322-0543 EMERGENCY DEPARTMENT RECORD FORM rev 05-07
322-0543 EMERGENCY DEPARTMENT RECORD FORM rev 05-07
322-0543 EMERGENCY DEPARTMENT RECORD FORM rev 05-07

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Ka‘u Hospital Hale Ho‘ola Hamakua<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> <strong>RECORD</strong>MEDICAL <strong>RECORD</strong> #:ACCOUNT #:ROOM #:DATE:NAME:ER PHYSICIANLASTFIRSTMIDDLE DOB:AGE:SEX: Male FemalePRIVATE PHYSICIAN TIME IN REG TIME READY TO BE SEEN MD TIME DISCHARGE TIME/DATEAccident: Place: Accident Date/Time: Police Notified: Yes NoInsurance Yes No Dispatcher Time: Notified by:Condition on Arrival: ALERT VERBAL PAINFUL Accompanied by: Self Other:Mode of arrival: Ambulatory Stretcher UNCONSCIOUS STIMULI Other (specify) Police Name: ___________ Badge #: ________ WC Police Medics # ______________Information from: Patient Interpreter Name: Other: Name:Triage Time Triage Complaint:PMH:Allergies:SIGNATURE:RN/LPNETOH Yes NoSMOKER Yes No Smoking CessationVACCINATIONS: (complete vaccination assessment form & give vaccine(s) if indicatedMEDICATIONS: (See Medication ID & Reconciliation Form ) Pt. Med list ENCOURAGE USE OF PRE-PRINTED ORDER <strong>FORM</strong>STime: BP: HR: Resp: SPO2: Temp: Wt: Ht: PAIN: AX Yes AcuteONSET: PAIN-LOCATION PR Oral Kg: No ChronicTRIAGE: EMERGENT LMP: FHT & LOCATION DT: Visual AcuityPAIN-Duration/Type/Quality Scale 1-10 Cramping Stabbing Other URGENT Non-UrgentRight Left Both Squeezing Burning*CCU Labs include: CBC, CK, CKMB, Troponin, BMP, MagnesiumTIMEM.D. ORDERSM.D.INITIALSNURSE’SINIT & TIMEPhysicians Notes:Lab: CBC BMP CMP CCU*Pneumonia: Pulse Ox, BC x 2, Antibiotics, Smoke Cessation UA PT PTT BHCG EKG PCXR BNPCHF: Pulse Ox, EKG, CXR, Smoke Cessation, LVF AssessACS: ASA, B-Blocker, ACEI, Smoke CessationCVA: Sx Onset, Sx Intensity, Stroke ScalesDx Imp. Stable Resolved Improved Discharged WorsenedChief Complaint/DX: Critical CareDisposition: Time: ____________ Home Admit Other:Transfer to:Accepting Physician: FASTTRACK See your private physician indays, if not improved. Valuables & Clothing: Given to: Relative Patient Admit / BO Follow-up instructions sheet given. Other:Signature:Private Physician / Consultant Date/Time ER Physician Date/Time # Dictated<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>
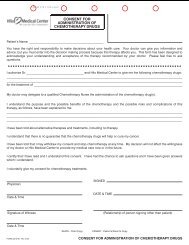
Ka‘u Hospital Hale Ho‘ola Hamakua<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> <strong>RECORD</strong>MEDICAL <strong>RECORD</strong> #:ACCOUNT #:ROOM #:DATE:NAME:LASTFIRSTMIDDLEDOB:AGE:SEX: Male FemaleER PHYSICIANPRIVATE PHYSICIAN TIME IN REG TIME READY TO BE SEEN MD TIMEDISCHARGE TIME/DATEAccident: Place: Accident Date/Time: Police Notified: Yes NoInsurance Yes No Dispatcher Time: Notified by:Condition on Arrival: ALERT VERBAL PAINFUL Accompanied by: Self Other:Mode of arrival: Ambulatory Stretcher UNCONSCIOUS STIMULI Other (specify) Police Name: ___________ Badge #: ________ WC Police Medics # ______________Information from: Patient Interpreter Name: Other: Name:Triage Time Triage Complaint:PMH:Allergies:SIGNATURE:RN/LPNETOH Yes NoSMOKER Yes No Smoking CessationVACCINATIONS: (complete vaccination assessment form & give vaccine(s) if indicatedMEDICATIONS: (See Medication ID & Reconciliation Form ) Pt. Med list ENCOURAGE USE OF PRE-PRINTED ORDER <strong>FORM</strong>STime: BP: HR: Resp: SPO2: Temp: Wt: Ht: PAIN: AX Yes AcuteONSET: PAIN-LOCATION PR Oral Kg: No ChronicTRIAGE: EMERGENT LMP: FHT & LOCATION DT: Visual AcuityPAIN-Duration/Type/Quality Scale 1-10 Cramping Stabbing Other URGENT Non-UrgentRight Left Both Squeezing BurningMental Status: ____ WNL____ Awake, A & O x 3____ Awake, Oriented _________ Response toVerbal Stimuli____ Response toPainful Stimuli____ Unresponsive____ Age AppropriateBehavior: ____ WNL____ Unconscious____ Calm, Cooperative____ Withdrawn____ Depressed____ Anxious____ Irritable____ Hostile / Aggressive____ Other __________Skin: ____ WNL____ Dry / Warm____ Hot ____ Moist____ Cool____ Mottled____ Pale____ JaundicedMucus Membrane____ Dry / moistCardiac: ____ WNLChest Pain Now Y or N____ Radiating____ Non-radiatingHeart Rate____ Regular ____ IrregularEdema Y or N______________________Pain: ____ WNL____ Dull / Sharp____ Pressure / Aches____ Constant / Intermittent____ Radiates to ____________________________0No Hurt2HurtsLittle Bit4HurtsLittleMoreRespiratory: WNL____ Dyspnea____ Retraction____ Rapid Breath Sounds ____ R ____ L____ Slow____ Shallow____ Deep____ Stridor____ Cough____ LaboredClearCracklesWheezesDiminishedAbsent____ R ____ L____ R ____ L____ R ____ L____ R ____ L____ R ____ LNeuro: ____ WNLPupils ____ PERLSize: __ R __ LReaction: __ R __ LGCS: ____________Deficits: ______________ = Strength____ MAE See Neuro formSpeech: ____ WNL____ Normal____ Slurred____ Aphasic1 2 3 4 5 6 7 8Abdomen: ____ WNL____ Soft ____ Rigid ____ Distended____ GuardingBowel Tones: ____ Present____ Diminished ____ AbsentTenderness: ____ None____ Epigastric ___ Rebound____ RUQ ___ RLQ ___ LUQ ___ LLQOther __________________________Last BM: ________________________6HurtsEvenMore8HurtsWhole Lot10HurtsWorstExtremities: ____ WNL____ MAE ____ = Strength____ Deformity _____________ CMS____ Pulse____ Edema____ Laceration _____________ Abrasions _________GU: ____ WNL____ Voiding Difficulty____ Flank Pain R / L____ Dysuria____ Hematuria____ Frequency____ Urgency____ Unable to voidEENT: ____ WNLEars:Pain ___ R ___ LDrainage ___ R ___ LTinnitus ___ R ___ L____ Acute Deficits ____________________________Eyes: VA See AboveOB / GYN: ____ WNLGR ___ PARA ___ AB ___Vaginal Bleeding: Y or NVaginal Discharge: Y or NContraception: __________FHT: See AboveLMP: see AboveNutrition:____ N/AL____ WDWN____ Obese____ Cache tic____ Denies Issues____ Wt Loss / Gain10 lbs in one monthChronic Deficits: ____ WNL____ Legally Blind____ Hearing Aid____ Amputation/Paralysis____ AV Shunt R / L____ Mastectomy R / L____ Walker ___ Cane ___ BraceHave you developed changes in ADL's, mobilityor communication recently? Yes No<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>Living Situation:____ N/A____ With Family____ With Friends____ Alone____ Nursing Home____ HomelessSignatures:Barriers to Learning: ____ WNLReady to Learn: Y or N____ Unstable____ Emotional____ Cognitive____ Sight/Hearing/Speech____ Language ____________D.V. Screening:____ N/AAfraid Y or NControl Y or NHurt Y or NDeferred ___________GCS-Glascow Coma Scale WDWN-Well developed/Well nourished VA-Visual Acuity MAE-Moves all extremities SPO2-Pulse Oximetry PCXR-Portable Chest XrayDIAGRAMMING CODE:ABRASIONS - ABRUISES - BRBURNS - BUERYTHEMA - ELACERATIONS - LPETECHIAE - PPRESSURE ULCER - PURASH - RSCARS - SSTOMAS - STULCERS - UOTHER - OOTHER: (I.E. TATTOOS, AMPUTATIONS, FRAIL SKIN,DISCOLORATION) SEE BODY OR BURN <strong>RECORD</strong>
PATIENT NAME:<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> CRITICAL CARE NURSING NOTES CONTINUATION SHEETMED. REC. NO. ACCOUNT NO. PATIENT NAME DATEDATE:PAGE 5ATTENDING DOCTORBIRTHDATEAGEALLERGIES:DATE TIME BP P R T SPO2RN RN RN RN<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>
<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> <strong>RECORD</strong>MEDICAL <strong>RECORD</strong> #:ACCOUNT #:ROOM #:DATE:NAME:LASTFIRSTMIDDLEDOB:AGE:SEX: Male FemalePLACE STICKERS UPRIGHT IN SPACES BELOWLEVEL OFSERVICE EQ Pump IV Kendall 270-0868 Removal of Cast 450-4049 Breakfast Dinner Code 500-450-0030 Bair Hugger 450-5003 Lunch<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>
HILO MEDICAL CENTER<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> ENCOUNTER <strong>FORM</strong>Category Based Emergency Department Procedure Charging GuideAcct # _______________________ MR # ________________________________Patient Name:________________________________________________________Date of Service: ______________________________________________________Office Use:Nurse: ____________________________________________________ER Clerk:__________________________________________________ 11/3/06NURSE TO CHARGE:LEVEL OF CARE 450: INFUSIONS / INJECTIONS 450: VACCINE ADMINISTRATION 450:Minimal/Fast Track0001 99281 Infusion Therapy: 0-1 Hr<strong>07</strong>65 9<strong>07</strong>65 Administration Vaccine /2104 90471Minor Care0002 99282 Infusion Ea. add’l hr. (Max 8 Hr) <strong>07</strong>66 9<strong>07</strong>66 Immunization OtherModerate Care0003 99283 Hydration: 0-1 Hr<strong>07</strong>60 9<strong>07</strong>60 Administration Ea. Add’l Vaccine 2103 90472Intermediate Care0004 99284 Hydration Ea. add’l hr.<strong>07</strong>61 9<strong>07</strong>61 Administration Hepatitis B Vaccine 0<strong>05</strong>8 90471Guarded00<strong>05</strong> 99285 Injection: Intra Arterial<strong>07</strong>73 9<strong>07</strong>73 Administration Influenza Vaccine 2100 G0008Critical Care0006 99291 Injection: Intramuscular / Subcu <strong>07</strong>72 9<strong>07</strong>72 Administration PPV Vaccine 2101 G0009Gastric Lavage/ NG Tube1500 911<strong>05</strong> Injection: IV Push Initial Drug <strong>07</strong>74 9<strong>07</strong>74 IV RELATED PROCEDURES 450:Cardioversion-Elec11<strong>05</strong> 92960 Injection: IV Push Each Add’l Seq Drug <strong>07</strong>75 9<strong>07</strong>75 Coronary Thrombolysis via IV 0040 92977Cardiopulmonary Resuscitation 0030 92950 IV Inf Add’l Seq 0-1 Hr<strong>07</strong>67 9<strong>07</strong>67 Venipuncture6415 36415Temp Transcutaneous Pacing 2953 92953 IV Infusion Concurrent<strong>07</strong>68 9<strong>07</strong>68RESPIRATORY TREATMENTIV Inf Port/Impl Pump >8 Hrs <strong>07</strong>70 C8957 OTHER _______________________________________Demo/Eval Inhal Treatment 4664 94664 POINT OF CARE TESTING 450:MISCELLANEOUSRespiratory Treatment Initial 5866 94640 Fingerstick2948 82948 Rhythm ECG w/EKG 12 Lead 3042 94664Respiratory Treatment Subsq 5868 94640 Hemoccult2270 82270Gastroccult2273 82271OTHER _______________________________________MEDICAL <strong>RECORD</strong> TO CODE:LEVEL OF CARE 450:Endo Trach Intubation1500 31500Procedural SedationTemp Transvenous Pacemaker 3210 33210Pericardiocentesis3010 33010Thoracentesis2000 32000Tube Thoracostomy2020 32020Peritoneal Asp / Lavage9080 49080Lumbar Puncture2319 62270Tracheostomy1603 31603Change of Gastrotomy Tube 3760 43760IV RELATED PROCEDURES 450:Insert PICC Line > 5 yrs 6489 36569OTHER _______________________________________INJECTION: 450:Asp / Inj Bursa Sm Joint0600 20600Asp / Inj Bursa Med Joint06<strong>05</strong> 206<strong>05</strong>Asp / Inj Bursa Lg Joint0610 20610Injection: Ligament<strong>05</strong>50 2<strong>05</strong>50Dental Block4404 64400Nerve Block4450 64450GENITAL, URINARY, RECTUMHemorrhoid / Thrombectomy 6320 46320I & D Bartholins6420 56420I & D Perianal Abscess6<strong>05</strong>0 46<strong>05</strong>0OTHER _______________________________________WOUND EXPLORATION 450:Explore Wound NeckExplore Wound ChestExplore Wound Abdm / FlankExplore Wound Extremity010001010102010320100201012010320103BURN CARE: 450:Dress/Debride - Sm w/o Anesth 6020 16020Dress/Debride - Med w/o Anesth 6025 16025Dress/Debride - Lg w/o Anesth 6030 16030OTHER _______________________________________BLOOD TRANSFUSIONS: 450:Blood Transfusion0110 36430REDUCTION OF DISLOCATIONSTMJ Dislocation1480 21480Shoulder Dislocation3650 23650Elbow Dislocation4600 24600Radial Head Subluxation4640 24640MCP Finger6700 26700Interphalangeal Joint Finger 6770 26770Patellar Dislocation7560 27560Ankle Dislocation7840 27840MCP Toe8630 28630Interphalangeal Joint Toe8660 28660INTEGUMENTARY 450:I & D Abscess0060 10060I & D Abscess - Complex0061 10061I & D Pilonidal Cyst0080 10080Incision & Removal FB, Subcu 0122 10120tissue, simpleIncision & Removal FB, Subcu 0121 10121tissue, complicatedDebridement Infected Skin 1000 11000Debridement; Skin Partial Thick 1040 11040Debridement; Skin Full Thick 1041 11041Debridement; Skin/Subcu Tissue 1042 11042Debridement; Skin/Subcu Tissue & 1043 11043MuscleINTEGUMENTARY (Cont) 450:I & D Hematoma0141 10140Puncture Asp / Abscess / Cyst / 0161 10160HematomaAvul Nail Plate, Partial / Complete 1730 11730SimpleExcision Nail Matrix1750 11750Wedge Excise, Skin of Nail Fold 1765 11765OTHER _______________________________________MISCELLANEOUS: 450:Remove Earwax9210Nasal Hemorr/Ant Pack/Caut Simp 0901Nasal Hemorr/Ant Pack/Caut Compl 0903Nasal Hemorr/Post Pack/Caut 09<strong>05</strong>Laryngoscopy15<strong>05</strong>I & D, Abscess Ear8700FRACTURE CARE: CLOSED 450:Nasal Bond1310Mandibular1450Clavicular3500Proximal Humeral3600Distal Radial5600Metacarpal, Single6600Prox / Med Phalang, Finger 6720Finger / Thumb w/o Manip 6750Radial Shaft w/o Manip5500Ulnar Shaft w/o Manip5530Patella7520Distal Tibia7760Distal Fibula7786Calcaneal8400Tarsal Bone8450Metatarsal Bone8470Great Toe8490692103090130903309<strong>05</strong>315<strong>05</strong>690002131021450235002360025600266002672026850255002553027520277602778628400284502847028490<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>
FRACTURE CARE: CLOSED (Cont) 450:LACERATION REPAIR: 450:Face, Ears, Eyelids, LipsToe w/o Manip8510Toe w/Manip8515SPLINT / STRAPPING / CAST 450:Long Arm Splint91<strong>05</strong>Short Arm Splint9125Long Leg Splint95<strong>05</strong>Short Leg Splint9515Finger Splint - Static9130Long Arm Cast9065Short Arm Cast9<strong>07</strong>5Long Leg Cast9345Short Leg Cast94<strong>05</strong>Strapping Shoulder9240Strapping, Elbow or Wrist 9260Strapping, Hand or Finger 9280Strapping, Knee9530Strapping, Ankle9540Strapping, Toes9550Strapping, Ulna Boot9580Removal of Cast40492851028515291<strong>05</strong>29125295<strong>05</strong>29515291302906529<strong>07</strong>529345294<strong>05</strong>29240292602928029530295402955029580297<strong>05</strong>OTHER _______________________________________Scalp, Neck, Trunk, Hands, FeetSimple Lac
HILO MEDICAL CENTER<strong>EMERGENCY</strong> <strong>DEPARTMENT</strong> ENCOUNTER <strong>FORM</strong>Point Based Emergency Acuity Level Charging GuidePatient Name:________________________________________________________Date of Service: ______________________________________________________Admitted: _____________ Discharge: _____________ Transfer:______________Office Use:Nurse: ____________________________________________________ER Clerk:__________________________________________________Data Entry Clerk: __________________________________________ 11/22/06POINT VALUE 10 POINT VALUE 20 POINT VALUE 30 POINT VALUE 40 POINT VALUE 50ASSESSMENTX Triage assessmentPsych Eval (simple)Reassessment - ER staffRestraint Usage (child)Pediatric WeightCirculation Sensation &Motion (CMS) ChecksUA/Tox Screencollected by staffCulture Screen - throat -wnd - collected by staffX Med ScreeningExam/Nsg Asmt (of MSEonly, use #8900003)Neuro (CNS) ChecksAssessment - PsychNurse (BHR)Eye AcuityC - Collar/Miami J CollarApplicationCombative or DisruptivePatient/Restraint Usage(adult)Psych Eval (Complex)MD ConsultSuicide Precaution 1:1Pedi-Bag for UAPO Meds (simple)Meal Set UpTopical MedicationsSuppositoriesOrthostatic Vital SignsET MedsPO Meds (complex)Sublingual Meds - withcontinued assessmentsS/L flush / D/CMEDICATION / FLUID ADMINISTRATIONNoc Cabinet Meds -issuedCharcoal / Sorbitol AdminPortacath accessRapid Sequence IntubationArterial Line Placement(assist)1:1 Care - Trauma, Cardiac, suicideprecautions - Transfers (Queens)Thrombolytic Therapy -Cardiac 1:1 CarePacemaker Insertion (assist)Vascath - assistDeclotting (after hours)PO Meds (complex) -oral contrastCharcoal / Ipecac AdminMed List / ValuablesG-Tube FlushORTHOPEDIC CAREWalker InstructionsHip Fract. Care PathCold/Hot Pack ApplicationCrutch Use instructionsWOUND CARESteri Strip ApplicationRing RemovalWound Dressing(complex)Suture Set Up - SterileIrrigation with simpulse(complex)Wound Dressing(intermediate)Wound Prep (complex)Irrigation of WoundSuture RemovalWound Dressing (simple)Wound Prep(intermediate)Wound Prep (simple)<strong>FORM</strong> <strong>322</strong>-<strong><strong>05</strong>43</strong> Rev. 5/<strong>07</strong>
POINT VALUE 10 POINT VALUE 20 POINT VALUE 30 POINT VALUE 40 POINT VALUE 50CARDIOPULMONARY CAREO2 Mask / CannulaCardiac Monitor Continuous -BP, SPO2, RhythmChest Tube Insertion (assist)Continuous SPO2MonitoringOral / Bulb SyringeSuctioningBedpanCool Air Mist NebulizerNIBP Monitoring(continuous)ABG by ER staffET SuctioningGI / GU / GYN CAREBladder Cath (foley)Tracheotomy CareCHF - Care PathPneumonia - Care PathUltrasound - OB - withfoleyVentilator Management (byER Staff)CT / US / r/o AAA/nursestand by onlyCode 500, Intubation, CPR, IVmeds/continuous monitoringUrinalStraight CathColostomy IrrigationCommodeFetal Heart Sounds /DopplerPelvic Exam (assist)Foley IrrigationRectal Exam (assist)EnemaMISCELLANEOUSClerical registration /Old chartsDischarge Instructionswith HandoutsHygienic Skin CleaningIntradepartmentTransport - RadiologyEye/Ear IrrigationMandatory Reporting toHPDAdmit to M/S telemetry -includes transportAdmit to ICU / OR / Psychincludes transportCT Head with IV Contrast/nurse stand by onlyCT abdomen/appendix with oral andrectal contrast/nurse stand by onlyPROCEDURAL SEDATION: Includes1:1 and cardiac monitorFiberoptic Scope - assistSupport/Teaching i.e. EDteach inhaler useOral/Bulb SyringeSuctioningTOTAL ALL (Columns1,2,3,4,5) =Support/TeachingcomplexLegal ETOH - nursestandby w / HPDAdmit / transport to floorno telemetryOTHER:OTHER:MRI - with staffaccompanyingOTHER:Transport to Queens:__________________________EMS Base Station(designated Base)Post Mortem Care1. Total this Column 2. Total this Column 3. Total this Column 4. Total this Column 5. Total this ColumnOBSERVATION, INJECTION/INFUSION & OTHER MEDICAL SERVICES W/SPECIALcoding -please mark procedures done in ER -- circle as appropriateDOA3108900FOR BUSINESS OFFICE USE ONLY:Point System BelowUse Modifier 25 for any radiology test listed:Modifier Levels listed on Category Based FormLevel 1 (251)99291Splint, Sling & Swathe, Ace bandage,Crutches,Walker