Veterinary fees claim form - The Co-operative Insurance
Veterinary fees claim form - The Co-operative Insurance
Veterinary fees claim form - The Co-operative Insurance
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
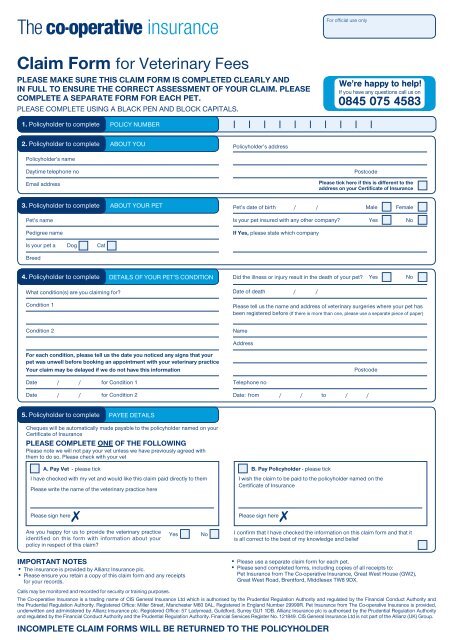
For official use onlyClaim Form for <strong>Veterinary</strong> Feesplease make sure this <strong>claim</strong> <strong>form</strong> is completed clearly andIN FULL TO ensure the correct assessment of your <strong>claim</strong>. please<strong>Co</strong>mplete a separate <strong>form</strong> for each pet.Please COMPLETE using A black pen AND block capitals.We’re happy to help!If you have any questions call us on0845 075 45831. Policyholder to complete POLICY NUMBER2. Policyholder to complete ABOUT YOUPolicyholder’s addressPolicyholder’s nameDaytime telephone noEmail addressPostcodePlease tick here if this is different to theaddress on your Certificate of <strong>Insurance</strong>3. Policyholder to complete ABOUT YOUR PET Male FemalePet’s date of birth / /Pet’s nameIs your pet insured with any other company?YesNoPedigree nameIf Yes, please state which companyIs your pet a Dog CatBreed4. Policyholder to complete DETAILS OF YOUR PET’S CONDITIONDid the illness or injury result in the death of your pet?YesNoWhat condition(s) are you <strong>claim</strong>ing for?Date of death / /<strong>Co</strong>ndition 1Please tell us the name and address of veterinary surgeries where your pet hasbeen registered before (If there is more than one, please use a separate piece of paper)<strong>Co</strong>ndition 2NameAddressFor each condition, please tell us the date you noticed any signs that yourpet was unwell before booking an appointment with your veterinary practiceYour <strong>claim</strong> may be delayed if we do not have this in<strong>form</strong>ationPostcodeDate / / for <strong>Co</strong>ndition 1Date / / for <strong>Co</strong>ndition 2Telephone noDate: from / / to / /5. Policyholder to complete PAYEE DETAILSCheques will be automatically made payable to the policyholder named on yourCertificate of <strong>Insurance</strong>PLEASE COMPLETE ONE OF THE FOLLOWINGPlease note we will not pay your vet unless we have previously agreed withthem to do so. Please check with your vetA. Pay Vet - please tickI have checked with my vet and would like this <strong>claim</strong> paid directly to themPlease write the name of the veterinary practice hereB. Pay Policyholder - please tickI wish the <strong>claim</strong> to be paid to the policyholder named on theCertificate of <strong>Insurance</strong>Please sign here7Please sign here7Are you happy for us to provide the veterinary practiceidentified on this <strong>form</strong> with in<strong>form</strong>ation about yourpolicy in respect of this <strong>claim</strong>?YesNoI confirm that I have checked the in<strong>form</strong>ation on this <strong>claim</strong> <strong>form</strong> and that itis all correct to the best of my knowledge and beliefImportant notes• <strong>The</strong> insurance is provided by Allianz <strong>Insurance</strong> plc.• Please ensure you retain a copy of this <strong>claim</strong> <strong>form</strong> and any receiptsfor your records.• Please use a separate <strong>claim</strong> <strong>form</strong> for each pet.• Please send completed <strong>form</strong>s, including copies of all receipts to:Pet <strong>Insurance</strong> from <strong>The</strong> <strong>Co</strong>-<strong>operative</strong> <strong>Insurance</strong>, Great West House (GW2),Great West Road, Brentford, Middlesex TW8 9DX.Calls may be monitored and recorded for security or training purposes.<strong>The</strong> <strong>Co</strong>-<strong>operative</strong> <strong>Insurance</strong> is a trading name of CIS General <strong>Insurance</strong> Ltd which is authorised by the Prudential Regulation Authority and regulated by the Financial <strong>Co</strong>nduct Authority andthe Prudential Regulation Authority. Registered Office: Miller Street, Manchester M60 0AL. Registered in England Number 29999R. Pet <strong>Insurance</strong> from <strong>The</strong> <strong>Co</strong>-<strong>operative</strong> <strong>Insurance</strong> is provided,underwritten and administered by Allianz <strong>Insurance</strong> plc. Registered Office: 57 Ladymead, Guildford, Surrey GU1 1DB. Allianz <strong>Insurance</strong> plc is authorised by the Prudential Regulation Authorityand regulated by the Financial <strong>Co</strong>nduct Authority and the Prudential Regulation Authority. Financial Services Register No. 121849. CIS General <strong>Insurance</strong> Ltd is not part of the Allianz (UK) Group.incomplete Claim FORMS will be returned to THE POLICYHOLDER5042 <strong>Co</strong>-Op Vet Fees CF 8123-3.indd 1 24/02/2014 14:27
ASK your vet to complete these THREE sections6. Vet to completeGENERAL INFORMATIONWhen was this pet first registered at your practice? / /If this pet has been referred please give the name, address and telephonenumber of the practice which referred itNameAddressTelephone noIn connection with treatment <strong>claim</strong>ed did you:If Yes, were the pet’s vaccinations up to date at time of treatment?Please give dateYes of last vaccination / / No Don’t knowIs any part of this <strong>claim</strong> for dental treatment?If Yes, please enclose a full clinical history over the last 2 years. If this is notattached this will delay the client’s <strong>claim</strong>Is any part of this <strong>claim</strong> for treatment of a urinary problem?If Yes, is the cost of diet food included in this <strong>claim</strong>?If Yes, please provide the name of the diet food being used and total costbeing <strong>claim</strong>edYesYesYesNoNoNoMake a house visit?YesNoNameAmount £ -Or provide out of hours treatment?YesNoWere crystals present?YesNoIf Yes, why was the house visit/out of hours treatment necessary?If Yes, are the crystalsIf other, please specifyOxalate Struvite OtherPlease give dates and results of last two urine testsDate / / ResultIs any part of this <strong>claim</strong> for a condition the pet can bevaccinated against?YesNoDate / / Result7. Vet to complete ABOUT THE ILLNESS OR INJURY<strong>Co</strong>ndition 1Name of the illness or injury (if no diagnosis has been made please give clinical signs)7. Vet to complete ABOUT THE ILLNESS OR INJURY<strong>Co</strong>ndition 2 (If relevant)Name of the illness or injury (if no diagnosis has been made please give clinical signs)Is this <strong>claim</strong> a continuation?YesNoIs this <strong>claim</strong> a continuation?YesNoWhen did this illness or injury begin (as noted on your records)? / /When did this illness or injury begin (as noted on your records)? / /Treatment dates:from / / to / /Treatment dates:from / / to / /Did death or euthanasia result from this illness or injury?YesNoDid death or euthanasia result from this illness or injury?YesNoDate of death / /Date of death / /If the pet was put to sleep, did you recommend this?YesNoIf the pet was put to sleep, did you recommend this?YesNoTo your knowledge has this pet been seen before for:To your knowledge has this pet been seen before for:This illness or injuryYesNoThis illness or injuryYesNoAny similar or related illness or injuryYesNoAny similar or related illness or injuryYesNoAny similar or related clinical signsYesNoAny similar or related clinical signsYesNoIf Yes, please provide the history with dates?If Yes, please provide the history with dates?Date / /Date / /Date / /Date / /Total amount <strong>claim</strong>ed (inc VAT)£ -Total amount <strong>claim</strong>ed (inc VAT)£ -Please enclose full invoices to support this <strong>claim</strong>Please enclose full invoices to support this <strong>claim</strong>8. Vet to complete DECLARATION BY THE VETERINARY PRACTICEVet stampThis practice is authorised to have <strong>claim</strong>s paid directYesNoI have checked the in<strong>form</strong>ation on this <strong>claim</strong> <strong>form</strong> and confirm that it is all correctto the best of my knowledge and beliefNamePosition in practiceEmail addressSignature7Date / /incomplete Claim FORMS will be returned to THE POLICYHOLDER 8123/3 03.145042 <strong>Co</strong>-Op Vet Fees CF 8123-3.indd 2 24/02/2014 14:27