Request for Prescription Information or Change Form
Request for Prescription Information or Change Form
Request for Prescription Information or Change Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
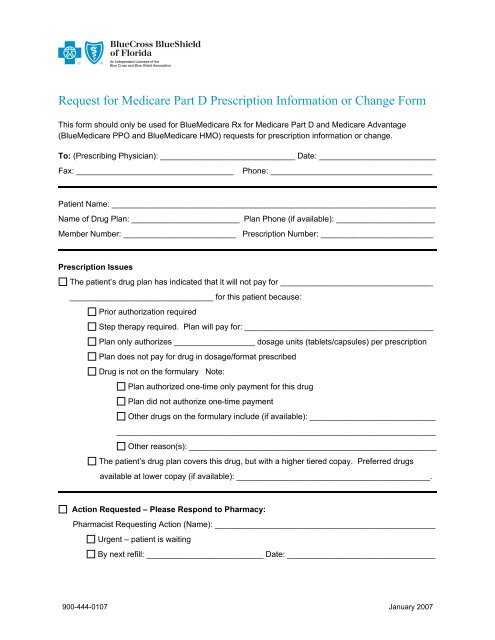
<strong>Request</strong> <strong>f<strong>or</strong></strong> Medicare Part D <strong>Prescription</strong> In<strong>f<strong>or</strong></strong>mation <strong>or</strong> <strong>Change</strong> F<strong>or</strong>mThis <strong>f<strong>or</strong></strong>m should only be used <strong>f<strong>or</strong></strong> BlueMedicare Rx <strong>f<strong>or</strong></strong> Medicare Part D and Medicare Advantage(BlueMedicare PPO and BlueMedicare HMO) requests <strong>f<strong>or</strong></strong> prescription in<strong>f<strong>or</strong></strong>mation <strong>or</strong> change.To: (Prescribing Physician): ______________________________ Date: __________________________Fax: ___________________________________Phone: ____________________________________Patient Name: ________________________________________________________________________Name of Drug Plan: ________________________ Plan Phone (if available): ______________________Member Number: _________________________ <strong>Prescription</strong> Number: _________________________<strong>Prescription</strong> IssuesThe patient’s drug plan has indicated that it will not pay <strong>f<strong>or</strong></strong> __________________________________________________________________ <strong>f<strong>or</strong></strong> this patient because:Pri<strong>or</strong> auth<strong>or</strong>ization requiredStep therapy required. Plan will pay <strong>f<strong>or</strong></strong>: __________________________________________Plan only auth<strong>or</strong>izes __________________ dosage units (tablets/capsules) per prescriptionPlan does not pay <strong>f<strong>or</strong></strong> drug in dosage/<strong>f<strong>or</strong></strong>mat prescribedDrug is not on the <strong>f<strong>or</strong></strong>mulary Note:Plan auth<strong>or</strong>ized one-time only payment <strong>f<strong>or</strong></strong> this drugPlan did not auth<strong>or</strong>ize one-time paymentOther drugs on the <strong>f<strong>or</strong></strong>mulary include (if available): ___________________________________________________________________________________________________Other reason(s): _______________________________________________________The patient’s drug plan covers this drug, but with a higher tiered copay. Preferred drugsavailable at lower copay (if available): ___________________________________________.Action <strong>Request</strong>ed – Please Respond to Pharmacy:Pharmacist <strong>Request</strong>ing Action (Name): _________________________________________________Urgent – patient is waitingBy next refill: __________________________ Date: _________________________________900-444-0107 January 2007
Provide alternative medication: __________________________________________________Other recommended action: ____________________________________________________Physician Signature: ________________________________ Date: _____________________________Action <strong>Request</strong>ed – Contact Drug Plan to <strong>Request</strong>: pri<strong>or</strong> auth<strong>or</strong>ization <strong>f<strong>or</strong></strong>mulary exceptionIn<strong>f<strong>or</strong></strong>mation Only – No Immediate Action NecessaryPlease Note: Medicare Part D does not pay <strong>f<strong>or</strong></strong> barbiturates, benzodiazepines, fertility drugs, drugs <strong>f<strong>or</strong></strong> weight loss <strong>or</strong>weight gain, drugs <strong>f<strong>or</strong></strong> hair growth, over-the-counter drugs, <strong>or</strong> prescription vitamins (except prenatal vitamins andflu<strong>or</strong>ide preparations).From: Pharmacy Name: ________________________________________________________________Fax: ______________________ Phone: ______________________ Email: ______________________Address: ____________________________________________________________________________In<strong>f<strong>or</strong></strong>mation on this <strong>f<strong>or</strong></strong>m is protected health in<strong>f<strong>or</strong></strong>mation and subject to all privacy and security regulations underHIPAA. Use of this <strong>f<strong>or</strong></strong>m is end<strong>or</strong>sed by the Alzheimer’s Association, American Medical Association, AmericanPharmacists Association, Center <strong>f<strong>or</strong></strong> Medicare Advocacy, Medical Group management Association, NationalCommunity Pharmacists Association and the National Council on the Aging.The Centers <strong>f<strong>or</strong></strong> Medicare & Medicaid Services has reviewed this fax <strong>f<strong>or</strong></strong>m, but does not require its use. Use of the<strong>f<strong>or</strong></strong>m <strong>f<strong>or</strong></strong> communications between pharmacists and physicians is voluntary. It is not a legal document. The officialMedicare program provisions are contained in relevant laws, regulations, and rulings.900-444-0107 January 2007