149 Kimura's Disease - JK Science
149 Kimura's Disease - JK Science
149 Kimura's Disease - JK Science

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
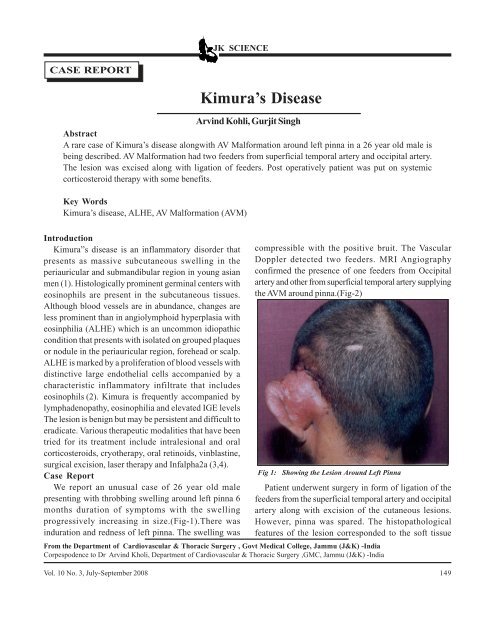
<strong>JK</strong> SCIENCECASE REPORTArvind Kohli, Gurjit SinghAbstractA rare case of Kimura’s disease alongwith AV Malformation around left pinna in a 26 year old male isbeing described. AV Malformation had two feeders from superficial temporal artery and occipital artery.The lesion was excised along with ligation of feeders. Post operatively patient was put on systemiccorticosteroid therapy with some benefits.Key WordsKimura’s disease, ALHE, AV Malformation (AVM)Kimura’s <strong>Disease</strong>IntroductionKimura”s disease is an inflammatory disorder thatpresents as massive subcutaneous swelling in theperiauricular and submandibular region in young asianmen (1). Histologically prominent germinal centers witheosinophils are present in the subcutaneous tissues.Although blood vessels are in abundance, changes areless prominent than in angiolymphoid hyperplasia witheosinphilia (ALHE) which is an uncommon idiopathiccondition that presents with isolated on grouped plaquesor nodule in the periauricular region, forehead or scalp.ALHE is marked by a proliferation of blood vessels withdistinctive large endothelial cells accompanied by acharacteristic inflammatory infiltrate that includeseosinophils (2). Kimura is frequently accompanied bylymphadenopathy, eosinophilia and elevated IGE levelsThe lesion is benign but may be persistent and difficult toeradicate. Various therapeutic modalities that have beentried for its treatment include intralesional and oralcorticosteroids, cryotherapy, oral retinoids, vinblastine,surgical excision, laser therapy and Infalpha2a (3,4).Case ReportWe report an unusual case of 26 year old malepresenting with throbbing swelling around left pinna 6months duration of symptoms with the swellingprogressively increasing in size.(Fig-1).There wasinduration and redness of left pinna. The swelling wascompressible with the positive bruit. The VascularDoppler detected two feeders. MRI Angiographyconfirmed the presence of one feeders from Occipitalartery and other from superficial temporal artery supplyingthe AVM around pinna.(Fig-2)Fig 1: Showing the Lesion Around Left PinnaPatient underwent surgery in form of ligation of thefeeders from the superficial temporal artery and occipitalartery along with excision of the cutaneous lesions.However, pinna was spared. The histopathologicalfeatures of the lesion corresponded to the soft tissueFrom the Department of Cardiovascular & Thoracic Surgery , Govt Medical College, Jammu (J&K) -IndiaCorpespodence to Dr Arvind Kholi, Department of Cardiovascular & Thoracic Surgery ,GMC, Jammu (J&K) -IndiaVol. 10 No. 3, July-September 2008 <strong>149</strong>
<strong>JK</strong> SCIENCEangiomatosis with accompanying lymphoid hyperplasiawith reactive germinal center formation and Eosinophiliasuggestive of Kimura’s disease. (Fig- 3) Post operativelypatient was put on systemic corticosteroid therapywith some benefit.Fig-2: MRI Showing The AVM Around Pinna With FeedersFrom Occipital and ST ArteryDiscussionLu (5) in a comparative study of 12cases comparedKimura:s disease(KD) with epitheloid hemangioma(EH)KD represented a lymphoid hyperplasia and EH a benignvascular tumor. Patient in our case had clinicopathologicalfeatures of KD but associated with AV malformationaround left pinna, Chan KM (6) has reported case ofKimura’s disease of the auricle Misago N (7 ) reportedan unusual case of arteriovenous (AV) malformation(localized form of soft tissue angiomatosis): a reactionof angiolymphoid hyperplasia with eosinophilia (ALHE)developed over the lesion of this pre-existing AVmalformation. However in our patient there were definitevascular feeders from occipital and superficial temporalartery along with histological features suggestive ofKimura’S disease a combination which is unparalleled inscreened litreature.Fig -3: Angiomatosis With Lymphoid Hyperplasia With ReactiveGerminal Center Formation &Esinophilia ( HXE- 400)The treatment of Kimura”s disease isprobelematicSurgical resection has been found to becurative although recurrence is common (4). Localizedinitial regrowth can be managed with surgical excision,other therapeutic options include radiation, systemiccorticosteroids Cytotoxic agents,cyclosporin andpentoxyfiline Systemic steroids may be indicated infrequent relapses or cases complicated by nephroticsyndrome, Sato S et al (8) has suggested combined useof steroids with cyclosporine with good response in apatient Radiation may be considered in cases refractoryto surgical and medical therapyReferences1 Chun SI. Kimura”s disease and ALHE with eosinophilia.J Am Acad Dermatol 1992,27;9542 Odam RB,James DW,.Berger G T. Andrew’s <strong>Disease</strong>s ofthe skin,clinical dermatology WB Saunders 2000 .pp.7473 Armstrong WB,Allison G, Pena F et al .Kimura;sdisease;two case reports and a literature review.Ann OtolRhinol Laryngol 1998;107;1066-714 Day TA,Abreo F,Hoajsoe DK, et al .Treatment of kimura’sdisease;a therauptic enigma.Otolaryngol Head NeckSurg1995;112;333-375 Lu L,Chen RG,Li XQ,Wang J.Kimura’s disease andepitheloid hemangioma;a comparative study of 12 cases.Zhonghua Bing Li Xue Za Zhi 2005; 34;353-576 Chan KM,Mok JS,Ng SK et al. Kimura,s disease of theauricle. Otolaryngol Head Neck Surg 2001;124;598-997. Misago N Tanaka T Kodera H et al. Localized soft tissueangiomatosis with subsequent development ofangiolymphoid hyperplasia with eosinophilia. J Dermatol1999 ;26:48-558 Sato S Kawashima H Kuboshima S et al . Combinedtreatment of steroids and Cyclosporin in Kimura”s disease.Paed 2006 ;118(3):921-23.150 Vol. 10 No. 3, July-September 2008