Infarction in Fibroadenoma Breast During Pregnancy ... - JK Science
Infarction in Fibroadenoma Breast During Pregnancy ... - JK Science
Infarction in Fibroadenoma Breast During Pregnancy ... - JK Science

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
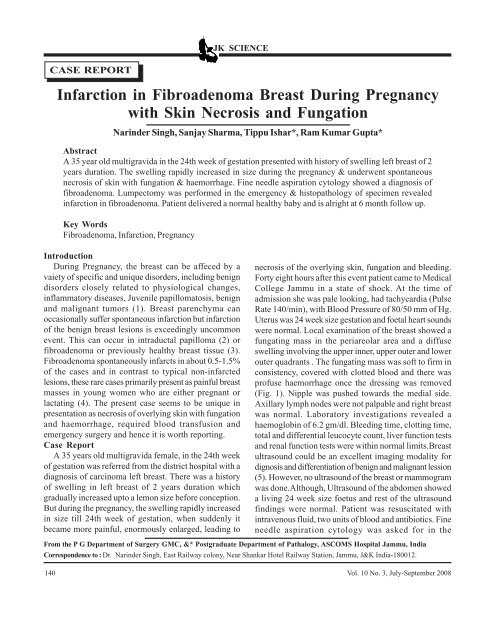
<strong>JK</strong> SCIENCECASE REPORT<strong>Infarction</strong> <strong>in</strong> <strong>Fibroadenoma</strong> <strong>Breast</strong> Dur<strong>in</strong>g <strong>Pregnancy</strong>with Sk<strong>in</strong> Necrosis and FungationNar<strong>in</strong>der S<strong>in</strong>gh, Sanjay Sharma, Tippu Ishar*, Ram Kumar Gupta*AbstractA 35 year old multigravida <strong>in</strong> the 24th week of gestation presented with history of swell<strong>in</strong>g left breast of 2years duration. The swell<strong>in</strong>g rapidly <strong>in</strong>creased <strong>in</strong> size dur<strong>in</strong>g the pregnancy & underwent spontaneousnecrosis of sk<strong>in</strong> with fungation & haemorrhage. F<strong>in</strong>e needle aspiration cytology showed a diagnosis offibroadenoma. Lumpectomy was performed <strong>in</strong> the emergency & histopathology of specimen revealed<strong>in</strong>farction <strong>in</strong> fibroadenoma. Patient delivered a normal healthy baby and is alright at 6 month follow up.Key Words<strong>Fibroadenoma</strong>, <strong>Infarction</strong>, <strong>Pregnancy</strong>IntroductionDur<strong>in</strong>g <strong>Pregnancy</strong>, the breast can be affeced by avaiety of specific and unique disorders, <strong>in</strong>clud<strong>in</strong>g benigndisorders closely related to physiological changes,<strong>in</strong>flammatory diseases, Juvenile papillomatosis, benignand malignant tumors (1). <strong>Breast</strong> parenchyma canoccasionally suffer spontaneous <strong>in</strong>farction but <strong>in</strong>farctionof the benign breast lesions is exceed<strong>in</strong>gly uncommonevent. This can occur <strong>in</strong> <strong>in</strong>traductal papilloma (2) orfibroadenoma or previously healthy breast tissue (3).<strong>Fibroadenoma</strong> spontaneously <strong>in</strong>farcts <strong>in</strong> about 0.5-1.5%of the cases and <strong>in</strong> contrast to typical non-<strong>in</strong>farctedlesions, these rare cases primarily present as pa<strong>in</strong>ful breastmasses <strong>in</strong> young women who are either pregnant orlactat<strong>in</strong>g (4). The present case seems to be unique <strong>in</strong>presentation as necrosis of overly<strong>in</strong>g sk<strong>in</strong> with fungationand haemorrhage, required blood transfusion andemergency surgery and hence it is worth report<strong>in</strong>g.Case ReportA 35 years old multigravida female, <strong>in</strong> the 24th weekof gestation was referred from the district hospital with adiagnosis of carc<strong>in</strong>oma left breast. There was a historyof swell<strong>in</strong>g <strong>in</strong> left breast of 2 years duration whichgradually <strong>in</strong>creased upto a lemon size before conception.But dur<strong>in</strong>g the pregnancy, the swell<strong>in</strong>g rapidly <strong>in</strong>creased<strong>in</strong> size till 24th week of gestation, when suddenly itbecame more pa<strong>in</strong>ful, enormously enlarged, lead<strong>in</strong>g tonecrosis of the overly<strong>in</strong>g sk<strong>in</strong>, fungation and bleed<strong>in</strong>g.Forty eight hours after this event patient came to MedicalCollege Jammu <strong>in</strong> a state of shock. At the time ofadmission she was pale look<strong>in</strong>g, had tachycardia (PulseRate 140/m<strong>in</strong>), with Blood Pressure of 80/50 mm of Hg.Uterus was 24 week size gestation and foetal heart soundswere normal. Local exam<strong>in</strong>ation of the breast showed afungat<strong>in</strong>g mass <strong>in</strong> the periareolar area and a diffuseswell<strong>in</strong>g <strong>in</strong>volv<strong>in</strong>g the upper <strong>in</strong>ner, upper outer and lowerouter quadrants . The fungat<strong>in</strong>g mass was soft to firm <strong>in</strong>consistency, covered with clotted blood and there wasprofuse haemorrhage once the dress<strong>in</strong>g was removed(Fig. 1). Nipple was pushed towards the medial side.Axillary lymph nodes were not palpable and right breastwas normal. Laboratory <strong>in</strong>vestigations revealed ahaemoglob<strong>in</strong> of 6.2 gm/dl. Bleed<strong>in</strong>g time, clott<strong>in</strong>g time,total and differential leucocyte count, liver function testsand renal function tests were with<strong>in</strong> normal limits.<strong>Breast</strong>ultrasound could be an excellent imag<strong>in</strong>g modality fordignosis and differentiation of benign and malignant lession(5). However, no ultrasound of the breast or mammogramwas done.Although, Ultrasound of the abdomen showeda liv<strong>in</strong>g 24 week size foetus and rest of the ultrasoundf<strong>in</strong>d<strong>in</strong>gs were normal. Patient was resuscitated with<strong>in</strong>travenous fluid, two units of blood and antibiotics. F<strong>in</strong>eneedle aspiration cytology was asked for <strong>in</strong> theFrom the P G Department of Surgery GMC, &* Postgraduate Department of Pathalogy, ASCOMS Hospital Jammu, IndiaCorrespondence to : Dr. Nar<strong>in</strong>der S<strong>in</strong>gh, East Railway colony, Near Shankar Hotel Railway Station, Jammu, J&K India-180012.140 Vol. 10 No. 3, July-September 2008
<strong>JK</strong> SCIENCEemergency which showed a diagnosis of fibroadenoma.After proper resuscitation, patient was taken up forsurgery and emergency lumpectomy was performedunder general anaesthesia with addition of tocolytic drugs(<strong>in</strong>j. Isoxsupr<strong>in</strong>e, <strong>in</strong>j. Proluton depot). Post operative shecont<strong>in</strong>ued on tocolytic drug, antibiotics and analgesics.Suction dra<strong>in</strong> was removed after 48 hrs. of the surgeryand stitches were taken out on 10th postoperative day.Gross specimen of the swell<strong>in</strong>g showed a grey white,lobulated, soft, fleshy mass about 20×15×12 cm size withfungation and central areas of haemorrhage. Microscopicexam<strong>in</strong>ation of the mass revealed large areas of <strong>in</strong>farction<strong>in</strong> fibroadenoma and histological pattern mostly seen aspericannalicular with loose oedmatous stroma (Fig. 2).Patient delivered a healthy full term male baby and isalright at 6 month follow up.Fig 1: Preoperative Photograph Show<strong>in</strong>g Fungat<strong>in</strong>g Mass withArea of <strong>Infarction</strong> and HaemorrhageFig 2: a) Low power Show<strong>in</strong>g Areas of Haemorrhagic <strong>Infarction</strong><strong>in</strong> <strong>Fibroadenoma</strong>. b) High power Exhibit<strong>in</strong>g PericannlicularPattern with Loose StromaDiscussionSpontaneous <strong>in</strong>farction <strong>in</strong> a fibroadenoma constitutesthe most characteristic example of necrosis of the breasttissue (6). Delaure and Redon (7) <strong>in</strong> 1949 were the firstto describe spontaneous <strong>in</strong>farction <strong>in</strong> fibroadenoma.Although successive reports have been published s<strong>in</strong>cethen, this type of pathology has not been dealt extremely<strong>in</strong> the literature (8). One of the most important feature ofspontaneous <strong>in</strong>farction <strong>in</strong> fibroadenoma is its associationwith pregnancy and lactation (9,10) although it has alsobeen described <strong>in</strong> adolescent girl (11) and follow<strong>in</strong>g f<strong>in</strong>eneedle aspiration(12). The pathophysiology of <strong>in</strong>farctionhas been attributed to the relative vascular ischemia dur<strong>in</strong>gphase of <strong>in</strong>creased metabolic demand (4) or thrombosisof the supply<strong>in</strong>g vessels dur<strong>in</strong>g pregnancy (13). <strong>Infarction</strong><strong>in</strong> fibroadenoma must be differentiated from a carc<strong>in</strong>oma(8) and our patient was also referred with a diagnosis ofmalignancy. <strong>Infarction</strong> may be focal or there may be totalnecrosis of a pre-exist<strong>in</strong>g benign lesion (10). Total orsubtotal <strong>in</strong>farctions are likely to <strong>in</strong>volve the overly<strong>in</strong>g sk<strong>in</strong>as well (9), as was seen <strong>in</strong> the present case. Afterreview<strong>in</strong>g the pert<strong>in</strong>ent literature most of the reportedcases have presented with tender lumps which wereexcised electively. But our case is unique <strong>in</strong> thepresentation with fungation and haemorrhage for whichblood transfusion and emergency surgery was required.ConclusionAn awareness about this unusual lesion is requiredwhile deal<strong>in</strong>g with the breast masses dur<strong>in</strong>g pregnancyand further the importance of dist<strong>in</strong>guish<strong>in</strong>g such apathology from carc<strong>in</strong>oma is highly stressed upon.References1. Sabate JM, Clatet M, Torrubia A et al. Radiologicalevaluation of breast disorder related to pregnancy andlactation.Radiographics 2007; 27 (Suppl): 101-24.2. Fl<strong>in</strong>t A, Oberman HA. <strong>Infarction</strong> and squamous metaplasiaof <strong>in</strong>traductal papilloma. A benign breast lesion that maysimulate carc<strong>in</strong>oma. Hum Pathol 1984, 15 : 765.3. Azzopardi JG.<strong>Fibroadenoma</strong>-Major Probl. Pathol 1979,11: 43.4. Raju GC, Narayns<strong>in</strong>gh V. <strong>Infarction</strong> of fibroadenoma ofthe breast. J Royal Coll Surg 1985, 30: 162-63.5. Son EJ , Oh KK , Kim EK. <strong>Pregnancy</strong> associated breastdisease; radiological feature and dignostic dilemmas. YonesiMed J 2006 ; 47(1): 32-42.6. Haagensen CD. Diseases of the breast, 4 th ed Philadelphia,WB Saunders Co. 1985.pp.275.7. Delarue J, Redon H. Les Infarctus Des <strong>Fibroadenoma</strong>sMammaires. Sem<strong>in</strong> Hop Paris 1949; 25: 2991.8. Matias-Guiu X, Calabuig R, Badia F, et al. Spontaneous<strong>in</strong>farcts <strong>in</strong> fibroadenomas of the breast. Current Surgery1988; 277-79.9. Majumdar B, Rosales-Qu<strong>in</strong>tana S. <strong>Infarction</strong> of breastfibroadenomas dur<strong>in</strong>g pregnancy. JAMA 1975; 231: 963.10. Wilk<strong>in</strong>son L, Green WO. <strong>Infarction</strong> of breast lesion dur<strong>in</strong>gpregnancy and lactation. Cancer 1964; 17: 1567.11. Fowler CL. Spontaneous <strong>in</strong>farction of fibroadenoma <strong>in</strong> anadolescent girl, Pediatr. Radiol 2004; 34: 988-90.12. Vargas MP, Mer<strong>in</strong>o MJ. Infarcted myoxoid fibroadenomafollow<strong>in</strong>g f<strong>in</strong>e needle aspiration. Arch Pathol Lab Med1996 ;120:1069-71.13. Lucey J.J. Spontaneous <strong>in</strong>faction of the breast. J Cl<strong>in</strong> Path1975; 28 : 937-43.Vol. 10 No. 3, July-September 2008 141