Medical History Form - Intermountain Healthcare
Medical History Form - Intermountain Healthcare
Medical History Form - Intermountain Healthcare

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
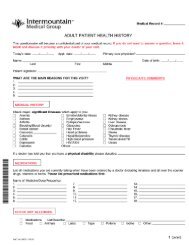
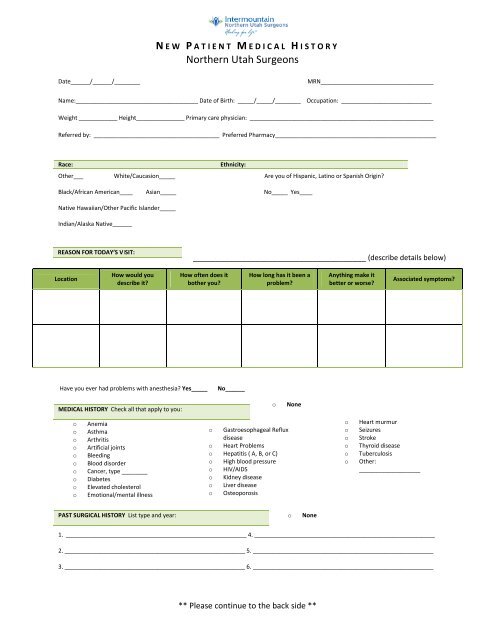
N E W P A T I E N T M E D I C A L H I S T O R YNorthern Utah SurgeonsDate______/______/________MRN___________________________________Name:______________________________________ Date of Birth: _____/_____/________ Occupation: ____________________________Weight ____________ Height_______________ Primary care physician: _________________________________________________________Referred by: _______________________________________ Preferred Pharmacy__________________________________________________Race:Ethnicity:Other___ White/Caucasion_____ Are you of Hispanic, Latino or Spanish Origin?Black/African American____ Asian_____ No_____ Yes____Native Hawaiian/Other Pacific Islander_____Indian/Alaska Native______REASON FOR TODAY’S VISIT:_______________________________________ (describe details below)LocationHow would youdescribe it?How often does itbother you?How long has it been aproblem?Anything make itbetter or worse?Associated symptoms?Have you ever had problems with anesthesia? Yes_____No______MEDICAL HISTORY Check all that apply to you:oNoneooooooooooAnemiaAsthmaArthritisArtificial jointsBleedingBlood disorderCancer, type ________DiabetesElevated cholesterolEmotional/mental illnesso Gastroesophageal Refluxdiseaseo Heart Problemso Hepatitis ( A, B, or C)o High blood pressureo HIV/AIDSo Kidney diseaseo Liver diseaseo OsteoporosisooooooHeart murmurSeizuresStrokeThyroid diseaseTuberculosisOther:___________________PAST SURGICAL HISTORY List type and year:oNone1. ________________________________________________________ 4. ________________________________________________________2. ________________________________________________________ 5. ________________________________________________________3. ________________________________________________________ 6. ________________________________________________________** Please continue to the back side **
ALLERGIES Check all that apply:oNoneoMedications (reaction): ________________________________________________________________o Other: _____________________________________________________________________________MEDICATIONS List all medications currently taking:1. _______________________________________________________2.________________________________________________________ooCheck here if the computer list isaccurate or if you have attached a copyof your med list3.________________________________________________________ 6. _______________________________________________________4.________________________________________________________ 7. ________________________________________________________5. ________________________________________________________ 8. ________________________________________________________FAMILY HISTORY Check those that apply:oooNoneFamily history of trouble with anesthesia.Family history of bleeding problems or easy bleedingFamily history of cancers . If yes what type/location __________________________________SOCIAL HISTORY Please fill out:Do you smoke cigarettes? Yes______ No______ How much do you smoke? _______ packs per day for______ years.Do you drink alcohol? Yes ______ No ______Have you ever used illegal drugs? Yes ______ No ______REVIEW OF SYSTEMS Check any condition(s) that apply to you, all others negative:Constitutionalo Recent weight losso Feverso Severe fatigueEyeso Double visiono Change in visionEars, Nose, Throat, Moutho Hearing losso Nasal congestiono Sore throato Trouble Swallowingo Hoarsenesso Mouth soresHematologico Easy bleedingo Bloody urine / stoolCardiovascularo Chest pain or anginao Heart attacko Leg Swellingo High Blood Pressureo Irregular heartbeatRespiratory/Lungso Persistent cougho Shortness of breatho Wheezingo Snoringo Stop breathing at nightGastrointestinalo Heartburn / indigestiono Nausea/vomitingo Abdominal paino Jaundiceo HepatitisGenitourinaryo Prostate problemso Burning or painful urinationMusculoskeletalo Joint paino Weakness in arms/legso Joint swelling/stiffnessNeurologicalo Numbness or tinglingo Severe headachesAllergic/Immunologico Sneezingo Itchy eyes/noseo Itchy throato Skin rasho HIVThe above information is accurate to the best of my knowledge:Reviewed by:Patient SignatureDateV 10.5.10