322-0543 EMERGENCY DEPARTMENT RECORD FORM rev 05-07
322-0543 EMERGENCY DEPARTMENT RECORD FORM rev 05-07
322-0543 EMERGENCY DEPARTMENT RECORD FORM rev 05-07

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
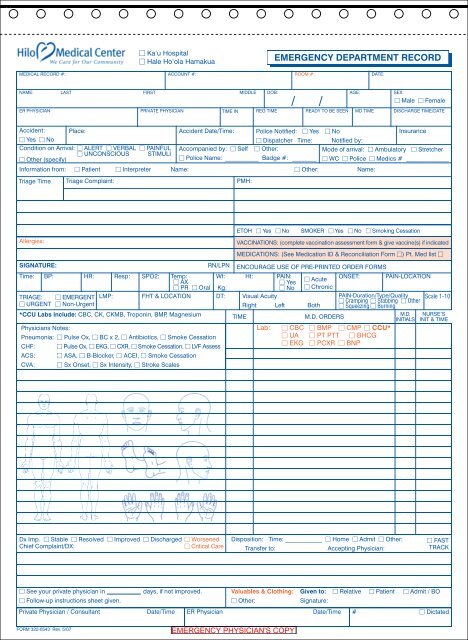
Ka‘u Hospital Hale Ho‘ola Hamakua<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> <strong>RECORD</strong>MEDICAL <strong>RECORD</strong> #:ACCOUNT #:ROOM #:DATE:NAME:ER PHYSICIANLASTFIRSTMIDDLE DOB:AGE:SEX: Male FemalePRIVATE PHYSICIAN TIME IN REG TIME READY TO BE SEEN MD TIME DISCHARGE TIME/DATEAccident: Place: Accident Date/Time: Police Notified: Yes NoInsurance Yes No Dispatcher Time: Notified by:Condition on Arrival: ALERT VERBAL PAINFUL Accompanied by: Self Other:Mode of arrival: Ambulatory Stretcher UNCONSCIOUS STIMULI Other (specify) Police Name: ___________ Badge #: ________ WC Police Medics # ______________Information from: Patient Interpreter Name: Other: Name:Triage Time Triage Complaint:PMH:Allergies:SIGNATURE:RN/LPNETOH Yes NoSMOKER Yes No Smoking CessationVACCINATIONS: (complete vaccination assessment form & give vaccine(s) if indicatedMEDICATIONS: (See Medication ID & Reconciliation Form ) Pt. Med list ENCOURAGE USE OF PRE-PRINTED ORDER <strong>FORM</strong>STime: BP: HR: Resp: SPO2: Temp: Wt: Ht: PAIN: AX Yes AcuteONSET: PAIN-LOCATION PR Oral Kg: No ChronicTRIAGE: EMERGENT LMP: FHT & LOCATION DT: Visual AcuityPAIN-Duration/Type/Quality Scale 1-10 Cramping Stabbing Other URGENT Non-UrgentRight Left Both Squeezing Burning*CCU Labs include: CBC, CK, CKMB, Troponin, BMP, MagnesiumTIMEM.D. ORDERSM.D.INITIALSNURSE’SINIT & TIMEPhysicians Notes:Lab: CBC BMP CMP CCU*Pneumonia: Pulse Ox, BC x 2, Antibiotics, Smoke Cessation UA PT PTT BHCG EKG PCXR BNPCHF: Pulse Ox, EKG, CXR, Smoke Cessation, LVF AssessACS: ASA, B-Blocker, ACEI, Smoke CessationCVA: Sx Onset, Sx Intensity, Stroke ScalesDx Imp. Stable Resolved Improved Discharged WorsenedChief Complaint/DX: Critical CareDisposition: Time: ____________ Home Admit Other:Transfer to:Accepting Physician: FASTTRACK See your private physician indays, if not improved. Valuables & Clothing: Given to: Relative Patient Admit / BO Follow-up instructions sheet given. Other:Signature:Private Physician / Consultant Date/Time ER Physician Date/Time # Dictated<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>