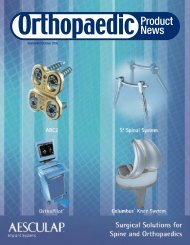
EXECUTIVE INTERVIEWcontinued from page 16complexity. We’ve kept it simple. The Kinectiv Technologyimplants and instrumentation have been designed with significantconsultation from surgeons, O.R. personnel and sales representatives.Our goal was a streamlined, simple option for bothsurgeon and patient. Our sole use of the +0 heads gives the systemthat simplicity and eliminates the need for multiple head lengths,complicated charts and head size limitations. We have been quitepleased by the response from surgeons and O.R. teams who havefound that the intuitive and readily apparent 4mm leg length andoffset adjustments help improve operative flow.OPN: Zimmer isn’t the first to develop a mobile bearing knee implant.Why a new generation of mobile bearing knees?HP: There have been several generations of mobile bearingimplants, and as an industry we’ve learned that, for certainpatient demographics, a mobile bearing option can provide amore natural range of motion. As the market leader in total kneearthroplasty, we feel it’s imperative to offer a solution for this marketsegment that builds on the clinical legacy of our NexGen <strong>Knee</strong>System while offering unique and value added technologies. Thenext step is improving upon patient satisfaction and the implantfunction and performance expectations. To this end, the NexGenLPS-Flex Mobile Bearing <strong>Knee</strong> System (See Exhibit 4.) wasdesigned to accomplish three main goals: (1) to restore naturalkinematics, (2) to accommodate safe flexion to 155˚, and (3) toenable surgeons to utilize Minimally Invasive Solutions procedures.Exhibit 4: The NexGen LPS-Flex Mobile Bearing <strong>Knee</strong> System.HP: The NexGen LPS-Flex Mobile Bearing <strong>Knee</strong> System was theresult of our analysis of the effects and component interactionsthat result when knee prostheses undergo deep flexion, beyond120˚. Zimmer’s design allows for safe high flexion as the posteriorcondyles roll back up to 155˚. This higher flexion meets theneeds of patients with active daily living, leisure or work activities,as well as patients whose culture or social customs dictate frequentkneeling or sitting cross-legged.Antecedent mobile bearing designs have failed to address seriousfunctional limitations arising from the kinematics of kneerotation. The problem with competing mobile bearing implantsarises from the central location of the pivot point on the tibialbaseplate.Zimmer has designed the NexGen LPS-Flex Mobile Bearing<strong>Knee</strong> with an anterior pivot (See Exhibit 5.), which is where bodymechanics tell us it should be – near the anterior cruciate ligamentsite. Anterior pivoting replicates the anatomic center of rotationand reduces patellofemoral forces. 8-11 Patellofemoral forces alsoincrease with greater medial/lateral displacement, which researchhas implicated in post-surgical anterior knee pain. Reduction inpatellofemoral forces could reduce patellar complications such aspatellar dislocation, component wear, damage and loosening. 8,9 Ananterior stop on the tibial baseplate effectively prevents the “spinout”seen in competing implants and noted in the literature. 12,13 Inregards to design features which facilitate minimally invasive surgicalapproaches, the height of the anterior trunnion is only10mm, which in combination with our “mini keel” tibial baseplate(See Exhibit 6.) reduces the need for tibial subluxation to insert thecomponents. Another key feature is Zimmer’s enhanced PScam/spine mechanism which, unlike most PS systems, drivesdown the spine of the articular surface, increasing resistance tosubluxation.Exhibit 5: The NexGen LPS-Flex Mobile Bearing <strong>Knee</strong>System with an anteriorpivot point.OPN: Tell us more about the benefits of the NexGen LPS-Flex MobileBearing <strong>Knee</strong>.OPN: Some companies claim that bone conservation is a key factor inhigh-flex knee implants. These companies criticize femoral designs suchas the LPS-Flex because an additional 2mm of bone must be removedfrom the posterior condyles compared to the standard femoral designs.HP: While bone conservation is always important, Zimmerresearch has shown the removal of an additional 2mm of bone isrequired to optimize the tibiofemoral contact area (See Exhibit 7.)continued on page 1918 ORTHOPAEDIC PRODUCT NEWS • November/December 2009
EXECUTIVE INTERVIEWcontinued from page 18Exhibit 6: Mini keel tibial baseplate.HP: The NexGen Mobile Bearing <strong>Knee</strong> flexibly accommodates differentsurgical styles, and can be accomplished through a minimallyinvasive procedure which results in smaller incisions, lessblood loss and less pain. The Zimmer Multi-Reference® 4-in-1Instrumentation allows for a measured resection technique.Alternatively, the Zimmer Minimally Invasive SolutionsIntramedullary Instrumentation accommodates a tibia-first, flexionbalancing approach. Regardless of the surgical technique, thisprecise instrumentation allows surgeons to adjust and controlalignment prior to performing any bone cuts.OPN: What’s next for Zimmer?throughout the entire range of motion. An implant system thatprovides a greater tibiofemoral contact area during high flexioncan help minimize the possibility of edge loading, and therebyreduce the likelihood of the metal condyle “digging” into thearticular surface when the knee is flexed beyond 125˚. 14 On theNexGen LPS-Flex implants, this was accomplished by extendingthe radius of the posterior femoral condyles so the contact arearemains high in deep flexion.Exhibit 7: Research shows the removal of an additional 2mm of bone isrequired to optimize the tibiofemoral contact area throughout the entirerange of motion.To extend the radius, the posterior condyles are slightly thicker,which also increases the posterior condylar offset, and thusreduces the chance of impingement of the femoral shaft on the tibialarticular surface. 15 Some competitors, such as the StrykerTriathlon <strong>Knee</strong>, for example, claim to be “high-flex friendly.”However, our own head-to-head research has shown that theTriathlon <strong>Knee</strong> has significantly less contact area when comparedto the NexGen Flex Implants at high flexion angles between 125˚and 155˚. 14OPN: Let’s talk about the procedure. What kind of instrumentation andprocedure options are there for surgeons in implanting the NexGenMobile Bearing <strong>Knee</strong>?HP: We are currently developing new products and technologiesacross all of our reconstructive lines, with some exciting offeringscoming out of the extremities category, as well as knees and hips.We are also continuing to build our global spine, trauma and dentalbusinesses. As we continue to grow across all divisions, we arealso investing in orthobiologic technologies and advanced materials,allowing us to address more of the continuum of care for jointdisease.MM: In parallel with our innovations in orthopaedic solutions, wewill continue to expand our offerings at the Zimmer Institute,which is setting the standard in the industry for personalized andhands-on surgical training.References1. Noble PC, Box GG, Kamaric E, Fink MJ, Alexander JW, Tullos HS. The effectof aging on the shape of the proximal femur. Clin Orthop. 1995;316:31-44.2. Maruyama M, Feinberg JR, Capello WN, D’Antonio JA. Morphologic features ofthe acetabulum and femur: anteversion angle and implant positioning. ClinOrthop. 2001;393:52-65.3. Data from Mohamed Mahfouz, Ph.D., University of Tennessee Center forMusculoskeletal Research. Femoral Bone Atlas.4. Data on file at Zimmer.5. Sugano N, Noble PC, Kamaric E. Predicting the position of the femoral headcenter. J Arthroplasty. 1999;14:102-107.6. Dorr LD, Long WT, Inaba Y, Sirianni L, Boutary M. MIS total hip replacementwith a single posterior approach. Seminars in Arthroplasty. 2005;16:179-185.7. Malik A, Maheshwari A, Dorr LD. Impingement with total hip replacement. JBone Joint Surg. 2007;89:1832-1842.8. Smith AJ, et al. Pre-surgery knee joint loading patterns during walking predictthe presence and severity of anterior knee pain after total knee arthroplasty. JOrthop Res. Number 22, pp 26-266. 20049. Browne C, et al. Patellofemoral forces after total knee arthroplasty: effect ofextensor moment arm. <strong>Knee</strong>. Number 12, pp 81-88. 2005.10. Scuderi GR et al. In vivo kinematic evaluation and design considerations relatedto high flexion in total knee arthroplasty. J Biomech. Number 38, pp 277-284. 200511. Hollister AM, et al. The Axes of Rotation of the <strong>Knee</strong>. Clin Orthop Relat Res.Number 290, pp 259-268. 199312. Stiehl JB. Clinical results and complications in mobile bearing total kneearthroplasty. Instr Course Lect 2005;55:233.13. Thompson N.W., Wilson DS, Cran GW, et al. Dislocation of the rotating platformafter low contact stress total knee arthroplasty. Clin Orthop. 2004;425:207.14. Data on file at Zimmer.15. Bellemans J, Banks S, Victor J, Vandenneucker H, Moemans A. Fluoroscopicanalysis of the kinematics of deep flexion in total knee arthroplasty: influence ofposterior condylar offset. J Bone Joint Surg (Br). 2002; 84-B(1):50-53.For more information, please contact CRM@zimmer.com.Note: All trademarks are the property of their respective owners.November/December 2009 • ORTHOPAEDIC PRODUCT NEWS 19