Mineral Homeostasis in CKD - Mineral and Bone Disorder - Medscape
Mineral Homeostasis in CKD - Mineral and Bone Disorder - Medscape
Mineral Homeostasis in CKD - Mineral and Bone Disorder - Medscape

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
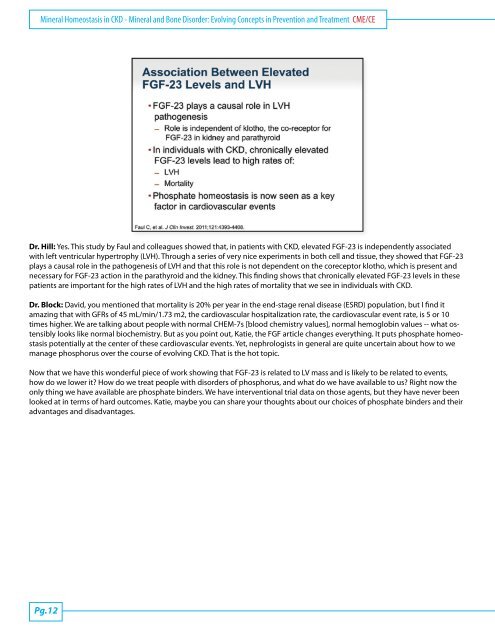
<strong>M<strong>in</strong>eral</strong> <strong>Homeostasis</strong> <strong>in</strong> <strong>CKD</strong> - <strong>M<strong>in</strong>eral</strong> <strong>and</strong> <strong>Bone</strong> <strong>Disorder</strong>: Evolv<strong>in</strong>g Concepts <strong>in</strong> Prevention <strong>and</strong> Treatment CME/CEDr. Hill: Yes. This study by Faul <strong>and</strong> colleagues showed that, <strong>in</strong> patients with <strong>CKD</strong>, elevated FGF-23 is <strong>in</strong>dependently associatedwith left ventricular hypertrophy (LVH). Through a series of very nice experiments <strong>in</strong> both cell <strong>and</strong> tissue, they showed that FGF-23plays a causal role <strong>in</strong> the pathogenesis of LVH <strong>and</strong> that this role is not dependent on the coreceptor klotho, which is present <strong>and</strong>necessary for FGF-23 action <strong>in</strong> the parathyroid <strong>and</strong> the kidney. This f<strong>in</strong>d<strong>in</strong>g shows that chronically elevated FGF-23 levels <strong>in</strong> thesepatients are important for the high rates of LVH <strong>and</strong> the high rates of mortality that we see <strong>in</strong> <strong>in</strong>dividuals with <strong>CKD</strong>.Dr. Block: David, you mentioned that mortality is 20% per year <strong>in</strong> the end-stage renal disease (ESRD) population, but I f<strong>in</strong>d itamaz<strong>in</strong>g that with GFRs of 45 mL/m<strong>in</strong>/1.73 m2, the cardiovascular hospitalization rate, the cardiovascular event rate, is 5 or 10times higher. We are talk<strong>in</strong>g about people with normal CHEM-7s [blood chemistry values], normal hemoglob<strong>in</strong> values -- what ostensiblylooks like normal biochemistry. But as you po<strong>in</strong>t out, Katie, the FGF article changes everyth<strong>in</strong>g. It puts phosphate homeostasispotentially at the center of these cardiovascular events. Yet, nephrologists <strong>in</strong> general are quite uncerta<strong>in</strong> about how to wemanage phosphorus over the course of evolv<strong>in</strong>g <strong>CKD</strong>. That is the hot topic.Now that we have this wonderful piece of work show<strong>in</strong>g that FGF-23 is related to LV mass <strong>and</strong> is likely to be related to events,how do we lower it? How do we treat people with disorders of phosphorus, <strong>and</strong> what do we have available to us? Right now theonly th<strong>in</strong>g we have available are phosphate b<strong>in</strong>ders. We have <strong>in</strong>terventional trial data on those agents, but they have never beenlooked at <strong>in</strong> terms of hard outcomes. Katie, maybe you can share your thoughts about our choices of phosphate b<strong>in</strong>ders <strong>and</strong> theiradvantages <strong>and</strong> disadvantages.Pg.12




![NIH STROKE SCALE Interval: 1[ ] Baseline 2[ ] 2 hours ... - Medscape](https://img.yumpu.com/43645244/1/190x245/nih-stroke-scale-interval-1-baseline-2-2-hours-medscape.jpg?quality=85)