
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
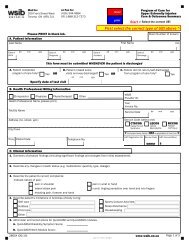
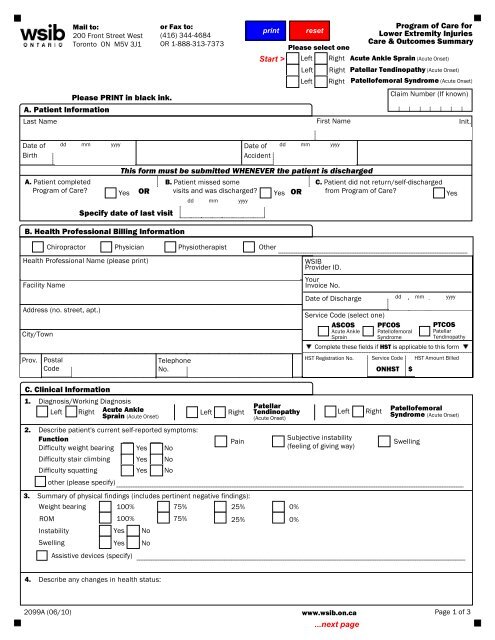
Mail to:200 Front Street WestToronto ON M5V 3J1Please PRINT in black ink.A. Patient InformationLast Nameor Fax to:(416) 344-4684OR 1-888-313-7373Program of <strong>Care</strong> forLower Extremity InjuriesPlease select one<strong>Care</strong> & <strong>Outcomes</strong> <strong>Summary</strong>Left Right Acute Ankle Sprain (Acute Onset)Left Right Patellar Tendinopathy (Acute Onset)Left Right Patellofemoral Syndrome (Acute Onset)First NameClaim Number (If known)Init.Date ofBirthdd mm yyyy Date of dd mm yyyyAccidentA. Patient completedProgram of <strong>Care</strong>?This form must be submitted WHENEVER the patient is dischargedB. Patient missed someC. Patient did not return/self-dischargedYes OR visits and was discharged? Yes OR from Program of <strong>Care</strong>?YesSpecify date of last visitB. Health Professional Billing Informationdd mm yyyyChiropractor Physician Physiotherapist OtherHealth Professional Name (please print)Facility NameAddress (no. street, apt.)City/TownProv.PostalCodeWSIBProvider ID.YourInvoice No.Date of DischargeService Code (select one)ASCOS PFCOSAcute Ankle PatellofemoralSprainSyndromedd mm yyyyPTCOSPatellarTendinopathyComplete these fields if HST is applicable to this formHST Registration No. Service Code HST Amount BilledTelephoneNo. ONHST $C. Clinical Information1. Diagnosis/Working DiagnosisLeft Right Acute AnkleLeft RightSprain (Acute Onset)PatellarTendinopathy(Acute Onset)2. Describe patient's current self-reported symptoms:Function Subjective instabilityPainDifficulty weight bearing Yes No(feeling of giving way)SwellingDifficulty stair climbing Yes NoDifficulty squatting Yes Noother (please specify)3. <strong>Summary</strong> of physical findings (includes pertinent negative findings):Weight bearing 100% 75% 25% 0%ROM 100% 75%25% 0%InstabilityYes NoSwelling Yes NoAssistive devices (specify)LeftRightPatellofemoralSyndrome (Acute Onset)4. Describe any changes in health status:2099A (06/10)www.<strong>wsib</strong>.on.caPage 1 of 3
Patient's Last NameDate ofBirthFirst NameProgram of <strong>Care</strong> forLower Extremity Injuries<strong>Care</strong> & <strong>Outcomes</strong> <strong>Summary</strong>dd mm yyyy Date ofdd mm yyyy Claim Number (If known)AccidentC. Clinical Information (continued)5. Describe patient's limitations in Activities of Daily Living:Child careHousekeepingSleep disturbanceOther6. Administer and record scores for the:A. Lower Extremity Functional Scale (LEFS) /80B. Numeric Pain Rating Scale (NPRS) /10HobbiesSelf careSports/Leisure Activities(e.g. no pain =0 worst possible pain =10)7. What level of pre-injury function has the worker attained? 100% 75% 50% 25%8. Are there any complicating factors that may delay recovery: Yes NoIf Yes, identify:Believes hurt equals harm Home environment concerns Prefers passive treatmentsLow mood/social withdrawal Work environment concerns Other:Fears/avoids activity9. Are there outstanding recovery issues? Yes NoIf Yes, specify:What is your recommendation to resolve these issues? What progress has been made to address these issues?10. Indicate if additional treatment(s)/assessment(s) or referral(s) are required: NoYesIndicate treatment(s) recommended:D. Return To Work Information11. Did patient losetime from work?YesNoIf Yes,indicate dates:FromDatedd mm yyyy To dd mm yyyyDate12. Patient's current employment status: How long do you anticipate before the patientA. Full time OR Part time workercan return to full and unrestricted work?B. Regular duties OR Modified dutiesC. Regular hours OR Modified hoursdays13. Describe the patient's functional limitations:A. No LimitationsB. Limitations (please specify)Comments:Bending/twistingKneelingSittingWalkingClimbing stairs/ladders LiftingStanding Walking on uneven groundOther:14. Has patient made contact with the employer since the injury: Yes No15. Indicate type of contact you had with the employer: Verbal Written NoneWhere no contact has been made, please indicate reason:Could notreachDid not receivecall backContactnot initiated2099A2 Page 2 of 3
Patient's Last NameDate ofAccidentFirst NameProgram of <strong>Care</strong> forLower Extremity Injuries<strong>Care</strong> & <strong>Outcomes</strong> <strong>Summary</strong>dd mm yyyyDate ofdd mm yyyy Claim Number (If known)BirthE. <strong>Summary</strong> of <strong>Care</strong> DeliveredMark (x) in corresponding box for each Program of <strong>Care</strong>component delivered.16. Acute Ankle Sprain (AS)Program of <strong>Care</strong> Interventions Supported by EvidenceWeeks1 - 301 cryotherapy02 manipulation03 passive joint mobilization04 proprioception/functional training05 range of motion and strengthening exercisesProgram WeeksWeeks4 - 8Other Interventions Not Supported by Evidence and Not Recommended06 laser therapy07 prolonged immobilization (for greater than 72 hours)08 ultrasoundIndicate total number of treatment visits Weeks 4 - 8Weeks 1 - 317.Patellar Tendinopathy (PT)Program of <strong>Care</strong> Interventions Supported by EvidenceWeeks1 - 6Weeks7 - 1209 therapeutic exerciseOther Interventions Not Supported by Evidence and Not Recommended10 friction or ultrasound11 deep transverse friction massageIndicate total number of treatment visits Weeks 1 - 6Weeks 7 - 1218.Patellofemoral Syndrome (PF)Program of <strong>Care</strong> Interventions Supported by EvidenceWeeks1 - 6Weeks7 - 1212 therapeutic exercise13 mobilization14 acupunctureOther Interventions Not Supported by Evidence and Not Recommended15 deep transverse friction massage for iliotibial band syndrome16 McConnell Regimen17 taping18 ultrasoundIndicate total number of treatment visits Weeks 7 - 12Weeks 1 - 6It is an offense to knowingly make a false or misleading statement or representation to the Workplace Safety andInsurance Board (WSIB). I hereby declare that the information being submitted is true and complete.Health Professional's Signature Date: dd mm yyyy2099A3 Page 3 of 3