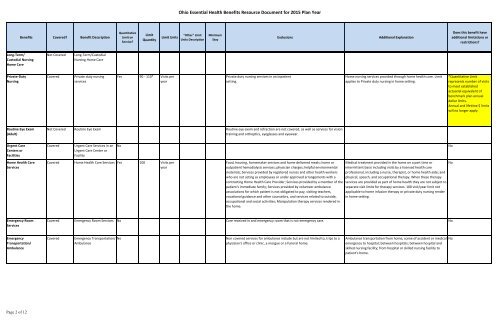
<strong>Ohio</strong> <strong>Essential</strong> <strong>Health</strong> <strong>Benefits</strong> Resource Document for 2015 <strong>Plan</strong> Year<strong>Benefits</strong> Covered? Benefit DescriptionQuantitativeLimit onService?LimitQuantityLimit Units"Other" LimitUnits DescriptionMinimumStayExclusionsAdditional ExplanationDoes this benefit haveadditional limitations orrestrictions?Long-Term/Custodial NursingHome CareNot CoveredLong-Term/CustodialNursing Home CarePrivate-DutyNursingCoveredPrivate duty nursingservicesYes 90 - 110* Visits peryearPrivate duty nursing services in an inpatientsetting.Home nursing services provided through home health care. Limitapplies to Private duty nursing in home setting.*Quantitative Limitrepresents number <strong>of</strong> visitsto meet establishedactuarial equivalent <strong>of</strong>benchmark plan annualdollar limits.Annual and lifetime $ limitswill no longer apply.Routine Eye Exam(Adult)Not Covered Routine Eye Exam Routine eye exam and refraction are not covered, as well as services for visiontraining and orthoptics, eyeglasses and eyewear.Urgent CareCenters orFacilitiesHome <strong>Health</strong> CareServicesCoveredUrgent Care Services in anUrgent Care Center orFacilityCovered Home <strong>Health</strong> Care Services Yes 100 Visits peryearNoFood, housing, homemaker services and home delivered meals; home oroutpatient hemodialysis services; physician charges; helpful environmentalmaterials; Services provided by registered nurses and other health workerswho are not acting as employees or under approved arrangements with acontracting Home <strong>Health</strong> Care Provider; Services provided by a member <strong>of</strong> thepatient's immediate family; Services provided by volunteer ambulanceassociations for which patient is not obligated to pay, visiting teachers,vocational guidance and other counselors, and services related to outside,occupational and social activities; Manipulation therapy services rendered inthe home.Medical treatment provided in the home on a part time orintermittent basis including visits by a licensed health carepr<strong>of</strong>essional, including a nurse, therapist, or home health aide; andphysical, speech, and occupational therapy. When these therapyservices are provided as part <strong>of</strong> home health they are not subject toseparate visit limits for therapy services. 100 visit/year limit notapplicable to home infusion therapy or private duty nursing renderin home setting.NoNoEmergency RoomServicesCovered Emergency Room Services No Care received in and emergency room that is not emergency care. NoEmergencyTransportation/AmbulanceCoveredEmergency Transportation/AmbulanceNoNon covered services for ambulance include but are not limited to, trips to aphysician's <strong>of</strong>fice or clinic, a morgue or a funeral home.Ambulance transportation from home, scene <strong>of</strong> accident or medicalemergency to hospital; between hospitals; between hospital andskilled nursing facility; from hospital or skilled nursing facility topatient's home.No<strong>Page</strong> 2 <strong>of</strong> 12
<strong>Ohio</strong> <strong>Essential</strong> <strong>Health</strong> <strong>Benefits</strong> Resource Document for 2015 <strong>Plan</strong> Year<strong>Benefits</strong> Covered? Benefit DescriptionQuantitativeLimit onService?LimitQuantityLimit Units"Other" LimitUnits DescriptionMinimumStayExclusionsAdditional ExplanationDoes this benefit haveadditional limitations orrestrictions?Inpatient HospitalServices (e.g., HospitalStay)Covered Inpatient Hospital Services No Oral surgery that is dental in origin; Removal <strong>of</strong> impacted wisdom teeth;Reversal <strong>of</strong> voluntary sterilization; radial keratotomy, keratoplasty, Lasik andother surgical procedures to correct refractive defects; surgeries for sexualdysfunction; surgeries or services for sexual transformation; surgical treatment<strong>of</strong> flat feet, subluxation <strong>of</strong> the foot, weak, strained, unstable feet, tarsalgia,metatarsalgia, hyperkeratoses; surgical treatment <strong>of</strong> gynecomastia; treatment<strong>of</strong> hyperhidrosis; sclerotherapy for treatment <strong>of</strong> varicose veins <strong>of</strong> the lowerextremity; treatment <strong>of</strong> telangiectatic dermal veins.Facility billed services while in an inpatient facility. Includes roomand board, nursing services, and ancillary services and supplies.Yes - also see specificexceptions to theseexclusons and/or additionalexclusions that are detailedunder separately listedbenefits or services (e.g.,bariatric surgery, cosmeticsurgery)Inpatient Physicianand SurgicalServicesCoveredInpatient Physician andSurgical ServicesYes 1 Other One (1)Inpatientvisit/day perPhysician orotherPr<strong>of</strong>essionalProviderOral surgery that is dental in origin; Removal <strong>of</strong> impacted wisdom teeth;Reversal <strong>of</strong> voluntary sterilization; radial keratotomy, keratoplasty, Lasik andother surgical procedures to correct refractive defects; surgeries for sexualdysfunction; surgeries or services for sexual transformation; surgical treatment<strong>of</strong> flat feet, subluxation <strong>of</strong> the foot, weak, strained, unstable feet, tarsalgia,metatarsalgia, hyperkeratoses; surgical treatment <strong>of</strong> gynecomastia; treatment<strong>of</strong> hyperhidrosis; sclerotherapy for treatment <strong>of</strong> varicose veins <strong>of</strong> the lowerextremity; treatment <strong>of</strong> telangiectatic dermal veins.Facility billed services while in an inpatient facility. Includes roomand board, nursing services, and ancillary services and supplies.Yes - also see specificexceptions to theseexclusons and/or additionalexclusions that are detailedunder separately listedbenefits or services (e.g.,bariatric surgery, cosmeticsurgery)Bariatric Surgery Not Covered Bariatric Surgery Bariatric surgery, regardless <strong>of</strong> the purpose it is proposed or performed. Thisincludes Roux- en-Y(RNY), Laparoscopic gastric bypass surgery or other gastricbypass surgery (surgical procedures that reduce stomach capacity and divertpartially digested food from the duodenum to the jejunum, the section <strong>of</strong> thesmall intestine extending from the duodenum), or Gastroplasty, (surgicalprocedures that decrease the size <strong>of</strong> the stomach), or gastric bandingprocedures. Complications directly related to bariatric surgery that results inan Inpatient stay or an extended Inpatient stay for the bariatric surgery, asdetermined by Us, are not covered. This exclusion applies when the bariatricsurgery was not a Covered Service under this <strong>Plan</strong> or any previous Anthemplan, and it applies if the surgery was performed while the Member wascovered by a previous carrier/self-funded plan prior to coverage under thisCertificate. Directly related means that the Inpatient stay or extended Inpatientstay occurred as a direct result <strong>of</strong> the bariatric procedure and would not havetaken place in the absence <strong>of</strong> the bariatric procedure.<strong>Page</strong> 3 <strong>of</strong> 12