Mineral Homeostasis in CKD - Mineral and Bone Disorder - Medscape
Mineral Homeostasis in CKD - Mineral and Bone Disorder - Medscape
Mineral Homeostasis in CKD - Mineral and Bone Disorder - Medscape

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
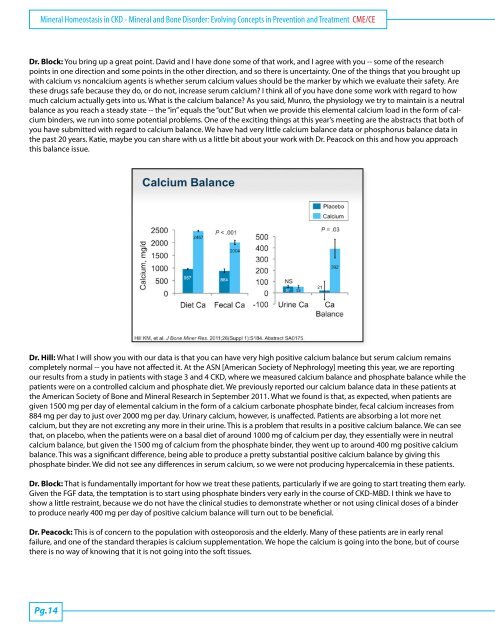
<strong>M<strong>in</strong>eral</strong> <strong>Homeostasis</strong> <strong>in</strong> <strong>CKD</strong> - <strong>M<strong>in</strong>eral</strong> <strong>and</strong> <strong>Bone</strong> <strong>Disorder</strong>: Evolv<strong>in</strong>g Concepts <strong>in</strong> Prevention <strong>and</strong> Treatment CME/CEDr. Block: You br<strong>in</strong>g up a great po<strong>in</strong>t. David <strong>and</strong> I have done some of that work, <strong>and</strong> I agree with you -- some of the researchpo<strong>in</strong>ts <strong>in</strong> one direction <strong>and</strong> some po<strong>in</strong>ts <strong>in</strong> the other direction, <strong>and</strong> so there is uncerta<strong>in</strong>ty. One of the th<strong>in</strong>gs that you brought upwith calcium vs noncalcium agents is whether serum calcium values should be the marker by which we evaluate their safety. Arethese drugs safe because they do, or do not, <strong>in</strong>crease serum calcium? I th<strong>in</strong>k all of you have done some work with regard to howmuch calcium actually gets <strong>in</strong>to us. What is the calcium balance? As you said, Munro, the physiology we try to ma<strong>in</strong>ta<strong>in</strong> is a neutralbalance as you reach a steady state -- the “<strong>in</strong>” equals the “out.” But when we provide this elemental calcium load <strong>in</strong> the form of calciumb<strong>in</strong>ders, we run <strong>in</strong>to some potential problems. One of the excit<strong>in</strong>g th<strong>in</strong>gs at this year’s meet<strong>in</strong>g are the abstracts that both ofyou have submitted with regard to calcium balance. We have had very little calcium balance data or phosphorus balance data <strong>in</strong>the past 20 years. Katie, maybe you can share with us a little bit about your work with Dr. Peacock on this <strong>and</strong> how you approachthis balance issue.Dr. Hill: What I will show you with our data is that you can have very high positive calcium balance but serum calcium rema<strong>in</strong>scompletely normal -- you have not affected it. At the ASN [American Society of Nephrology] meet<strong>in</strong>g this year, we are report<strong>in</strong>gour results from a study <strong>in</strong> patients with stage 3 <strong>and</strong> 4 <strong>CKD</strong>, where we measured calcium balance <strong>and</strong> phosphate balance while thepatients were on a controlled calcium <strong>and</strong> phosphate diet. We previously reported our calcium balance data <strong>in</strong> these patients atthe American Society of <strong>Bone</strong> <strong>and</strong> <strong>M<strong>in</strong>eral</strong> Research <strong>in</strong> September 2011. What we found is that, as expected, when patients aregiven 1500 mg per day of elemental calcium <strong>in</strong> the form of a calcium carbonate phosphate b<strong>in</strong>der, fecal calcium <strong>in</strong>creases from884 mg per day to just over 2000 mg per day. Ur<strong>in</strong>ary calcium, however, is unaffected. Patients are absorb<strong>in</strong>g a lot more netcalcium, but they are not excret<strong>in</strong>g any more <strong>in</strong> their ur<strong>in</strong>e. This is a problem that results <strong>in</strong> a positive calcium balance. We can seethat, on placebo, when the patients were on a basal diet of around 1000 mg of calcium per day, they essentially were <strong>in</strong> neutralcalcium balance, but given the 1500 mg of calcium from the phosphate b<strong>in</strong>der, they went up to around 400 mg positive calciumbalance. This was a significant difference, be<strong>in</strong>g able to produce a pretty substantial positive calcium balance by giv<strong>in</strong>g thisphosphate b<strong>in</strong>der. We did not see any differences <strong>in</strong> serum calcium, so we were not produc<strong>in</strong>g hypercalcemia <strong>in</strong> these patients.Dr. Block: That is fundamentally important for how we treat these patients, particularly if we are go<strong>in</strong>g to start treat<strong>in</strong>g them early.Given the FGF data, the temptation is to start us<strong>in</strong>g phosphate b<strong>in</strong>ders very early <strong>in</strong> the course of <strong>CKD</strong>-MBD. I th<strong>in</strong>k we have toshow a little restra<strong>in</strong>t, because we do not have the cl<strong>in</strong>ical studies to demonstrate whether or not us<strong>in</strong>g cl<strong>in</strong>ical doses of a b<strong>in</strong>derto produce nearly 400 mg per day of positive calcium balance will turn out to be beneficial.Dr. Peacock: This is of concern to the population with osteoporosis <strong>and</strong> the elderly. Many of these patients are <strong>in</strong> early renalfailure, <strong>and</strong> one of the st<strong>and</strong>ard therapies is calcium supplementation. We hope the calcium is go<strong>in</strong>g <strong>in</strong>to the bone, but of coursethere is no way of know<strong>in</strong>g that it is not go<strong>in</strong>g <strong>in</strong>to the soft tissues.Pg.14




![NIH STROKE SCALE Interval: 1[ ] Baseline 2[ ] 2 hours ... - Medscape](https://img.yumpu.com/43645244/1/190x245/nih-stroke-scale-interval-1-baseline-2-2-hours-medscape.jpg?quality=85)