Clavicle Hook Plate. One implant for two indications. - Osteosyntese
Clavicle Hook Plate. One implant for two indications. - Osteosyntese
Clavicle Hook Plate. One implant for two indications. - Osteosyntese

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
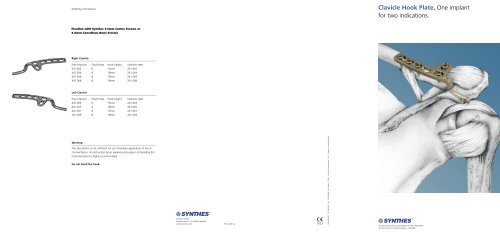
Ordering in<strong>for</strong>mation<strong>Clavicle</strong> <strong>Hook</strong> <strong>Plate</strong>. <strong>One</strong> <strong>implant</strong><strong>for</strong> <strong>two</strong> <strong>indications</strong>.Fixation with Synthes 3.5mm Cortex Screws or4.0mm Cancellous Bone ScrewsRight <strong>Clavicle</strong>Pure titanium Shaft holes <strong>Hook</strong> height Stainless steel441.062 6 15mm 241.062441.064 6 18mm 241.064441.066 8 15mm 241.066441.068 8 18mm 241.068Left <strong>Clavicle</strong>Pure titanium Shaft holes <strong>Hook</strong> height Stainless steel441.063 6 15mm 241.063441.065 6 18mm 241.065441.067 8 15mm 241.067441.069 8 18mm 241.069WarningThis description is not sufficient <strong>for</strong> an immediate application of the instrumentation.An instruction by an experienced surgeon in handling thisinstrumentation is highly recommended.Do not bend the hook.Synthes GmbHEimattstrasse 3, CH-4436 Oberdorfwww.synthes.comPresented by:036.000.821 SE_034300 AA 31050028 © Synthes 2006 Printed in Switzerland LAG Subject to modifications.
<strong>One</strong> <strong>implant</strong> <strong>for</strong> <strong>two</strong> <strong>indications</strong>Surgical stepsSurgical stepsLateral clavicular fracture, Neer type IIAC luxation, Tossy type IIILateral clavicular fracture, Neer type IIAC luxation, Tossy type IIIBenefitsIncisionIncisionImmediate postoperative early functional aftertreatment and mobilisationthanks to the joint-bridging hook.Shape, dimension and screw hole arrangement of the hook plate havebeen designed to fit the anatomy.Surgical exposure by means of an approximately 8 cm sagittal incision, 2cm medial of the AC joint. Transverse incision of the muscular fascia andexact fascia preparation to expose the AC joint and the lateral portion ofthe clavicle.Surgical approach as shown in figure 1. Usually, the lateral clavicle isdecorticated from the acromioclavicular ligament and capsule, and theacromioclavicular ligament and capsule are still fixed to the acromion andjoint disk. Loop retaining sutures around the acromioclavicular ligamentand capsule.LC-DCP screw holes allow dynamic compression of fractures and optimumplate fixation.High-quality AO/ASIF stainless steel <strong>implant</strong>sTitanium <strong>implant</strong>s provide excellent biocompatibility and hardly interfereFigura 1Figura 4with MRI examinations.InsertionInsertionUse bone reduction <strong>for</strong>ceps <strong>for</strong> the temporary fixation. Prepare the platePrepare the plate seat and insert the hook under the acromion, dorsal ofseat and, after palpation of the hook path (elevator and scissors), insertthe AC joint, after having palpated the hook path by using an elevator orthe hook under the acromion, dorsal of the AC joint. Determine the hookscissors. Select the correct hook depth (15 or 18mm). Take special care todepth (15 or 18mm), and insert the selected plate.avoid overcorrection. Use the plate holding <strong>for</strong>ceps to fix the plate tempo-Position the plate and use the plate holding <strong>for</strong>ceps to press it onto therarily to the clavicle. Control stability by pulling the arm, and verify themedial fragment. An improvement of the obtained reduction is possiblereduction (the acromion must be flush with the clavicle). Position the finalusing other bone holding <strong>for</strong>ceps. In very rare cases, it is possible to per-plate. Pull the acromioclavicular ligament and capsule under the lateralLiterature<strong>for</strong>m a temporary reduction with Kirschner wires.plate be<strong>for</strong>e pressing the plate onto the bone. Now press the plate ontothe bone. Repeat control of reduction and stability.Hackenbruch W., Regazzoni P. and Schwyzer K.Operative Behandlung der lateralen Claviculafraktur mit der ’’Clavicula-Hakenplatte’’ (Surgical treatment of a lateral clavicular fracture using the’’<strong>Clavicle</strong> <strong>Hook</strong> <strong>Plate</strong>“)Unfallchirurgie, Versicherungsmedizin 1994, vol. 87, no. 3:145Figura 2FixationFigura 5FixationHenkel Th., Oetiker R. and Hackenbruch W.Die Behandlung der frischen AC-Luxation Tossy III durch Bandnaht undtemporäre Fixation mit Clavicula-Hakenplatte (The treatment of the freshAC luxation, type Tossy III by ligament suture and temporary fixation usinga <strong>Clavicle</strong> <strong>Hook</strong> <strong>Plate</strong>)Swiss Surgery 1997, 3:160Depending on the type of fracture, use one or <strong>two</strong> screws to occupy thelateral plate holes, possibly 4.0mm cancellous bone screws. In case ofseveral fragments or a very small lateral fragment, these screws can beoptimally positioned obliquely through the LC-DCP holes. Place screwseccentrically in the medial plate holes to provide dynamic compression onthe fracture gap. As a rule, three screws are sufficient on the medial fragment.In a multifragmentary fracture, the longer eight hole plate may beused as an exception.Three cortex screws are usually enough to occupy the plate holes. Priorto the final tightening of the screws, either stitch and tie the retainingsutures to the ligament and capsule rest of the lateral clavicle or pull thesutures through the lateral holes of the plate and tie them together undertension. Proceed to the final tightening of the screws. Verify reductionand stability. Close the wound layer by layer over a drainage taking particularcare to exactly reconstruct the muscular fascia. Subsequent immobilization<strong>for</strong> <strong>two</strong> days. Thereafter, rehabilitation by early functionalexercises.Figura 3Figures 1-6: ventral-cranialFigura 6Figures 1-6: ventral-cranial