JSTA December 2010 - Australian Association of Stomal Therapy ...
JSTA December 2010 - Australian Association of Stomal Therapy ...
JSTA December 2010 - Australian Association of Stomal Therapy ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
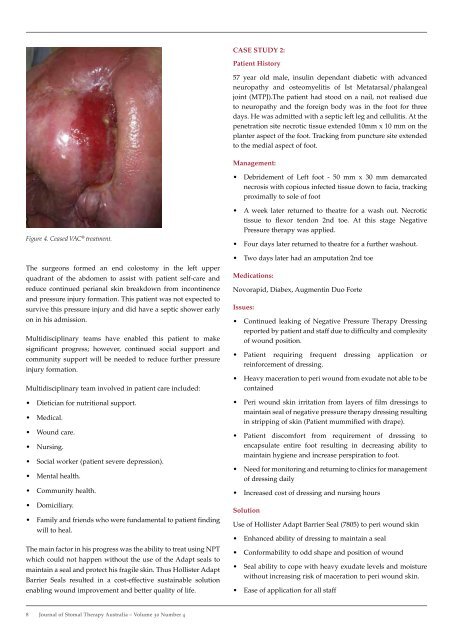
Figure 4. Ceased VAC ® treatment.<br />
The surgeons formed an end colostomy in the left upper<br />
quadrant <strong>of</strong> the abdomen to assist with patient self-care and<br />
reduce continued perianal skin breakdown from incontinence<br />
and pressure injury formation. This patient was not expected to<br />
survive this pressure injury and did have a septic shower early<br />
on in his admission.<br />
Multidisciplinary teams have enabled this patient to make<br />
significant progress; however, continued social support and<br />
community support will be needed to reduce further pressure<br />
injury formation.<br />
Multidisciplinary team involved in patient care included:<br />
• Dietician for nutritional support.<br />
• Medical.<br />
• Wound care.<br />
• Nursing.<br />
• Social worker (patient severe depression).<br />
• Mental health.<br />
• Community health.<br />
• Domiciliary.<br />
• Family and friends who were fundamental to patient finding<br />
will to heal.<br />
The main factor in his progress was the ability to treat using NPT<br />
which could not happen without the use <strong>of</strong> the Adapt seals to<br />
maintain a seal and protect his fragile skin. Thus Hollister Adapt<br />
Barrier Seals resulted in a cost-effective sustainable solution<br />
enabling wound improvement and better quality <strong>of</strong> life.<br />
8 Journal <strong>of</strong> <strong>Stomal</strong> therapy australia – Volume 30 Number 4<br />
cASe STudy 2:<br />
Patient History<br />
57 year old male, insulin dependant diabetic with advanced<br />
neuropathy and osteomyelitis <strong>of</strong> Ist Metatarsal/phalangeal<br />
joint (MTPJ).The patient had stood on a nail, not realised due<br />
to neuropathy and the foreign body was in the foot for three<br />
days. He was admitted with a septic left leg and cellulitis. At the<br />
penetration site necrotic tissue extended 10mm x 10 mm on the<br />
planter aspect <strong>of</strong> the foot. Tracking from puncture site extended<br />
to the medial aspect <strong>of</strong> foot.<br />
Management:<br />
• Debridement <strong>of</strong> Left foot - 50 mm x 30 mm demarcated<br />
necrosis with copious infected tissue down to facia, tracking<br />
proximally to sole <strong>of</strong> foot<br />
• A week later returned to theatre for a wash out. Necrotic<br />
tissue to flexor tendon 2nd toe. At this stage Negative<br />
Pressure therapy was applied.<br />
• Four days later returned to theatre for a further washout.<br />
• Two days later had an amputation 2nd toe<br />
Medications:<br />
Novorapid, Diabex, Augmentin Duo Forte<br />
Issues:<br />
• Continued leaking <strong>of</strong> Negative Pressure <strong>Therapy</strong> Dressing<br />
reported by patient and staff due to difficulty and complexity<br />
<strong>of</strong> wound position.<br />
• Patient requiring frequent dressing application or<br />
reinforcement <strong>of</strong> dressing.<br />
• Heavy maceration to peri wound from exudate not able to be<br />
contained<br />
• Peri wound skin irritation from layers <strong>of</strong> film dressings to<br />
maintain seal <strong>of</strong> negative pressure therapy dressing resulting<br />
in stripping <strong>of</strong> skin (Patient mummified with drape).<br />
• Patient discomfort from requirement <strong>of</strong> dressing to<br />
encapsulate entire foot resulting in decreasing ability to<br />
maintain hygiene and increase perspiration to foot.<br />
• Need for monitoring and returning to clinics for management<br />
<strong>of</strong> dressing daily<br />
• Increased cost <strong>of</strong> dressing and nursing hours<br />
Solution<br />
Use <strong>of</strong> Hollister Adapt Barrier Seal (7805) to peri wound skin<br />
• Enhanced ability <strong>of</strong> dressing to maintain a seal<br />
• Conformability to odd shape and position <strong>of</strong> wound<br />
• Seal ability to cope with heavy exudate levels and moisture<br />
without increasing risk <strong>of</strong> maceration to peri wound skin.<br />
• Ease <strong>of</strong> application for all staff