TransformaTions - LV Prasad Eye Institute
TransformaTions - LV Prasad Eye Institute
TransformaTions - LV Prasad Eye Institute
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
a nETwork of EyE CarE for aLL<strong>LV</strong> <strong>Prasad</strong> <strong>Eye</strong> <strong>Institute</strong> is a comprehensive eye health facility with its main campus located in Hyderabad,India. A World Health Organization Collaborating Centre for Prevention of Blindness, the <strong>Institute</strong>offers comprehensive patient care, sight enhancement and rehabilitation services and high-impact ruraleye health programs. It also pursues cutting edge research and offers training in human resources for all levelsof ophthalmic personnel.<strong>LV</strong>PEI’s mission is to provide equitable and efficient eye care to all sections of society. In the past 21 years we haveprovided outpatient services to 4 million people and surgical care to over 400,000 patients - 50 percent of themfree, regardless of complexity. We have trained over 10,000 eye care personnel from India and abroad.The <strong>LV</strong>PEI system is now a network that spans two tertiary centres in Bhubaneswar and Visakhapatnam, and68 secondary and primary care centres that cover the remotest rural areas in the state of Andhra Pradesh,India. <strong>LV</strong>PEI is a not-for-profit organization governed by two trusts: the Hyderabad <strong>Eye</strong> <strong>Institute</strong> and theHyderabad <strong>Eye</strong> Research Foundation.Each day, hundreds of people who cannot afford eye care, receive care from some of the best eye healthprofessionals, while hundreds more benefit from <strong>LV</strong>PEI’s rural affiliates and satellite clinics in urban slums.These centers have seen almost 1.5 million outpatients in Andhra Pradesh alone, and over 50% have beentreated free. Of more than 150,000 surgeries, more than two-thirds have been done absolutely free of cost. Ourrural and urban community eye health programs include surveys of over 3,500 villages with a total populationof over 2 million. Teams of community eye health workers including local volunteers have conducted over1200 community screening and 800 school screening programs. The services provided, apart from surgeries,include prescription of spectacles, follow-up visits, referrals, training and community rehabilitation. <strong>LV</strong>PEI isalso involved in monitoring quality of cataract surgery in 80 Rotary hospitals in India. At the tertiary level, wework with 8 centres in India, and internationally, in 10 secondary and tertiary centres at different levels ofcapacity building.international Centre for advancement of rural <strong>Eye</strong> careThe International Centre for Advancement of Rural <strong>Eye</strong> care (ICARE) was founded in 1998, and is an integral partof the <strong>Institute</strong>. <strong>LV</strong>PEI’s community eye care services are planned and managed by ICARE. <strong>LV</strong>PEI has been involvedin developing eye care services in those areas of Andhra Pradesh and other parts of India where such facilitiesare neither available nor well developed. ICARE is an organized large-scale effort to reduce blindness in rural andunreached India, and other parts of the developing world, over the long term. ICARE was established with thesupport of Christoffel-Blindenmission of Germany and Sightsavers International of United Kingdom.2
a TUrning PoinT in BLinDnEss PrEVEnTionThe andhra Pradesh <strong>Eye</strong> Disease study (aPEDs)much of the learning that L V <strong>Prasad</strong> <strong>Eye</strong> <strong>Institute</strong> has gained over the past ten years ormore about preventable blindness and vision impairment has come from a seminal studyplanned and conducted by researchers at the <strong>Institute</strong> between the years 1996 and 2000.Now widely recognized as the first scientifically designed epidemiological study of this nature inthe developing world, the Andhra Pradesh <strong>Eye</strong> Disease Study helped <strong>LV</strong>PEI define and crystallize asustainable model of eye care service delivery that focused on the creation of permanent infrastructureand adequately trained human resources at all levels, from the advanced tertiary to the community.The study provided the basis for a new approach to eye care policy and its implementation in Indiaand the developing world.The Andhra Pradesh <strong>Eye</strong> Disease Study (APEDS) was conducted between 1996-2000, with theobjective of determining the prevalence of eye disease and burden of blindness and visual impairmentin state of Andhra Pradesh, a southern Indian state. Related objectives were to identify risk factorsfor major eye diseases, the impact of blindness and visual impairment on quality of life and barriersto the uptake of eye care services. Four areas, which together are a reasonable representation ofthe socio-economic and urban-rural distribution of the population of Andhra Pradesh were chosento obtain the sample for the study.These are Hyderabad (urban), WestGodavari (a relatively prosperous ruralarea), Adilabad and Mahaboobnagardistricts (both relatively backwardrural areas) . Overall, the study foundthat prevalence of blindness in AndhraPradesh was 1.84 % across all agegroups; i.e., approximately 1.5 millionpeople are blind in Andhra Pradesh.However, the prevalence of blindnessvaried across the region, from 1.36-2.40%.findings from aPEDs: HighlightsBlindness: The major causes of blindness were Cataract (44%), Refractive Errors (16.3%), RetinalDisease (10.9%), Glaucoma (8.2%), and Corneal Disease (7.1%). Nearly 70-75% of this blindness wasavoidable.Vision impairment: In addition, another 8.5% of the population has significant vision impairment.Among the causes for vision impairment, 45% were due to refractive errors and 40% due tocataract.The study established that blindness and visual impairment increased with age, was more common in females,among people lower socio-economic strata and in rural areas.Low vision: In addition, 1.05% of the population has low vision, the major causes being retinaldiseases (35.2%), amblyopia (25.7%) and optic atrophy (14.3%).Altogether in Andhra Pradesh, over 8 million people are in need of eye care if they are to carry out theirnormal activities independently and an additional 800,000 require some type of visual aid.3
Cataract: Though the majorfocus of the National Programfor Control of Blindness hashistorically been cataract, thestudy threw up certain issuesrelated to the outcome and qualityof cataract services.refractive error: APEDS, forthe first time in the world, showedthat uncorrected refractive errorwas one of the major causes ofblindness and the major causeof vision impairment. The overallprevalence of presbyopia above 30years was found to be 55.3% andonly one-third of those affectedwere found to be using presbyopicglasses.glaucoma and Diabeticretinopathy: Glaucoma anddiabetic retinopathy were foundto be emerging causes of blindnessand visual impairment with majorissues being lack of awareness,both among physicians as well asthe public. More th an 90% wereunaware of these diseases and someof them remained unaware despitehaving visited an ophthalmologist.The major risk factors for diabeticretinopathy were found to beincreasing age and duration ofdiabetes, urban residence, middleand upper socio-economic groupand hypertension. The major riskfactors for glaucoma were age andincreased intraocular pressure.Barriers: It was found thatutilization of eye care serviceswas less common in rural areasthan in urban areas (29.6% versus45.3%) with a major barrier beingaffordability (37%).4
efractive Error in Children in a rural Population in indiaFollowing the APEDS study, the group of epidemiologists and public health specialistsat <strong>LV</strong>PEI assisted by others continued their exploration of some of the key issuesrelated to the prevalence of blindness and vision impairment, particularly amongvulnerable populations such as the elderly and children.Refractive error is one of the most common causes of visual impairment aroundthe world and the second leading cause of treatable blindness. Though thereare a few studies on the prevalence and distribution of refractive errors frompopulation-based surveys in adults, similar data on children is very limited.To address the lack of strictly comparable, representative data, a series ofpopulation-based surveys in children 5 to 15 years of age were jointly initiatedin 1998 by the World Health Organization and the National <strong>Eye</strong> <strong>Institute</strong>. Usingthe same protocol, we conducted the Refractive Error Study in Children (RESC)in populations with different ethnic origins and environmental settings — ruralJhapa district in eastern Nepal; semi rural Shunyi District, near Beijing, China;La Florida, an urban area of Santiago, Chile; rural Mahabubnagar district nearHyderabad, in southern India; an urban area of New Delhi, India; semi rural/urban area of Durban, South Africa; an urban area of Guangzhou, China; andGombak district in Kuala Lumpur, Malaysia. The RESC survey in Mahabubnagardistrict was conducted by ICARE from April 2000 to February 2001.Refractive error was identified as the main cause of visual impairment in childrenaged between 7 and 15 years in rural India. There was a benefit of spectaclesin 70% of those who had visual acuity of 20/40 or worse in the better eye atbaseline examination. Because visual impairment can have a significant impacton a child’s life in terms of education and development, it is important thateffective strategies be developed to eliminate this easily treated cause of visualimpairment.The foundations of iCarEAPEDS laid the foundation for developing a plan to effectively control blindnessin Andhra Pradesh, to begin with, and to build an approach to tackling avoidableblindness across the developing world, where much of the context is similar.Information from APEDS also led to the development of the Pyramidal Modelof eye care service delivery, addressing concerns of equity and quality within ahigh-quality, sustainable framework. RESC on the other hand, helped us developa program to address vision impairment due to uncorrected refractive error inchildren of school going age, now one of ICARE’s major focus areas.These and other related studies have served to build a strong foundation ofunderstanding that feeds our work in advocacy, training, service delivery andinfrastructure development in the regions where we have a presence. It is suchongoing epidemiological work that continues to inform and direct the workof <strong>LV</strong>PEI, through ICARE, to serve the most disadvantaged populations in thedeveloping world.5
THE PyramiD moDEL<strong>LV</strong>PEI has developed the pyramidal model for eye care service delivery from community level VisionCentres for primary care (1:50,000) to the Centre of Excellence level for advanced tertiary care(1:50 million). This model has been successfully implemented in several districts of Andhra Pradeshand lends itself globally to adaptations and possible modifications as per the local need under the ‘VISION2020: The Right to Sight’ global initiative for elimination of avoidable blindness. The Government of Indiahas adopted the <strong>LV</strong>PEI model of Vision Centres for rural areas for implementation across the countryand allocated funds for it.The pyramid model directly addresses the problem of avoidable blindness in India. Since the majority ofblind people in India live in rural areas, the most effective approach is to develop the widest possiblenetwork of rural eye care centers, staffed by trained eye health workers.Towards this <strong>LV</strong>PEI developed a comprehensive eye care model, which was subsequently adopted bythe VISION 2020: Right to Sight program of the International Agency for the Prevention of Blindness(IAPB). The pyramid service model aims at providing high quality and sustainable eye care in rural andunderserved urban areas, by setting up new eye care centers while upgrading existing facilities, thuscreating a network of services that are integrated with the local community infrastructure.The VISION 2020 service model is envisaged as a pyramid, bringing a wide network of eye care facilities inunderserved areas under the umbrella of a state-of-the-art eye <strong>Institute</strong> with tertiary care facilities, trainingprograms, research facilities, and a resource center for infrastructure development and rehabilitation.The model meets the criteria of availability, affordability, and accessibility of preventive, curative, andrehabilitative eye care services.Vision guardiansA vision guardian is a volunteer from the community working as a liaison between the service providers(Vision Centres) and the community. His/her primary job is to “keep an eye on the eye health of the people”.Any person, preferably with basic reading and writing skills, can be trained as a vision guardian. Most ofthem are selected in partnership with local self help groups and other community organizations.Vision CentresThe Vision Centre (VC) model was launched in 2002, and was initially supported by Sight SaversInternational (United Kingdom) and, more recently, by the Lavelle Fund of New York, Inc., USA andLatter-day Saint Charities, Salt Lake City, USA.Vision Centres (VC) form the base of the pyramid. Each VC is staffed by a vision technician, who isrecruited from the local community and trained by <strong>LV</strong>PEI for one year. The VCs perform ophthalmicevaluation, refraction, dispense spectacles and diagnose potentially blinding diseases. They also conducthealth education progams.service CentresService Centres are secondary care centers, which offer comprehensive outpatient and surgical services,including community based rehabilitation and low vision care. They undertake preventive eye care programsand serve as an eye donation centre. The same high quality eye care services are provided to both payingand non-paying patients. Each Service Centre aims to be financially self-sufficient within three years,through the following approach: Fifty percent of the services are paid by patients who have the ability topay in a three-tier fee structure. The remaining 50 percent services are provided free to underprivilegedpatients. Experience has shown that the centres can provide services to 70 percent non-paying and 30percent paying patients and yet be self-sustainable.8
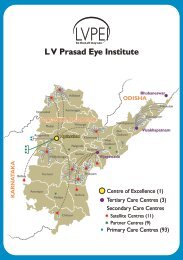
oUr rEaCH anD rangEINDIAvvvvIndia Partners: Tertiary CentresSuryodaya <strong>Eye</strong> Centre, KolkataC L Gupta <strong>Eye</strong> <strong>Institute</strong>, Moradabad, Uttar PradeshMGM <strong>Eye</strong> <strong>Institute</strong>, Raipur, ChattisgarhAlakh Nayan Mandir <strong>Eye</strong> <strong>Institute</strong>, UdaipurIndia Partners: Secondary Centres<strong>LV</strong>PEI - OEU Collaborating hospitals<strong>LV</strong>PEI - Rotary Partner hospitalsChandra Prabha <strong>Eye</strong> Hospital, Jorhat, AssamBausch & Lomb Advanced Cataract Centre, Haldwani,UttaranchalBausch & Lomb Advanced Cataract Centre, Sri Ganga NagarAndhrA PrAdesh9
‘ParTnEring’ a soLUTionThe accompaniment ProgramICARE’s accompaniment program envisages working with ‘partner eye centres’ in underserved areas forfour years. Shorter or longer engagement periods may be planned depending on specific need, feasibilityand resource availability. ICARE provides strategic and technical assistance to establish standardizedsystems of patient care and hospital management, along with effective community eye care programsamong the target population.iCarE works with the partner eye hospital in:• designing the facility and selecting equipment,• developing human resources,• planning service delivery and financial sustainability, and• planning community eye health programs and operations research.in line with <strong>LV</strong>PEI’s intensive engagement at all levels of service delivery, ICARE has developed an to-end capacity building program that addresses the need for eye care services by bridging demand,end-need and capability to deliver. Working with partner eye care hospitals and development agencies,ICARE provides strategic and technical assistance to establish standardized systems of patient care,hospital management and community eye care programs in areas of need.operation <strong>Eye</strong>sight Universal CEo Pat fergusonopens an <strong>LV</strong>PEi Vision CentreDesigning the facility and selecting equipmentICARE advises partners on the technical aspects and feasibility of the infrastructure, including microdetailssuch as floor plans and architectural design. It facilitates the implementation of the design, workingclosely with architects and contractors. ICARE also assists partners in selecting and negotiating prices forall equipment and infrastructural needs.Developing human resourcesICARE works with the partner to identify and plan human resources for the facility, with an eye to providingcomprehensive eye care. It works in close engagement with the partner and other stakeholders in thecommunity to develop a full complement of eye care workers, covering all cadres.The emphasis is on bringing on board clinical, para-clinical and administrative personnel to build a strong team thatcan handle the gamut of operations right from community mobilization to patient handling to clinical and postclinicalservices.10
Planning service delivery and financial sustainabilityThe program helps put in place mechanisms to ensure optimization of services and achievement offinancial sustainability. The focus is on achieving a balance between financial sustainability and making freetreatment available to those who cannot pay.Planning community eye health programs and operations researchICARE also works with the partner to implement the <strong>LV</strong>PEI pyramidal model of eye care service deliveryfor a target population. This includes mechanisms of community mobilization and generation of humanand material resources from the community so as to encourage ownership of health care, and follow upresearch to monitor the effectiveness of interventions.The Partnership impactStarted in 1994, with a secondary centre in West Godavari District in Andhra Pradesh, ICARE has doneextensive capacity building (3 year’s accompaniment program) with 15 secondary care hospital in state ofAndhra Pradesh. As a resource centre for Operation <strong>Eye</strong>sight Universal (OEU), ICARE is involved extensivelyin capacity building of their partner hospitals in India (close to 15 hospitals), apart from engagement withseveral other secondary and tertiary centres. <strong>LV</strong>PEI is also involved in monitoring quality of cataract surgeryin 80 Rotary hospitals in India. At the tertiary level, <strong>LV</strong>PEI is working with 8 centres in India. Internationally<strong>LV</strong>PEI in involved with 10 secondary and tertiary centres at different levels of capacity building.At the primary level, <strong>LV</strong>PEI has a network of 51 vision centres in Andhra Pradesh. Apart from this <strong>LV</strong>PEI hasdeveloped network of vision centres with some of their partners and is also involved in training of trainers forvision centres project with Standard Charted Bank (SCB) (40 vision centres at 4 different locations in India).The concept of <strong>LV</strong>PEI Vision Centres have been adopted by the Government of India for development of 3000vision centres and by the Australian Government for developing vision centres for S-E Asia.andhra Pradeshimpact of service Centres• Covers13 districts and 10 million population in around7500 villages• 100% comprehensive eye examination done• 1.5 million out-patients seen and 150,000 sight restoringsurgeries performed• 60% out-patients and 75% surgeries performed free of cost• More than 90% have good outcomes (equal to or betterthan 6/18)• 75% having more than 100% cost recoveryimpact of Vision Centres• Covering 6 districts reaching 3 million population inaround 600 villages and seen 2,50,000 out-patients• 80,000 spectacles prescribed, 60,000 spectaclesdispensed and 50,000 Patients referredimpact of community eye care (CEC) activities• Door-to-door survey done in 3500 villages• 3 million population surveyed with 700,000 identifiedwith eye problem• 200,000 screened, 70,000 glasses prescribed and30,000 referred• 125000 children screened in 800 school covered• 13000 identified with eye defects, 3000 prescribedspectacles and 3500 referred• Rehabilitation done for 1500 subjectswith fullerton india• 12 screening programs with 6200 people screened• 2700 spectacles dispensed and 2000 peoplereferrednationalwith oEU (since 2003)• Resource centre for OEU covering 10 states• 2.5 million out-patients seen and 250,000 sightrestoring surgeries performed• 60% out-patients and 50% surgeries performed freeof cost• 60% increase in out-patients and 50% increase insurgical output• More than 100% increase in total revenue since 2005• More than 500% increase in optical and pharmacyrevenuewith rotary (since 2005)• 600,000 outpatients screened and 60,000 sightrestoring surgeries performed11
iCarE ProjECTss no.ProjectPrincipalinvestigatorssupported byDuration1Community Assisted and Financed <strong>Eye</strong> care(CAFE)Dr Giridhar Pyda<strong>Eye</strong> SightInternational, CanadaApril 2001 toFebruary 20062Impact of Cataract Surgery on Quality oflife - a Qualitative StudyMr.Vilas Kovai Sightsavers International 2004 - 20053Providing <strong>Eye</strong> care through EmpoweredPeople (PEEP)Mr ShubhrakantiBhattacharyaORBIS InternationalJune 2004 toDecember 20074Capacity building program for themanagement of diabetic retinopathy in thestate of Andhra PradeshDr Taraprasad DasDr Annie MathaiMs S SheeladeviLions Club InternationalFoundationAugust 2005to July 200856Comprehensive <strong>Eye</strong> Health program inPrakasam districtImpact Assessment Study after refractionerror correction among schoolgoingchildrenICARE teamMr Jachin D Williams7 Sight for Kids Mr Jachin D Williams8Diabetes prevention program throughChild to Family Communication forchange in lifestyle and health promotion inPrakasam districtMs S SheeladeviMs Jayanthi SagarRaavi Brothers, USAVision CRC, AustraliaLions Club InternationalFoundationWorld DiabetesFoundationAugust 2005to July 2010September 2005to December 2008November 2005to March 2009April 2006to March 20119Child to Child and Child to Familycommunication as a strategy to improveawareness and uptake of eye care servicesMr D KiranVision CRC, AustraliaApril 2006to December 200810Pediatric Ophthalmology Learning andTraining Centre (POLTC)Dr Giridhar PydaDr Ramesh MurthyORBIS International,IndiaOctober 2006to March 201011Rapid assessment of cataract surgicalservices in Service Centre areasMr M Srinivas<strong>LV</strong>PEIAt regularintervals12Nimmagadda <strong>Prasad</strong> – <strong>LV</strong>PEI Children’s <strong>Eye</strong>Health InitiativeMs S SheeladeviMr ShubhrakantiBhattacharyaNimmagaddaFoundationJuly 2007 to June 202013Community Linkage for Integration ofPrimary Health (CLIP)Dr Syed Imtiaz AhmedMr ShubhrakantiBhattacharya<strong>LV</strong>PEIAugust 2008to December 200914Rapid Assessment of Refractive Errors(RARE)Mr Srinivas MarmamulaDr Jill E KeeffeDr Gullapalli N Rao<strong>LV</strong>PEIAt regularintervals15Capacity building program to addressDiabetes and Diabetic retinopathy inPrakasam DistrictDr Ajit Babu MajjiMs S SheeladeviWorld DiabetesFoundationSeptember 2008 toAugust 201312
Developing Comprehensive modelsOur approach to developing new and more comprehensive approaches to eye care service delivery are based on learning froma variety of studies, some of which are profiled here. We have also looked at qualitative indicators of service outcomes, such ashow quality of life has been impacted by cataract surgery. The understanding gained from these studies is applied to the way webuild services and train people to deliver them.Comprehensive <strong>Eye</strong> Health ProgramThe objective of the comprehensive eye health program is to reduce the magnitude of blindness in Prakasamdistrict from its estimated 1.84% to less than 0.3% during a five year period, by providing comprehensive eyecare services. This is a comprehensive approach incorporating preventive, curative and rehabilitation services andis supported by Sudhakar and Sreekanth Ravi of California, USA. The project duration is from August 2005 to July2010. The objective of the program is to provide high quality, sustainable, comprehensive eye care by developingprimary and secondary level service providers, developing innovative community participatory programs to aiduptake of services, integrating components of primary health care and primary eye care, and utilizing managementand geographic information systems to aid service delivery.Capacity development program to address diabetes and diabetic retinopathyThis project aims at strengthening the existing infrastructure and building capacity to help better the quality oflife of persons with diabetes in Prakasam district, Andhra Pradesh state, India. It will adopt a multidisciplinaryapproach (including modification in lifestyle, special diabetes oriented care of feet, eyes, etc) and emphasize strongpublic and private partnerships (among <strong>LV</strong>PEI, district health administration and private practitioners) with effectivecommunity integration and participation within the district. The World Diabetes Foundation is supporting theproject for a period of 5 years (2008 to 2013). The objectives include:• Developing a registry of all persons with diabetes in the district and ensure continuous follow up,• Strengthening the capacity of public health facilities and not-for-profit organizations at the district level for care of personswith diabetes and diabetic retinopathy,• Establishing a working network of specialists both in public and private sector for specialties like cardiology, nephrology,care of feet and retina,• Education and training of paramedics, general physicians, village volunteers, ophthalmologists and mid level ophthalmicassistants, and• Facilitating annual comprehensive diabetic screening programs.This project started on October 1, 2008, and was officially launched on November 14, 2008.`13
Diabetes prevention program through Child to family CommunicationThis program was launched in Prakasam district (Andhra Pradesh) in May 2006 and is supported by the WorldDiabetes Foundation. It aims at developing a sustainable district level model to promote lifestyle changes in ruralAndhra Pradesh using the child-to-family communication strategy. Diabetes being a major public health problem, withalarming increases in its prevalence, there is an urgent need for interventions in lifestyle to prevent an epidemic of diabetes. Thedisease is also a major factor in causing many retinal eye diseases. The project duration is from April 2006 to March 2011.june 2006 – september 2008Project PerformanceTraining programsSchoolchildren trained 1,02,017Teachers trained 7,043CoverageSchools covered 598Villages covered 413Mandals covered 44Training programsPrimary Health Centers doctors 74NGOs 156Self help group representatives 28, 542Self help groups 1,029screening by trained childrenFamilies 4,57,732Persons 20,37,763High risk persons identified and screened for blood and urine sugar 97,400Screened persons suspected to have diabetes 6,264sight first – 1141: Lions – <strong>LV</strong>PEi capacity development project for diabetic eye diseaseBlindness due to diabetes is a major eye health concern; almost two-thirds of persons with diabetes have a highpotential for vision loss. To address the problem of diabetic retinopathy in the state of Andhra Pradesh, <strong>LV</strong>PEIlaunched a 3-year capacity building program for 18 eye hospitals, with support from Lions Club International. Theproject was launched in August 2005.The objectives of the Sight First – 1141 project are to generate awareness about eye diseases associated withdiabetes, provide comprehensive treatment for persons with diabetic retinopathy, build the capacity of partnerhospitals through training of personnel at various levels, and set up a dedicated training infrastructure at <strong>LV</strong>PEI.14Project performance – service delivery (2005 to 2008)General diabeticpatientsDiabetic retinopathyeyes identifiedLasersSurgeryOutreachprogramsPartners 19,414 11,234 1,546 0 508<strong>LV</strong>PEI 11,003 6,594 3,902 1,946 25Total 30,417 17,828 5,448 1,946 533Training Programs Target # for 3 years # Enrolled # CompletedShort-term fellowship 18 9 9Long-term fellowship 3 1 1Mid level ophthalmic personnel (MLOP) 18 16 15Community workers 18 14 14Total 57 40 39Knowledge, attitude and practice studies were done in all the partner areas in 2006 and 2008 to assessthe baseline and plan modifications over a period of 2 years in the service area.
Eliminating Childhood Blindnessnimmagadda <strong>Prasad</strong> – <strong>LV</strong>PEi Children’s <strong>Eye</strong>Health initiativeanother major initiative to address childhood blindness is theNimmagadda <strong>Prasad</strong> – <strong>LV</strong>PEI Children’s <strong>Eye</strong> Health Initiative,supported by the Nimmagadda Foundation. Launched on July7, 2007, the initiative aims at preventing childhood blindness sothat “No child in Andhra Pradesh is needlessly blind or visuallyimpaired by the year 2020”.The Nimmagadda Foundation offers support in the areas ofinfrastructure development, screening and treatment includingspectacles, awareness generation, development of information,education and communication (IEC) material, training and othercommunity based programs.july 2007 to september 2008Outpatients (Non-paying) 32,209Surgical procedures (Non-paying) 4,987Spectacles distributed 1,328Teachers trained 1,403Children screened at schools 39,990Schools covered 174Pediatric ophthalmology Learning and Training Centresome of the major hurdles in the elimination of avoidable childhood blindness are shortage of skilled humanresources to address pediatric eye diseases, inadequate infrastructure and lack of good anesthesia and paraophthalmicsupport. To address these concerns in India and south-east Asia ORBIS has set up three PediatricOphthalmology Learning and Training Centres (POLTC) at Sanka ra Netralaya, Aravind, and L V <strong>Prasad</strong> <strong>Eye</strong> <strong>Institute</strong>,Hyderabad, in October 2006. The objectives of the 3½-year POLTC program are:Training 5 pediatric eye care teams for ORBIS India partners. Each team of 6 personnel (ophthalmologist,anesthetist, optometrist, nurse, counselor, and an outreach coordinator) will empower one institution inpediatric ophthalmology.• Examination of 25,000 children, treatment for 2500 and surgeries for 975 children• Enhancing capacity of the 2 ORBIS supported partners in pediatric ophthalmology• Provision of 450 free spectacles• Support in skill development of pediatric ophthalmology faculty of <strong>LV</strong>PEI• Offering research and participation opportunities at national/international conferences and workshopsTwo batches completed training by 30th September 2008. Training of third batch is continuing. Trainees arebeing involved in presentations, publications and research activities.january 2007 to september 2008Children examined 73,272Children treated 6,597Surgeries performed 9,344Number of school screening programs 21Pediatric Hospital Based Program 0115
sight for kidsstructured approach to address childhood blindness needs early detection of eye ailments among children. Thisa is the objective of the Sight for Kids project, which is supported by the Lions Clubs International Foundation(LCIF) and Johnson & Johnson. <strong>LV</strong>PEI’s role is of designer, coordinator and implementing partner. The objectivesare:• Training schoolteachers to identify children with eye problems,• Training teachers to screen and identify children with vision defects and eye conditions and refer them forappropriate care,• Detailed eye examination of all referred children by ophthalmic personnel,• Providing appropriate response in the form of spectacles, treatment, surgery or vision rehabilitation,• Empowering teachers to create awareness on eye health and care, and• Implementing sustainable eye health program in schools.In three years, the program has trained ophthalmic assistants and trainers of schoolteachers for 8 partner eye facilitiesin Hyderabad. Posters on eye health awareness, screening kits and teachers’ screening manual were distributed inthe schools covered.impact assessment studynovember 2005 to september 2008Number of schools 505Teachers trained 667Children screened by the trained teachers 47,270Identified with eye problems 724Referred for further screening 490Free spectacles dispensed 219Treated for other eye conditions 282The ‘Impact of correction of refractive errors among children aged 10 to 15 years on activity-based performance andother vision-based functions in the state of Andhra Pradesh’ research study under taken by ICARE – <strong>LV</strong>PEI aimsto provide information on the impact of refractive error correction on the life of schoolchildren and use of spectacleswithin the existing system.The exercise aims to assess the benefits in terms of improved ability to perform routine activities, which in turn improvesquality of life. It also studies the percentage of compliance when advised spectacles and the barriers in procuring them.This study is being conducted under the aegis of the Vision Cooperative Research Centre (Vision CRC) of Australia.Subjects for the study were recruited from 31 schools from four locations in Andhra Pradesh – Hyderabad, Adilabad,Mahabubnagar and Prakasam districts, where <strong>LV</strong>PEI’s secondary and primary eye care centres are situated.Of these, 310 subjects were recruited for the study and baseline data collection was completed by interviewing 310subjects, 310 parents of the subjects, 310 teachers and 930 peers.16
Empowering rural CommunitiesCommunity assisted and financed <strong>Eye</strong> care (CafE)for people in rural areas, healthcare comes with many direct and indirect costs. <strong>LV</strong>PEI, with support from<strong>Eye</strong> Sight International (ESI), Canada, implemented a universal affordable, continuous self-sustaining modelto provide eye care to all members of a community, irrespective of socio-economic status. This project alsoaimed to address a major barrier identified in APEDS: affordability of services.The novel experiment was initiated in 16 villages of West Godavari district in Andhra Pradesh for a population of50,000. Field workers collected a payment of Re 1 per family per month for a year, to build a community fund. Thisincluded a complete eye examination at a secondary eye centre including cataract surgery with intraocular lens(IOL) and minor surgeries. Beneficiaries were given photo identity cards with payment details. The service providerwas initially reimbursed through the grant money on verification of records of service delivery.The registration process started on 11 th Oct 2001 (World Sight Day) and lasted till 31 st May 2005. It was renewedevery year till 31 st May 2005 and service delivery by the base hospital was made available till 28 th February 2006.More than 70% of the population in the villages registered, of which 65% utilized hospital services, with 23,459outpatients visiting the hospital. A total of 2447 children between the ages of 6 and 15 were examined. Over2000 cataract surgeries with IOL were performed. The project made eye care services accessible to many whomight otherwise have not received treatment and helped identify specific barriers that are now being takeninto account while refining the model in another district of the state.Providing <strong>Eye</strong> care through Empowered People (PEEP)The Providing <strong>Eye</strong> Care through Empowered People (PEEP) was a community financed and assisted eyecare scheme offering quality primary and secondary eye care services to the population through theirparticipation and eventual ownership, leading to sustainability. It is based on the concept of community selfpayment,risk pooling and sharing.The project objectives were:• To provide quality and affordable eye care services through a community financed approach,• To facilitate community participation in providing eye care services, and• To empower the community towards gradual ownership of the eye care service project17
The main strategies followed were:Family registration through payment of Re 1 per person per month for a minimum of one year. Services wereavailable for registered members at no further cost for the period of registration.Implementation of the project in partnership with local self help groups (SHG)/federations/community basedorganizations/other organized groups and through trained vision guardians.An integrated approach was used by using community eye care, school screening programs, and Vision Centres.The project was implemented in four mandals around <strong>LV</strong>PEI’s first satellite facility, Bhosle Gopal Rao Patel <strong>Eye</strong>Centre, Mudhol in Adilabad district, with support from ORBIS International (India country office) and technicalinputs from Andhra Pradesh Mahila Abhivruddhi Society, Hyderabad, along with a partner organization SwamiVivekananda Youth Movement in Saragur, Karnataka. The service cost recovery for the project has been 86%through self-payment by the community members.october 2004 to june 2008People registered 34,327Households registered 8,214Outpatients treated at Service Centres 3,693Surgeries at Service Centres 772Patients visited Vision Centres 2,304People renewed for 2nd year 8,795Households renewed for 2nd year 2,021People renewed for 2nd and 3rd years 6,478Households renewed for 2nd and 3rd years 1,448Vision guardians trained 97SHG members trained 1,065Teachers trained 153Community Linkage in integration of Primary Health (CLiP)The Community Linkage in Integration of Primary Health (CLIP) project is an attempt to study how <strong>LV</strong>PEI plays a vitalrole in providing affordable, accessible and quality healthcare to the community in its service area. <strong>LV</strong>PEI’s pyramidaleye care model in the state of Andhra Pradesh provides excellent and equitable eye care to the community throughpermanent infrastructure and manpower.The eye care model is comprehensive in terms of controlling all the diseases that contribute to blindness; it has goodgeographical coverage and all the services are provided with appropriate delivery structures, relevant linkages and referrals.However, it was felt that with such a well-developed network of infrastructure and manpower, <strong>LV</strong>PEI could play an evengreater role in providing linkages among various healthcare providers so as to provide quality healthcare at an affordablecost. <strong>LV</strong>PEI’s eye care delivery structure and referral network can be a suitable vehicle for achieving comprehensivehealthcare for all with community involvement, with each tier supporting and implementing each level of activity.<strong>LV</strong>PEI looks forward to playing the role of a facilitator, linking all health services (public and private) and other welfareschemes, such as the Rajiv Aarogya Sri scheme, EMRI and HMRI services. The on-ground service delivery would bedone through Village Health Volunteers (VHV) — a cadre of volunteers from the village, trained by <strong>LV</strong>PEI in preventiveand promotive health care, awareness creation about early detection and referral of cases. These volunteers will ensurelinkage between various healthcare providers and work closely with government machinery. They will help createawareness about community health rights, ensuring active community participation in all activities, thus creating longterm sustainability.18
mapping rural <strong>Eye</strong> Care needsrapid assessment of Cataract surgical servicesCataract, the leading cause of blindness in the developing world, can be treated with surgery, one of the mostsuccessful and cost effective interventions in healthcare. Yet, cataract accounts for 44% of visual impairment inAndhra Pradesh according to the Andhra Pradesh <strong>Eye</strong> Disease Study (APEDS).Surveys were done in two secondary centres catchment population around Seshanna Chennawar <strong>Eye</strong> Centre(SCEC) in Adilabad and Bhosle Gopal Rao Patel <strong>Eye</strong> Centre, (BGRPEC), Mudhol in Adilabad district, using RapidAssessment of Cataract Surgical Services (RACSS) methodology during 2006 – 2007 to assess the prevalence ofcataract blindness and cataract surgical services in persons aged 50 years and older.The prevalence of blindness (using definition of blindness as presenting vision < 6/60 in the better eye) was 7.2%and 8% in SCEC and BGPREC respectively (Table 1). In both places, cataract was the leading cause of blindness,accounting for 88%, and 73% of the total blindness respectively. The cataract surgical coverage for persons for= 6/18 2276 (77.2) 1694 (78.4)
Unaided, aided and pinhole visual acuity was assessed using a Log MAR chart at a distance of 4 meters. Near vision was assessedusing the N notation chart at the subject’s customary working distance. A brief personal interview helped collect demographicinformation such as education level, occupation, use of spectacles (where applicable) and past utilization of eye care services. Allpeople with visual acuity
Training aT iCarETraining impact• 146 Community <strong>Eye</strong> Health Professionals• 59 <strong>Eye</strong> Care Managers• 284 <strong>Eye</strong> Care Program Leaders• 186 Vision Guardians• 750 School teachers trained under CEC Programs• 100 Community <strong>Eye</strong> Health workersTrainees come from all across India and other developing countriesCourseDurationsessioncommencesno. ofcandidatesEligibilityCertificate course: ProgramManagement & Evaluation2 weeks& 6 weeksMid-December 15 - 20Graduates working in eye care with govt.NGOs or the private sector for at least threeyears in a supervisory or higher positionTraining programs for eyecare support staff1 year January 50 per batch Secondary schooling or IntermediateCertificate course inComprehensive Community<strong>Eye</strong> Care & Rehabilitationof Vision Impaired6 weeks Variable10 fieldlevel teammembersPersons working in organizations involvedin health care service delivery and rural andurban community development programs, eyehospitals and other welfare organizations areeligible to apply for the course.Diploma in <strong>Eye</strong> HealthManagementDiploma in Community <strong>Eye</strong>HealthMaster’s in Community <strong>Eye</strong>Health (in collaborationwith the University of NewSouth Wales, Australia)I year June 15 - 206 months January 10 - 15I year January 15Graduates interested in pursuing a career incommunity eye health program managementGraduates with experience in community ordevelopment work; eye care managementexperience is an advantageGraduates with experience in community ordevelopment work and an interest in leadingrural eye care projectsICARE also offers customized programs in a variety of areas related to community health and development,including refresher training for para-clinical eye care staff and training of trainers in community eye health.21
international Centre for advancement of rural <strong>Eye</strong> CareL V <strong>Prasad</strong> <strong>Eye</strong> instituteKismatpur Campus, Don Bosco Nagar PO, Near Kali MandirHyderabad 500 086, IndiaTel: +91 40 30615605, Fax: +91 40 24011293E-mail: icaresecretary@lvpei.orgiCarE acknowledges the support ofmajor supportersChristoffel-Blindenmission• Nimmagadda Foundation, India• Sudhakar Raavi & Sreekanth Raavi, USA• Lavelle Fund for the Blind, USA• Latter-day Saint Charities, USAother supporters• Operation <strong>Eye</strong>sight Universal, Canada• Lions Club International, USA• Vision Co-operative Reasearch Centre, Australia• <strong>Eye</strong> Sight International, Canada• International Centre for <strong>Eye</strong> Health, UK• Fred Hollows Foundation, AustraliaSightsavers International• International Centre for <strong>Eye</strong>care Education,Australia• ORBIS International, USA• World Diabetes Foundation, Denmark• Four Acre Trust, UK• Fullerton India Ltd. India• International Agency for Prevention of Blindness• Andhra Pradesh Right to Sight Society, India• Open Society <strong>Institute</strong>, USA• Canadian International Development Agency, Canada