Instructor Trainer - Lifesaving Society
Instructor Trainer - Lifesaving Society
Instructor Trainer - Lifesaving Society
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
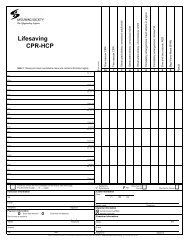
1<strong>Instructor</strong> <strong>Trainer</strong>Side 1: Please print each candidate's name and contact information legibly.Sex MFDate of BirthY/M/DPrerequisites Checked<strong>Lifesaving</strong> <strong>Society</strong>1TeachingCommunicationClass ManagementPlanningEvaluation2 3 4 5 6ResultNameAddressCityPostal codeE-mail2NameTelephoneSex M FAddressCityPostal codeE-mail3NameTelephoneSex M FAddressCityPostal codeE-mail4NameTelephoneSex M FAddressCityPostal codeE-mail5NameTelephoneSex M FAddressCityPostal codeE-mail6NameTelephoneSex M FAddressCityPostal codeE-mailBranch <strong>Trainer</strong>'s NameCheck box if there are more candidates on the reverse side of this page.This test sheet is page ___ of ___ pages.Branch <strong>Trainer</strong> InformationTelephoneID# Satisfactory PerformanceClinic InformationStart Date:F FailTotal Pass forClinicEnd Date:Total Fail for ClinicYY MM DD YY MM DDE-mail( )Telephone SignatureBranch <strong>Trainer</strong>'s NameE-mail( )Telephone SignaturAwards informationAwards issued by affiliateAwards not issuedID#Facility namePayment informationExam fees attachedExam fees not attachedSend invoice or receipt toAffiliateAddressReturn completed test sheet to the <strong>Lifesaving</strong> <strong>Society</strong> Branch Office promptly after the exam. Retain one copy for your records. Do not sent cash by mail.( )Telephone( )TelephoneCity Province Postal code
<strong>Instructor</strong> <strong>Trainer</strong>Side 2: Please print each candidate's name and contact information legibly.Date of BirthPrerequisites Checked<strong>Lifesaving</strong> <strong>Society</strong>TeachingCommunicationClass ManagementY/M/D 1 2 3 4Planning5Evaluation6Result7Sex MFNameAddressCityPostal codeE-mail8NameTelephoneSex M FAddressCityPostal codeE-mail9NameTelephoneSex M FAddressCityPostal codeE-mail10NameTelephoneSex M FAddressCityPostal codeE-mail11NameTelephoneSex M FAddressCityPostal codeE-mail12NameTelephoneSex M FAddressCityPostal codeE-mailTelephoneCheck box if there are more candidates on the reverse side of this page.This test sheet is page ___ of ___ pages.Clinic Information Satisfactory PerformanceBranch <strong>Trainer</strong> InformationF FailTotal Pass forClinicTotal Fail for ClinicStart Date:End Date:YY MM DDYY MM DDBranch <strong>Trainer</strong>'s NameID#( )name TelephoneE-mail( )TelephoneSignaturePlease complete Branch<strong>Trainer</strong>, Awards and Payment information sections on Side 1 of test sheet. Hostname, Clinic information, and Branch <strong>Trainer</strong> sections must be completed on both sides 1 and 2 of thetest sheet.Branch <strong>Trainer</strong>'s NameE-mailID#( )TelephoneSignatureReturn completed test sheet to the <strong>Lifesaving</strong> <strong>Society</strong> Branch Office promptly after the exam. Retain one copy for your records. Do not sent cash by mail.