling, MDCarly Hankins, BAJennifer HannahCynthia Hansen, PhDDarryl HardgeCAPT Ken Harman, MDLT COL Heidi Hastings, FACHEA.J. Heightman, MPA, EMT-PFred M. Henretig, MD<strong>The</strong> following presenters and / or planningmembers reported they have no relationshipswith commercial organization(s) to disclose:Jamie Davis, PhDCAPT Timothy Davis, MD, MPHCraig De Atley, PA-CJason E. Henry, RN, EMT, BAAntonio HernandezCAPT Steven Hirschfield, MD, PhDBrian Abrahamson, BACarl Adrianopoli, PhDPaul Clement Alleyne, MDDawn AnastasiaKnox Andress, RN, BA, ADDiane Angelico, RNJoseph H. Annelli, DVM, MDLindsey Anthony, MPA, CEMIsaac Ashkenazi, MD, MSc, MPACAPT Brad Austin, MPH, FACHEDennis Michael Baker, MA, LPCLT Jeffrey BallAllison Banger, MPHLeslie BeckBuddy BellCatherine Bennett, RN, MSAkiko Berkman, MPH, MPA, BSPaul Biedrzycki, MPH, MBAArnie Bierenbaum, MSCarolyn Blayney, RNMike Boucher, BSN, MSNSkip BowermanCAPT Sean M. Boyd, MPH, USPHSGary W. BrownJeff BryantNancy Carlson, BS, CFT, CFEPaul Carlton, Jr., MD, FACSMary Casey-Lockyer, RN, BSN,MHSLisa DeDecker, RN, MSCDR Patrick Denis, MBA, BSN, RNLeon Dent, MDMorgan DeWeese, BAAda Dieke, MPH, DrPH CCAPT Herman Allen Dobbs, MDJason Dobronz, FPEMJohn Donahue, BS, EMT-PDarrin DonatoErin Downey, MPH, ScDTony Dunford, RNCarrma Erickson-Hurt, APRN, ACHPNSandy Evans, RN, MPHTrish Factor, BS, MCHESMick FeeserSonda Finley, PHR, MBABarry Fisher, MPHAndrew Garrett, MD, MPHJane Garrett, BAJames Garrow, MPHBonnie Gaughan-BaileyMark Gentilman, OD, CEM, FACCPMAJ Micah GoettlGerardo GomezLori Gordon, DVMTimothy Grapes, MSRichard GreenKatie Hager, BSN, RNKathy HandraArchie HirschmannBen Ho, MDJudy Homer, RNJack HornerJerry Jaxx, DVM, ACLAMElleen Kane, MA, APRRachel KaulArthur Kellermann, MD, MPH, FACEPGerard R. Kelly, PhDLCDR Steven Kempton, CD, MMMAaron Kenneston, CEMDavid Kerschner, RN, MSNMary Alice King, MD, MPHScott Kirley, RRTHoward Klausner, MD, FACEPRADM Ann Knebel, RN, DNSc, FAANKathryn Koelemay, MD, MPHJimmy Koeninger, PhDDebra Kreisberg, PhDJoseph LamanaMike Lambert, EMT-P, AAAndre La PrairieTom Lawrence, NREMT-PThomas LehmanCAPT Mark Libby, RNNigel Lightfoot, MSc, FRCPath, FFPHGary LindberghLorie LiptakJill LittlefieldPresenter Disclosure<strong>2012</strong> Integrated Training Summit 73
Presenter DisclosuresPresenter DisclosureKevin Locke, MDRADM Boris Lushniak, MD, MPHDavid Marcozzi, MD, MHS-CL, FACEPGregg Margolis, PhD, NREMT-PThomas MacKayMary Massey, BSN, MA, MEPMarianne Matzo, PhD, FPCN, FAANJillian Maxwell, BAJeanne McBride, MS, BSKevin McCulleyBonnie McGuffinR. Doug Meckes, DVMGretchen MichaelCAPT A. Thomas Mignone, Jr., MPHGlenn Mitchell, MD, MPHMargaret R. Moon, MD, MPH, FAAPLCDR Tiffany Moore, RN, BSNJay MorrisCAPT David Morrissette, PhD, LCSWLisa Murphy, VMD, DABTChristopher Nelson, PhDLT Skip Payne, MSPH, REHS/RSRobert D. PattersonPaul E. Petersen, PharmD, BCPSGail Pfouts, RNNorm PlottJean Popiak Goodwin, DHA, PMPLeslie Porth, MPH, RNAnn Potter, RN, CEMMark PotterTia Powell, MDLCDR Johnnie Purify, MBA<strong>The</strong>rese QuinnCDR Paul Reed, MDTeddy Rogers, MSA, NREMT-PChris Rosa, BA, ParamedicMark Rosenthal, DO, PhD, FACEPJohn Ryan, GACEMVicki Sakata, MD, FACEP, FAAPHelga Scharf-Bell, MSN, RNLCDR Samuel Schaffzin, MPA74Jeffrey Schlegelmilch, MPH, MEPCheryl Schmidt, PhD, RN,CNEMerritt Schreiber, PhDAngela M. Schuman, PharmDDeAnne Seekins, MBAPaul Severin, MD, FAAPRobert Michael Shankman, GISPMoira Shea, MPALeatta ShipmanSara V. Sinclair, RN, LHFAKirsten Slowey, BABrian Smith, MD, MPHDale Smith, PhDCharlotte Spires, DVM, MPH, DiplACVPMJanice Springer, RN, PHN, DNP(C)Sharon Stanley, PhD, RN, BSSandra Stark Shields, LMFT, ATR-BC, CTSMadrah Starks-Robinson, BS, MPAKimberly StephensCharles Stewart, MD, EMDM, MPHBenita Stoddard, FACHEJon Surbeck, MA, CFO, IMTICRay Swienton, MD, FACEPBenjamin Swig, NREMT- B<strong>The</strong>resa Wing Sze Tam, MBBS (UK), FRCPCRegina Thomas, CBCPShedale Tindall, MSN, RNLauren ToomeyDavid J. TorresCAPT Rob Tosatto, PRh, MPH, MBACDR Anthony TranchitaCAPT Richard TurnerTrina von Waldner, PharmDDebra Wagner, CVA, NREMTDan Wall, RN, BSN, PANCatherine Witte, RPh, MdivCassandra WilsonApril Wood, BSN, RN, NREMT-B<strong>2012</strong> Integrated Training Summit<strong>The</strong> following presenters and / or planningmembers reported they have financial interest(s)/ arrangement(s) with one or more medicalcommercial organization(s).Jerry T. Anderson,BS, MS, CHEP reported heis employed by VWI, Inc as an EmergencyManagement ConsultantJef P. Bratberg, PharmD, BCPS reported he is amember of the speaker’s bureau for Merck, IncCharles Bauer, MD, CPE reported he is aconsultant for Panflu LLCJoseph Cocciardi, PhD, MS, CSP reported he is aconsultant for Cocciardi AssociatesMarie Kerl, DVM, MPH, DACVIM is on theSpeaker’s Bureau for Merck Animal HealthShannon Manzi, PharmD reported she will bediscussing off label use of pharmaceuticals forpediatric disaster patientsPaul Richter, MA, FASHE, CHEP, reported heis employed by VWI, Inc as an EmergencyManagement ConsultantMitch Saruwatari, PhD, MPH, EMT reported heis an employee of LiveProcess, Inc., a provider ofhealth care emergency management softwareChristopher Sullivan, PhD reported he is aconsultant with Bahia Consulting
<strong>2012</strong> Poster PresentationsMRCPoster 1MRC TRAIN: Preparing Public HealthProfessionals and Volunteers to ServeOur CommunitiesIlya Plotkin, MAPublic Health Foundationiplotkin@phf.orgMRCPoster 2K-SERV Credentialing andResource TrackingEmily NickelKansas Department of Health andEnvironmentenickel@kdheks.govMRCPoster 3MRC UniversityDavid Hopper, BAMacoupin County Medical Reserve Corpsdhopper@mcphd.netMRCPoster 43rd Annual Colorado Volunteer CapacityBuilding WorkshopKoral O’BrienColorado Department of Public Healthand Environmentkoral.obrien@gmail.comMRCPoster 5Integrated Training to Encourage anIntegrated ResponseJenifer Chatfield, DVMWest Central Florida Medical Reserve Corpsjen_chatfield@hotmail.comMRCPoster 6Medical Reserve Corps Partnership withLocal Community College in IndianaAmanda Stirratt, MPHIndiana State Department of Healthastirratt@isdh.in.govMRCPoster 7How Cameron County’s Medical Reserve Corp is Building Community Resilienceby Preparing Volunteers for Emergency Operations duringOperation Lone StarRoman Abeyta, MPHCameron County Department of Health and Human Servicesroman.abeyta@talho.orgFidel CalvilloCameron County Department of Health and Hman ServicesRaquel CastilloCameron County Department of Health and Human ServicesMRCPoster 8Understanding Willingness to VolunteerAmong Medical Reserve Corps VolunteersNicole Errett, MSPH, CPHJohns Hopkins Bloomberg School ofPublic Healthnerrett@jhsph.eduMRCPoster 9<strong>The</strong> Disaster Volunteer Predeployment(DVPrD) Structured InterviewThomas R. Thomson MEd, LPC, CPMOKMRC Stress Response Teamtrthomsonokc@gmail.comMRCPoster 10<strong>The</strong> Establishment of a Volunteer ForensicResponse Team in Chesterfield County,Virginia: A Pilot ProjectJon R. Donnelly, BAChesterfield (Virginia) HealthDistrict/Virginia Department of Healthjon.donnelly@vdh.virginia.govMRCPoster 11Regional Medical Reserve Corps StructureZumana Rios, MHAMultnomah County Health Departmentzumana.r.rios@multco.usPoster Presentations<strong>2012</strong> Integrated Training Summit 75
<strong>2012</strong> Poster PresentationsMRCPoster 12Sheltering Table Top ExerciseLiisa Karin JacksonMA Region 4A Public Health CoalitionLiisaJackson@comcast.netDoris MooreMA Region 4Amrc4a.doris@verizon.netMRCPoster 13<strong>The</strong> Mercer County Health DepartmentMedical Reserve Corps (MRC) and theHugh Jones Area Technical School HealthOccupation Students of America (HOSA)PartnershipStacy BlacketerMercer County Health Departmentstacyc.blacketer@ky.govMRCPoster 14Designing and Implementing a<strong>Preparedness</strong> and Response Curriculum ina Baccalaureate Nursing Program.Loren Stein, MSN, RNC-NICOklahoma University, College of Nursingloren-stein@ouhsc.eduCindy Rieger, APRN-CNSAdvanced Public Health NurseOklahoma University, College of NursingMRCPoster 15MRC and HOSA: Hand in Hand BuildingA Stronger CommunityStacy BlacketerMercer County MRCstacyc.blacketer@ky.govPatricia PrestonHOSAValencia HernandezHOSA/MRCKaylin GossHOSA/MRCMRCPoster 16Re-designing the Maryland Public Health & Medical Volunteer ProgramIsaac Ajit, MD, MPHOffice of <strong>Preparedness</strong> and Response, Maryland Department of Health and Mental HygieneIAjit@dhmh.state.md.usZachary Faigen, MSPHOffice of <strong>Preparedness</strong> and Response, Maryland Department of Health and Mental HygieneAnikah Salim, MPHOffice of <strong>Preparedness</strong> and Response, Maryland Department of Health and Mental HygieneSherry Adams, RNOffice of <strong>Preparedness</strong> and Response, Maryland Department of Health and Mental HygieneMRCPoster 17MRC Association Meeting PosterMike WeibelNational MRC Associationmweibel@brhd.orgMRCPoster 18Collaboration to CreatingCritical Capacity LocallyTerry ClarkMedical Reserve Corps Island Countyislandmrc@yahoo.comMRCPoster 19Developing a Medical Reserve Corp atLander University in Greenwood, SouthCarolinaRobbie Madden South, DHEd, MSN,APRN, PHCNS-BCLander Universityrsouth@lander.eduLeslie MacTaggert Myers, DNP,APRN, ANP-BCLander UniversityPoster PresentationsMRCPoster 20We’ve Got the Power!Pamela S. ToneyNorth Alabama Medical Reserve Corpsdirector@northalabamamrc.comBrooke RawlinsNorth Alabama Medical Reserve CorpsApplications in Response and <strong>Recovery</strong>Poster 21Impact of Electronic Medical Recordson Quality of Patient CareDivya SrinivasanGeorge Mason University,Cochrane Collaborationdivya5_s@hotmail.comApplications in Response and <strong>Recovery</strong>Poster 22Chemical, Radiological and NuclearMedical Countermeasure Developmentat BARDARonald G. Manning, PhDHHS/OS/ASPR/BARDAronald.manning@hhs.gov76<strong>2012</strong> Integrated Training Summit
<strong>2012</strong> Poster PresentationsApplications in Response and <strong>Recovery</strong>Poster 23Utilization ManagmentDonna K. Strong, MSN, RNUHPHS/Northen Navajo Medical Center (IHS)donna.strong@ihs.govApplications in Response and <strong>Recovery</strong>Poster 24Randomized Evaluation of Two MentalHealth Triage Tools in Medical ClearedDisaster Survivors by MRC Volunteers andPublic Health WorkersDonald E. Brannen, MHSA, MSGreene County Combined Health Districtdbrannen@gcchd.orgApplications in Response and <strong>Recovery</strong>Poster 25Using Geospatial Tools to Assist EmergencyPlanning, Response, and <strong>Recovery</strong>Daniel B. Koch, PhDOak Ridge National Laboratorykochdb@ornl.govPatricia W. Payne, MSPOak Ridge National LaboratoryApplications in Response and <strong>Recovery</strong>Poster 26On the Safe Side: Protecting Critical Infrastructure in Mass Causalty Incidents throughSite Security and Safety PlanningJohn J. Simkovich, DDS, MHASouth Carolina Department of Health and Environmental Control - Region 7simkovch@dhec.sc.govRaymond E. Barteet, Jr.South Carolina Department of Health and Environmental Control - Region 7Dana B. MilletSouth Carolina Department of Health and Environmental Control - Region 7Ann D. SportsSouth Carolina Department of Health and Environmental Control - Region 7Applications in Response and <strong>Recovery</strong>Poster 27<strong>The</strong> Creation and Evolution of the MemphisVA Medical Center Emergency MedicalResponse TeamJames PayneUS Dept of Veterans Affairs / VHA Officeof Emergencyjames.payne3@va.govPatrick S. Card, MBA, CCCPUS Dept of Veterans Affairs / Memphis VAMCApplications in Response and <strong>Recovery</strong>Poster 28San Francisco Bay Area Advanced PracticeCenter Presents: Assessment Methods forEmergency ResponseAdam Crawley, MPHUC Berkeley Center for Infectious Diseases &Emergency Readinessadam.w.crawley@gmail.comApplications in Response and <strong>Recovery</strong>Poster 29Triaging Resource Allocation for InpatientMovement (TRAIN)Brandon BondStanford University Medical Centerbbond@stanfordmed.orgRon Cohen, MDStanford University School of MedicineAnna Lin, MDLucile Packard Children’s HospitalApplications in Response and <strong>Recovery</strong>Poster 30Volunteer Management: Using Technologyto Manage Volunteer OperationsCarter Pittman, BS, EMT-PHamilton County Public HealthCarter.Pittman@hamilton-co.orgJared Warner, MEM, RSWarner <strong>Preparedness</strong> Services, LLCjwarner@warnerprep.comApplications in Response and <strong>Recovery</strong>Poster 31Emergency Registries: An ImportantTool for Your ToolboxJeffrey StevensRhode Island Department of HealthJeffrey.Stevens@health.ri.govApplications in Response and <strong>Recovery</strong>Poster 32Emergency <strong>Preparedness</strong>: EnhancingCommunication and Access to HealthInformation ResourcesDonna K. Sowles, RN, BS, EMT-PUpstate Medical Universitysowlesd@upstate.eduAnne E. Ryan, MS,RNUpstate Medical UniversityApplications in Response and <strong>Recovery</strong>Poster 33Developing and Using Pictograms inPublic Health <strong>Preparedness</strong> Operations:Recommendations and APC SolutionsBeth McGinnisMultnomah County Health Departmentbeth.mcginnis@multco.usPoster Presentations<strong>2012</strong> Integrated Training Summit 77
<strong>2012</strong> Poster PresentationsApplications in Response and <strong>Recovery</strong>Poster 34Harmful Stuff / Dangerous Goods (HS/DG)Recognition and Safety for First RespondersJames R, Overfleld, PhDPennyrile KY Health Districtj.overfield@mchsi.comApplications in Response and <strong>Recovery</strong>Poster 35Development and Evaluation of a NovelReal-time Mobile Telesonography SystemJ. FeldmanHackensack UMCmatildalandersson@gmail.comH. MorchelHackensack UMCC. OgedegbeHackensack UMCV. HazelwoodHackensack UMCApplications in Response and <strong>Recovery</strong>Poster 36CHEMM: A Comprehensive New Tool toManage Chemical Emergencies and MassCasulatiesJohn Koerner, MPH, CIHCBRNE Branch, HHS/ASPRjohn.koerner@hhs.govCollaboration and CoordinationPoster 37Partners Make A DifferenceDebra Davidson, PhDOzark Tri-County Consortium d/b/aACCESS Family Careddavidson@accessfamilycare.orgCollaboration and CoordinationPoster 38Leadership to Accomplish then IMPLEMENTa Three Decade Change: <strong>The</strong> American RedCross Disaster Health Services EnhancedResponse ModelSharon Stanley, PhD, RN, RSAmerican Red Crossstanleys@usa.redcross.orgMary Casey-Lockyer MHS, BSN, RN, CHSAmerican Red CrossCollaboration and CoordinationPoster 39Information Sharing: Adding Value forMedical and Public Health IntegrationHeather BrownU.S. Department of Homeland Security / Officeof Health AffairsHeather.N.Brown@dhs.govPaul StrangU.S. Department of Homeland Security / Officeof Health AffairsCollaboration and CoordinationPoster 40Integrating EMS into Public HealthInitiatives and Domestic <strong>Preparedness</strong>Collaboration and CoordinationPoster 41<strong>The</strong> Role of Librarians and Informationistsin Disaster ResponseCollaboration and CoordinationPoster 42Volunteer Integration: American Red Cross,National Student Nurse Program (NSNP)Richard Patrick, MS, CFO, EMT-P, FFDepartment of Homeland Security Office ofHealth AffairsRichard.Patrick@hq.dhs.govRichard Carr, MLS, AHIPUNM Health Science Library andInformatics CenterRCarr@salud.unm.eduBrian Bunnett, MLS, MA, AHIPUNM Health Sciences Library andInformatics CenterJanice Springer, RN, PHN, MA, DNP(c)springerja@usa.redcross.orgCheryl K Schmidt PhD, RN, CNE, ANEFUniversity of Arkansas for Medical SciencesCollege of NursingSharon A.R. Stanley, PhD, RN, RSAmerican Red CrossPoster PresentationsCollaboration and CoordinationPoster 43Effective Collaborations Between PublicHealth and Professional Associations forEmergency <strong>Preparedness</strong>Susan H. WebbMassachusetts Medical Societyswebb@mms.orgMichael Coughlin, MS, MAMA Department of Public HealthJohnna D. CogginMassachusetts Medical SocietyCollaboration and CoordinationPoster 44Community Immunity Point ofDispensing ProgramCheryl MurphyToledo-Lucas County Health Departmentmurphyc@co.lucas.oh.usStacy DeBruyne, MPHToledo-Lucas County Health DepartmentScott StrahlToledo-Lucas County Health DepartmentCollaboration and CoordinationPoster 45Building Sustainable Health Care Coalitionsin Rural and Small Metropolitan MissouriCommunitiesLeslie Porth, R.N., BSN, MPHMissouri Hospital Associationlporth@mail.mhanet.comJaclyn Gatz, MPAMissouri Hospital AssociationChris A Smith, MHA, MEP, CEASUniversity of Missouri Health Care78<strong>2012</strong> Integrated Training Summit
<strong>2012</strong> Poster PresentationsCollaboration and CoordinationPoster 46Hospital Readiness: Are you Truly Ready toRespond for that Pandemic?Robert Perry, RN, BSN, CENUniversity of New Mexico Hospital/NM-1Disaster Medical Assistance Teamrkkperry@hotmail.comCollaboration and CoordinationPoster 47Healthcare Coalition DevelopmentKerry DunnellBoston University School of Public Healthkdunnell@bu.eduTimothy M. McDonaldMassachusetts Department of Public HealthCollaboration and CoordinationPoster 48Best Practices in Leadership:A “Whole Community” Approach to AnimalEmergency ManagementAnne McCannUSDA / APHIS / Animal CareAnneliese.McCann@aphis.usda.govTy J. Vannieuwenhoven, DVM, MPHDACVPMCollaboration and CoordinationPoster 49<strong>The</strong> Role of Community Clinics and HealthCenters in Emergency First ResponseCollaboration and CoordinationPoster 50Community Hospital’s EvacuationDue to HurricaneCollaboration and CoordinationPoster 51Establishing A Modular DisasterMedical CenterJohn Michael Rendon, MPHCalifornia Primary Care Associationjrendon@cpca.orgRyan G Foster MS, RN, CNML, NEA-BCShore Health Systemrfoster@shorehealth.orgMark E. Gebhart, MDWright State Universitymark.gebhart@wright.eduCollaboration and CoordinationPoster 52Resiliency, Resources, andRegionalization: Addressing Challengesof Home Rule <strong>Through</strong> a CollaborativeRegionalization ProcessDebra Kreisberg, PhD<strong>The</strong> Center for Integrated Disaster <strong>Preparedness</strong>Debra.Kreisberg@UCDenver.eduMonyett Ellington,<strong>The</strong> Center for Integrated Disaster <strong>Preparedness</strong>,Department of Emergency MedicineSchool of Medicine, University of ColoradoDenverEducation and TrainingPoster 53Needs Analysis of Disaster MedicineTrainingCharles Stewart MD, EMDM, MPHUniversity of Oklahomacstew@storysmith.netEducation and TrainingPoster 54First Receiver Nurse Readiness toSupport Individual Readiness & InstitutionalCitizenship for Community Resilience inEmergenciesCathleen A. Evans, MSN, RN, CNE, CENAbington Memorial Hospital Dixon Schoolof Nursingcathyevans@verizon.netEducation and TrainingPoster 55A Concept Map to Promote Learning andKnowledge Capture <strong>from</strong> the U.S. EastCoast EarthquakeBrian A. Altman PhDNational Center for Disaster Medicine &Public Healthbrian.altman.ctr@usuhs.eduEducation and TrainingPoster 56Functional Needs Training Videos forVolunteers Assisting in Disaster SheltersDonna E Field Martin, AICP, MPHMid-America Regional Councildmartin@marc.orgEllen Gary, BSN, RNMedical Reserve Corps of Greater Kansas CityEducation and TrainingPoster 57Utilizing a “Code Sepsis” Team to ImproveOutcomes and Reduce MortalityDiane Fuller Switzer MN, ARNPHarborview Medical Center, University ofWashington, Seattle, Wa.dfswit@yahoo.comPoster Presentations<strong>2012</strong> Integrated Training Summit 79
<strong>2012</strong> Poster PresentationsEducation and TrainingPoster 58<strong>The</strong> Power of Stress:Staying in Optimal HealthEducation and TrainingPoster 59Lessons and Tools Developed <strong>from</strong> a StatewideHospital Evacuation Exercise ProgramEducation and TrainingPoster 60Effective Organization & Timely Delivery ofDMAT Team Member TrainingCarol Niemann MA, PC, LMHPDepartment of Corrections, Omaha, NE andMRC Eastern NE/Western IAcarol.niemann@nebraska.govPaul D. Biddinger,MD, FACEPMassachusetts General Hospital and HarvardSchool of Public Healthpbiddinger@partners.orgTimothy McDonaldMassachusetts Department of Public HealthEmergency <strong>Preparedness</strong> BureauRoberta Crawford, MEPMassachusetts Department of Public HealthEmergency <strong>Preparedness</strong> BureauKristen Kam McCowanCA-6 DMATkam@medsimkam.comSandra (Sam) BradleyCA-6 DMATEducation and TrainingPoster 61TEAM BUILDING: An Added Benefit of FieldTraining Exercise ParticipationEducation and TrainingPoster 62Operation Lone Star, An MPH StudentOverviewEducation and TrainingPoster 63Organizing and Training OrthopaedicSurgery Disaster Response VolunteersDiane KeaslerNDMS; AL-3 DMATdiane.keasler@hhs.govPaul Randy SmithNDMS; AL-3 DMATDave DiamondNY-2 DMATMontray Smith, MSN, RN, EMT-BUniversity of South Floridammsmith@mail.usf.eduChristopher T. Born, MD, FAAOS, FACSAmerican Academy Of Orthopaedic Surgeons/Orthopaedic Trauma Associationchristopher_born@brown.eduBruce Browner, MD, MS, FAAOS, FACSUniv. CT. Health Center-New England MusculoskeletalInstituteDavid Teuscher, MDBeaumont Bone & Joint InstituteEducation and TrainingPoster 64Nashville, TN ITS Mass Casualty IncidentCommand System (MCICS) ProposalJohn PuttOperational Consulting Groupjohnfputt@gmail.comRobert MarlinOperational Consulting GroupEducation and TrainingPoster 65WA-1 Vehicle Safety CourseMary Ditkoff PA-C, MPASNDMSmditkoff@msn.comEducation and TrainingPoster 66<strong>The</strong> Oregon AmeriCorps*VISTA/ MRC andAccreditation Partnership ProjectAlyssa BostianOregon Health Authortiy - Health Security<strong>Preparedness</strong> and Responsealyssa.bostian@state.or.usPoster PresentationsEducation and TrainingPoster 67Moulage – Bridging the Gap in SimulatedTraining ExercisesBobbie MericaMoulage Conceptsmoulageconcepts@sbcglobal.netEducation and TrainingPoster 68Hackensack University Medical Center’sMobile Rapid Response ProgramJ. FeldmanHackensack UMCmatildalandersson@gmail.comH. MorchelHackensack UMCC. OgedegbeHackensack UMCV. HazelwoodHackensack UMCEducation and TrainingPoster 69Enhance your Infectious Disease Detectionand Response Capacity with the BiosurveillanceSolutions and Infectious DiseaseEmergency Response ToolkitsHollie Lawyer, MPH, CHESSan Francisco Bay Area Advanced Practice Center/SanFrancisco Department of Public HealthHollie.Lawyer@sfdph.orgDean Lampman, MBASouthwest Center for Advanced Public HealthPractice /Tarrant County Public Health80<strong>2012</strong> Integrated Training Summit
<strong>2012</strong> Poster PresentationsEducation and TrainingPoster 70Designing, Implementing, and Evaluatinga Worksite Wellness Program for AndrewsCounty EmployeesJanice Arceneaux MS, RN, CMSRN<strong>The</strong> Centers for Medicare and Medicaid Servicesjanice.arceneaux@cms.hhs.govLessons Learned in Disaster ResponsePoster 71<strong>The</strong> Department of Veterans AffairsCaring for the NationCheryl Revis, AAS, CEMVeterans Health Administration Office ofEmergency Managementcheryl.revis@va.govLessons Learned in Disaster ResponsePoster 72Pandemic Readiness and Response Toolkit:Incorporates the Transitional MedicalModel (TMM), a Four Level Approach toPlanning, <strong>Preparedness</strong>, and ResponseGreg Moore, MBA, PMPToledo-Lucas County Health Departmentmooreg@co.lucas.oh.usEric Zgodzinski, MPH, RS, CPHToledo-Lucas County Health DepartmentStacy DeBruyne, MPHToledo-Lucas County Health DepartmentDrew Downing, MPHToledo-Lucas County Health DepartmentLessons Learned in Disaster ResponsePoster 73Ready or NotPhyllis Waits, EdD, MSN, RNJacksonville State Universitypwaits@jsu.eduKay Prickett, DSN, MSN, RNJacksonville State UniversityKim Craven, MSN, RNJacksonville State UniversityLessons Learned in Disaster ResponsePoster 74One Year Later: Implementing the LessonsLearned <strong>from</strong> FukushimaSterling ElliottWashington State Department of Healthselliott@astho.orgLessons Learned in Disaster ResponsePoster 75<strong>The</strong> Effects of the April 2011 TornadoOutbreak on Disaster <strong>Preparedness</strong> Trendsin Jefferson County, AlabamaLisa McCormick, DrPHUniversity of Alabama at Birmingham,School of Public Healthlmccormick@uab.eduJesse Pevear, MSPHAlabama Department of Public HealthLessons Learned in Disaster ResponsePoster 76Review of Public Health Event Case StudiesInvolving the Canada/US BorderAndre La PrairiePublic Health Agency of Canadaandre.laprairie@phac-aspc.gc.caLessons Learned in Disaster ResponsePoster 77Post Event Volunteer Registration Surge inMissouri’s ESAR-VHP Program: Show-MeResponseAnne Meredith Kyle, BSN, RNCenter for Emergency Response and Terrorism,Missouri Dept. of Health and Senior Servicesanne.kyle@health.mo.govLessons Learned in Disaster ResponsePoster 78Beyond the <strong>Preparedness</strong> Community:Lessons <strong>from</strong> Tohoku on the Need forGreater Community <strong>Preparedness</strong>Kristine Babbish, BAAmeriCorps*VISTA, Medical Reserve Corpskbabbish@co.linn.or.usLessons Learned in Disaster Response;Poster 79Sheltering-in-Place or Evacuation:A Hospital Case StudyRichard ZorasterLA County Emergency Medical Services Agencyrzoraster@dhs.lacounty.govJoe KeysLAC Olive View-UCLA Medical CenterResearch and ReviewPoster 80Evacuation Transportation ToolDevelopmentRichard ZorasterLA County Emergency Medical Services Agencyrzoraster@dhs.lacounty.govJoe KeysLAC Olive View-UCLA Medical CenterResearch and ReviewPoster 81Potential Tobacco Use and Its Effects on theMedical Clearance Process for ResponsePersonnelDebra Francince Kothman RRT, CTTSMiami Valley Hospital/DMAT OH-5gkothman@sbcglobal.netPoster Presentations<strong>2012</strong> Integrated Training Summit 81
<strong>2012</strong> Poster PresentationsResearch and ReviewPoster 82Preparing the Pharmacy Workforce toRespond to Public Health EmergenciesTrina von Waldner, BS, PharmD, RPhUniversity of Georgia College of Pharmacytvonwald@rx.uga.eduResearch and ReviewPoster 83Assessing Accuracy, Quality andEffectiveness of Medical CommunicationAmong First Responders andFirst ReceiversLee B. Smith, MD, JD, FACEPBureau for Public HealthLBSmith@hsc.wvu.eduResearch and ReviewPoster 84Framework of Challenges in InternationalMedical Response to DisastersAndre La PrairiePublic Health Agency of Canadaandre.laprairie@phac-aspc.gc.caResearch and ReviewPoster 85Exploring the Willingness to Report toWork during Pandemics among Health CareProfessionals in the Saudi Tertiary HospitalsSaad A. AlghanimKing Saud Universitysagksu@gmail.comResearch and ReviewPoster 86Success of Comprehensive AustereEnvironment and Operational MedicineCurriculum for Fourth YearMedical StudentsBryan Clardy MD, FAAFPUniversity of Arkansas for Medical Sciencesbhclardy@gmail.comResearch and ReviewPoster 87Clinical Presentations at Two DisasterMedical Assistance Team Sites:Post Hurricanes Gustav and Ike—Louisianaand Texas, 2008Rachel TormanHHS/ASPRrachel.torman@hhs.govResearch and ReviewPoster 88Deployment Perspectives:A Bird’s Eye ViewLaquitha Joyce MohairCenters for Medicare & Medicaid Services [CMS]laquitha.mohair@cms.hhs.govResearch and ReviewPoster 89Organizational Culture and CommunityHealth Outcomes during a Public HealthEmergencyDonald E. Brannen, MHSA, MSGreene County Combined Health Districtdbrannen@gcchd.orgResearch and ReviewPoster 90State <strong>Preparedness</strong>: A Study of State PlansZachary Fehrman, MPHClark County Combined Health Districtzackfehrman@yahoo.comPoster PresentationsSpecial Considerations in Emergency PlanningPoster 91Builidng Community Resilience forChildren and Families: <strong>The</strong> NationalChildren’s Disaster Mental Health Conceptof OperationsMerritt Dean SchreiberCenter for Disaster Medical Sciences,Department of Emergency Medicine,UC Irivne School of Medicinemds@uci.eduBetty Pfefferbaum, MD, JDUniversity of Oklahoma Health Sciences Centerand National Child Traumatic Stress NetworkSpecial Considerations in EmergencyPlanningPoster 92Planning for the Unique Evacuation andShelter-in-Place Needs of People withMedical Dependencies During a DisasterBrienne LenartYale: New Haven Health Center for Emergency<strong>Preparedness</strong> and Disaster Responsebrienne.lenart@ynhh.orgWilliam HalsteadYale: New Haven Health Center for Emergency<strong>Preparedness</strong> and Disaster ResponseSpecial Considerations in EmergencyPlanningPoster 93DHS Workforce Health & Medical Supportfor International DeploymentsIngrid Gail Hope, RN, MSNDHS/ Office of Health Affairsingrid.hope@dhs.govIvan A. Zapata, MS, CHESDHS - Office of Health Affairs82<strong>2012</strong> Integrated Training Summit
<strong>2012</strong> Poster PresentationsSpecial Considerations in EmergencyPlanningPoster 94How to Successfully Include Children inYour Hospital Mass Casualty DrillsSpecial Considerations in EmergencyPlanningPoster 95Pediatric Evacuation: Are you Ready toMove the Kids?Special Considerations in EmergencyPlanningPoster 96Kids On the Move: Special Considerationsfor the Movement of Pediatric PatientsDan KotzChildren’s Healthcare of Atlantadan.kotz@choa.orgStarla JonesChildren’s Healthcare of Atlanta atHughes SpaldingLiz Atkins, RNChildren’s Healthcare of Atlanta atEglestonMary Alice King MD, MPHHarborview Medical Center andSeattle Children’s, WAmaryking@u.washington.eduDanica LittleKing County Healthcare CoalitionAaron H. Gardner, MDHHS/ASPR/OPEO/ NDMS/OH-5 DMATaaronhgardner@gmail.comSpecial Considerations in EmergencyPlanningPoster 97Methadone and Evacuee Planning:Data Sharing for Optimal Patient CarePaul E PetersenTennessee Department of Health,Emergency <strong>Preparedness</strong> Programpaul.petersen@tn.govWesley Geminn, PharmDTennessee Department of Mental HealthJason Carter, PharmDTennessee Department of Mental healthSpecial Considerations in EmergencyPlanningPoster 98Registered and Ready: Creating a VirtualVolunteer Coordinating Center toRecruitVolunteers, Before, During and After aDisasterSusan Riedy, BSAlbany County Department of Healthsusan.riedy@albanycounty.comJill Dunkel, MS, MPAAlbany County Department of HealthSpecial Considerations in EmergencyPlanningPoster 99Considerations in Pediatric DisasterSurge - Mass Casualties, Critical Transportand the Technologically Dependent ChildElisabeth K Weber, RN, MA, CENChicago Department of Public Healthelisabeth.weber@cityofchicago.orgEvelyn Lyons, RN, MPHIllinois Department of Public HealthSpecial Considerations in EmergencyPlanningPoster 100Addressing the Psychosocial Needs ofChildren in DisastersKaren Olness, MDCase Western Reserve Universitykaren.olness@case.eduMarisa Herran, MDCase Western Reserve UniversitySpecial Considerations in Emergency PlanningPoster 101Utah Pediatric Disaster & MedicalResponse Teams-A Unique State Resourcefor <strong>Preparedness</strong> and the Management ofPediatric Disaster VictimsRichard Thomas, PharmD, DABATPrimary Children’s Medical Centerrichard.thomas@imail.orgBrent Kaziny, MD, MSUniversity of Utah, College of Medicine Divisionof Pediatric Emergency MedicineAlexander Cruz, BSN,RN,CEN,PM,MEPDepartment of Health, Bureau of EMSSpecial Considerations in EmergencyPlanningPoster 102What Lies Beneath: Local HealthDepartment Plans for a Mass Fatality EventMeredreth Maynard, BSN, RNTulsa Health Departmentmmaynard@tulsa-health.orgBrenda Dale, RN, MSMTulsa Health DepartmentSpecial Considerations in EmergencyPlanningPoster 103Including At-Risk Individuals andBehavioral Health in Emergency<strong>Preparedness</strong>, Response, and <strong>Recovery</strong>Olivia SparerHHS/ASPR/OPP/ABColivia.sparer@hhs.govCDR Harvey Ball, MS, CCC-SLPHHS/ASPR/OPP/ABCSpecial Considerations in EmergencyPlanningPoster 104Mental Health Resilience:A Collaborative ApproachAdela M. Rodriguez, LMSWNew York City Department of Health andMental HygieneArodrig3@health.nyc.govSpecial Considerations in EmergencyPlanningPoster 105Older Adults At Risk For NegativeOutcomes During Disaster Sheltering:What Does the Evidence Suggest?Jocelyn Anne Farrar RN, DNP, ACNP-BC,CCRNUniversity of Maryland School of Nursingjfarrar20@yahoo.comPoster Presentations<strong>2012</strong> Integrated Training Summit 83
<strong>2012</strong> Poster PresentationsSpecial Considerations in EmergencyPlanningPoster 106Low Birth Weight Babies and Very LowBirth Weight Babies in a Low ResourceEnvironmentJames L. Dickens, FNP-C, FAANPOASH/Office of Minority Healthjames.dickens@hhs.govSpecial Considerations in Emergency PlanningPoster 107Pediatric MCI Triage: Assessment ofProvider Performance in King County, WAKatherine Kenningham, MS-4University of Washington School of Medicinektmac85@uw.eduKathryn Koelemay, MD, MPHPublic Health - Seattle & King County, KingCounty Healthcare Coalition, UW School ofPublic HealthMary Alice King, MD, MPHHarborview Medical Center; University ofWashington; Seattle Children’s HospitalSpecial Considerations in Emergency PlanningPoster 108Preparing for Emergencies: VulnerablePopulations with Special Health Care NeedsDoris R. Varlese, JD<strong>The</strong> Mount Sinai Medical Centerdoris.varlese@mountsinai.orgPoster Presentations84<strong>2012</strong> Integrated Training Summit
Integrated Training Summit Acronym GuideAAAR/IPAEAHRQAmeriCorps*NCCCAmeriCorps*VISTAAPHISAPODAPOEARESARTASHASPRBBIABRACCC&OCCCCCCDCCDRGCERTCHCSCHEPCHEP.IncCOCOMCONOPSCONPLANCOSINCPXCRICSTDDARTDASFDCCPRDEMDESTDFODHSDMATDMORTDOCDoDDOEDOHDOIDOJDOLAfter Action Report / Improvement PlanAero-EvacuationAgency for Healthcare Research and QualityAmeriCorps*National CivilianCommunity CorpsAmeriCorps*Volunteers in Serviceto AmericaAnimal and Plant Health Inspection ServiceAerial Ports of DebarkationAerial Ports of EmbarkationAmateur Radio Emergency ServicesAssessment and Response TeamAssistant Secretary for HealthAssistant Secretary for <strong>Preparedness</strong> andResponseBureau of Indian AffairsBioterrorism Response Advisory CommitteeConcepts and ObjectivesCommissioned CorpsCitizen Corps CouncilsCenters for Disease Control and PreventionCatastrophic Disaster Response GroupCommunity Emergency Response TeamChairman of the Joint Chiefs of StaffCertified Healthcare Emergency ProfessionalChesapeake Health Education Program, Inc.Combatant CommandConcept of the OperationsU.S. Government Interagency DomesticTerrorism Concept of Operations PlanControl Staff InstructionsCommand Post ExerciseCities Readiness InitiativeCivil Support TeamDisaster Assistance Response TeamDisaster Aero Medical Staging FacilityDivision of Commissioned Corps Personnel andReadiness (including former Office of ForceReadiness and Deployment)Department of Emergency ManagementDomestic Emergency Support TeamDisaster Field OfficeDepartment of Homeland SecurityDisaster Medical Assistance TeamDisaster Mortuary Operational Response TeamDepartment of CommerceDepartment of DefenseDepartment of EnergyState Departments of HealthDepartment of InteriorDepartment of JusticeDepartment of LaborDOSDOTDPADPODSCADSCADTRIMEEEGsEMAEMACEMSEMSEMSEOCEPAERCERCGERTERT-AERT-NDepartment of StateDepartment of TransportationDefense Protection ActDistribution Proccess OwnerDefense Support of Civil AuthoritiesDefense Support of Civil AuthoritiesDomestic Threat Reduction and IncidentManagementExercise Evaluation GuidesEmergency Management AgencyEmergency Management Assistance CompactEmergency Medical SystemEmergency Medical ServicesEmergency Management SystemEmergency Operations CentersEnvironmental Protection AgencyEmergency Response CoordinatorEmergency Response Coordination GroupEmergency Response TeamEmergency Response Team-AdvancedEmergency Response Team-NationalESAR-VHP Emergency System for Advance Registration ofVolunteer Health ProfessionalsESF#8 Emergency Support Function #8EXPLANFFBIFCCFCCFDAFECCFEMAFERCFESCFIRSTFMCFNSFOCFPCFPSFRCMFRERPFRPFSAFTXGGISGSAHHANHETCHHSHRSAExercise PlanFederal Bureau of InvestigationFederal Communications CommissionFederal Coordinating CenterFood and Drug AdministrationFederal Emergency CommunicationsCoordinatorFederal Emergency Management AgencyFEMA Emergency Response CapabilityFederal Emergency Support CoordinatorFederal Incident Response Support TeamFederal Mobilization CenterFood and Nutrition ServiceFEMA Operations CenterFinal Planning ConferenceFederal Protection ServiceFEMA Regional Communications ManagerFederal Radiological Emergency Response PlanFederal Response PlanFarm Service AgencyField Training ExerciseGeographical Information SystemGeneral Services AdministrationHealth Alert NetworkHealth Education Training CenterDepartment of Health and Human ServicesHealth Resources and Services AdministrationHSASHSCHSEEPHSOCHSPDHUDIIHSIIMGIMTINRPIPRIRCTJJELCJFOJICJISJOCJPMTJPRTJTFJTTFLEPCLTACLTCMHomeland Security Advisory SystemHomeland Security CouncilHomeland Security Exercise and EvaluationProgramHomeland Security Operations CenterHomeland Security Presidential DirectiveDepartment of Housing and UrbanDevelopmentIndian Health ServiceInteragency Incident Management GroupIncident Management TeamInitial National Response PlanIn Progress ReviewIncident Response Coordination TeamJoint Exercise Life CycleJoint Field OfficeJoint Information CenterJoint Information SystemJoint Operations CenterJoint Patient Movement TeamJoint Patient Reporting TeamJoint Task ForceJoint Terrorism Task ForceLocal Emergency Planning CommitteeLong Term Acute CareLong Term CareMA-2 Massachusetts 2MACMACCMAC-STMassMAPMMRSMPCMRCMRTENNACCHONAHERCNASANAWASNCCNCCDPHNCEHNCIDNCPNCSNCTCNDMSEntity Multi-agency Coordinating EntityMulti-agency Command CenterMobile Acute Care Strike TeamMassachusetts Mutual Aid PlanMetropolitan Medical Response SystemMid Planning ConferenceMedical Reserve CorpsMedical Readiness, Training, and EducationcommitteeNational Association of County and City HealthOfficialsNational Animal Health Emergency ResponseCorpsNational Aeronautics and Space AdministrationNational Warning SystemNational Coordinating CenterNational Center for Chronic Disease Preventionand Health PromotionNational Center for Environmental HealthNational Center for Infectious DiseaseNational Oil and Hazardous SubstancesPollution Contingency PlanNational Communications SystemNational Counterterrorism CenterNational Disaster Medical SystemITS Acronym Guide<strong>2012</strong> Integrated Training Summit 85
Integrated Training Summit Acronym GuideITS Acronym GuideNEDSSNEEPNEPNGANGBNHCNHSUNICNICCNICCLNIFCNIHNIMSNIPPNIRTNISACNJTTFNMRTN-NCNOAANOCNPSNRCNRCCNRCSNRPNRTNSANSCNSPNTIANVOADNVRTNWCGNWRNWSOOASHOEMOEROFRDOGHAOIAOIGAOMBOPEOOPHPNational Electronic Disease Surveillance SystemNational Exercise and Evaluation ProgramNational Exercise ProgramNational Geospatial Intelligence AgencyNational Guard BureauNational Hurricane CenterNational Homeland Security UniversityNIMS Integration CenterNational Infrastructure Coordinating Center/National Interagency Coordination CenterNational Incident CommunicationsConference LineNational Interagency Fire CenterNational Institutes of HealthNational Incident Management SystemNational Infrastructure Protection PlanNuclear Incident Response TeamNational Infrastructure Simulation & AnalysisCenterNational Joint Terrorism Task ForceNational Medical Response TeamNORAD – NorthCOMNational Oceanic and AtmosphericAdministrationNational Operations CenterNational Park ServiceNuclear Regulatory CommissionNational Response Coordination CenterNatural Resources Conservation ServiceNational Response PlanNational Response TeamNational Security AgencyNational Security CouncilNational Search and Rescue PlanNational Telecommunications and InformationAdministrationNational Voluntary Organizations Active inDisasterNational Veterinary Response TeamNational Wildlife Coordinating GroupNOAA Weather RadioNational Weather ServicesOffice of the Assistant Secretary for HealthOffice of Emergency ManagementOffice of Emergency ResponseOffice of Force Readiness and Deployment(now the Division of Commissioned CorpsPersonnel and Readiness {DCCPR})Office of Global Health AffairsOffice of the Assistant Secretary for InformationAnalysisOffice of Intergovernmental AffairsOffice of Management and BudgetOffice of <strong>Preparedness</strong> and EmergencyOperationsOffice of Public Health <strong>Preparedness</strong>OSOSGOSHAOSLGCPPPCCPDDPHSPMPM SATRRACESRAMPRCPRCRARHARISCRMCCROCRRCCRRTSSCCSEMOSIMCENSIOCSITMANSLPPSLPSSNSSTARTSTARTEXTTCCOffice of the SecretaryOffice of the Surgeon GeneralOccupational Safety and Health AdministrationOffice of State and Local GovernmentCoordination and <strong>Preparedness</strong>Policy Coordination CommitteePresidential Decision DirectivePublic Health ServicePatient MovementPatient Movement Situational Awareness TeamRadio Amateur Communications for EmergencyServicesRemedial Action Management ProgramRegional Contingency PlanResource Conservation and <strong>Recovery</strong> ActRegional Health AdministratorRegional Interagency Steering CommitteeRegional Medical Coordinating CenterRegional Operations CenterRegional Response Coordination CenterRegional Response TeamSecretary’s Command Center (HHS)State Emergency Management OfficeNational Exercise Simulation CenterStrategic Information and Operations CenterSituation ManualState and Local <strong>Preparedness</strong> ProgramState and Local Programs and SupportDirectorateStrategic National StockpileScientific and Technical Advisory and ResponseTeamStart of ExerciseUSTRANSCOM Component CommandTCH 11 Turbo Challenge 2011TELLTSATSCUUASITraining, Exercises, Lessons LearnedTransportation Security AdministrationTerrorist Screening CenterUrban Area Security InitiativeUC 11 Ultimate Caduceuc 2011US&RUSACEUSCGUSDAUSJFCOMUSNORTHCOMUSPHSUSSSUSTCUSTranscomUrban Search and RescueU.S. Army Corps of EngineersU.S. Coast GuardU.S. Department of AgricultureUnited States Joint Forces CommandUnited States Northern CommandUnited States Public Health ServiceU.S. Secret ServiceU.S. Transportation CommandUnited States Transportation CommandVVAVAMCDepartment of Veteran AffairsVeterans Affairs Medical Center86<strong>2012</strong> Integrated Training Summit