Medical Record and Authorization For Emergency Medical Care Form
Medical Record and Authorization For Emergency Medical Care Form
Medical Record and Authorization For Emergency Medical Care Form

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
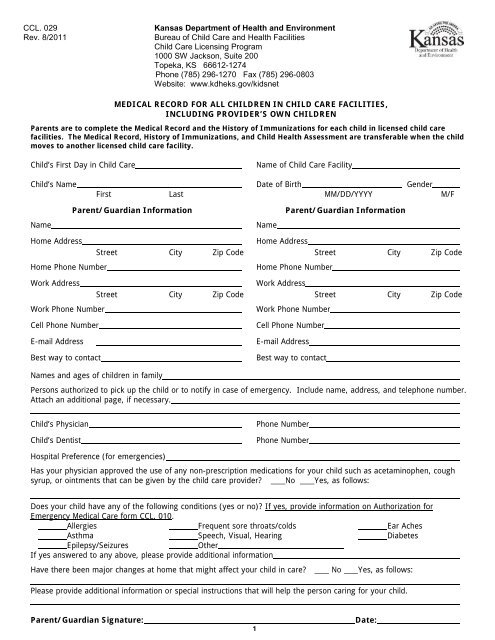
CCL. 029Rev. 8/2011Kansas Department of Health <strong>and</strong> EnvironmentBureau of Child <strong>Care</strong> <strong>and</strong> Health FacilitiesChild <strong>Care</strong> Licensing Program1000 SW Jackson, Suite 200Topeka, KS 66612-1274Phone (785) 296-1270 Fax (785) 296-0803Website: www.kdheks.gov/kidsnetMEDICAL RECORD FOR ALL CHILDREN IN CHILD CARE FACILITIES,INCLUDING PROVIDER’S OWN CHILDRENParents are to complete the <strong>Medical</strong> <strong>Record</strong> <strong>and</strong> the History of Immunizations for each child in licensed child carefacilities. The <strong>Medical</strong> <strong>Record</strong>, History of Immunizations, <strong>and</strong> Child Health Assessment are transferable when the childmoves to another licensed child care facility.Child’s First Day in Child <strong>Care</strong>Name of Child <strong>Care</strong> FacilityChild’s Name Date of Birth GenderFirst Last MM/DD/YYYY M/FNameParent/Guardian InformationNameParent/Guardian InformationHome AddressHome Phone NumberWork AddressWork Phone NumberHome AddressStreet City Zip Code Street City Zip CodeHome Phone NumberWork AddressStreet City Zip Code Street City Zip CodeWork Phone NumberCell Phone NumberE-mail AddressBest way to contactCell Phone NumberE-mail AddressBest way to contactNames <strong>and</strong> ages of children in familyPersons authorized to pick up the child or to notify in case of emergency. Include name, address, <strong>and</strong> telephone number.Attach an additional page, if necessary.Child’s PhysicianChild’s DentistPhone NumberPhone NumberHospital Preference (for emergencies)Has your physician approved the use of any non-prescription medications for your child such as acetaminophen, coughsyrup, or ointments that can be given by the child care provider? No Yes, as follows:Does your child have any of the following conditions (yes or no)? If yes, provide information on <strong>Authorization</strong> for<strong>Emergency</strong> <strong>Medical</strong> <strong>Care</strong> form CCL. 010.Allergies Frequent sore throats/colds Ear AchesAsthma Speech, Visual, Hearing DiabetesEpilepsy/SeizuresOtherIf yes answered to any above, please provide additional informationHave there been major changes at home that might affect your child in care? No Yes, as follows:Please provide additional information or special instructions that will help the person caring for your child.Parent/Guardian Signature:_________________________________________Date:_____________1
CCL 010Rev. 7/2012Kansas Department of Health <strong>and</strong> EnvironmentBureau of Family Health1000 SW Jackson, Suite 200 * Topeka, KS 66612-1274Child <strong>Care</strong> Unit Phone: 785-296-1270 Fax: 785-296-0803Foster <strong>Care</strong> Unit Phone (785) 296-1270 Fax (785) 296-7025Website: www.kdheks.gov/kidsnet/Consult local hospital to be sure this form is acceptable. Written permission of the parent, guardian or legal custodian , foremergency medical treatment must be on file at facility for each child on a form that meets the requirements of the hospital orclinic where emergency care will be given.License or Certificate #___________________89In order to meet all legal requirements, I hereby authorize _________________________________________________________ <strong>and</strong>/or__________________________________who is (are) representative(s) of ______________________________________________________(Child <strong>Care</strong> Facility)to give consent for any <strong>and</strong> all necessary emergency medical care for my child _________________________________________________(Name)while said child is in said individual's custody between the dates of ________________________ <strong>and</strong> ____________________________Month Day Year Month Day Year________________________________________________________________(Signature of Parent or Guardian)Parent's signature needs notarization or witnessed if required by local hospital or clinic.________________________________________________________________(Witness)Hiersteiner Child Development Center staffHiersteiner Child Development Centeruntil further noticeState of KansasBefore me, the undersigned authority, on this day personally appeared _____________________________________________known to be the person whose name is subscribed above, <strong>and</strong> acknowledged to me that he/she executed the same for the purposetherein expressed.Sworn <strong>and</strong> subscribed before me this ________________________ day of ____________________________Year________.(SEAL) Notary Public__________________________________________.My Commission expires _________________________________.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Physician _____________________________ Address __________________________________ Phone ______________________Hospital Preference ____________________________________________________________________________________________<strong>Emergency</strong> Phone Numbers ______________________________________________________________________________________Home Father (work) Mother (work)Do you have Health Insurance? _______ Policy Name <strong>and</strong> Number ______________________________________________________Do you receive medical assistance? _______ Program <strong>and</strong> <strong>Care</strong> Number _________________________________________________Is child eligible for military medical care? _______ I.D. Number _________________________________________________________<strong>Medical</strong> Information on Child: (see attached information)(Attach this form to the child's health record. Both forms must be taken to the emergency room.)
History of ImmunizationsRequired for all children in child care facilities, including the provider’s own children. A Kansas Certificate ofImmunizations (KCI) may be substituted for this form <strong>and</strong> attached to the completed <strong>Medical</strong> <strong>Record</strong>.Child’s Name:Date of Birth:First Last MM/DD/YYYYSection I. <strong>For</strong> a recommended schedule of immunizations, refer to the current schedule published by theAdvisory Committee on Immunization Practices (ACIP).Vaccine<strong>Record</strong> the Month. Day <strong>and</strong> Year that each Dose of Vaccine was Received1 st 2 nd 3 rd 4 th 5 th 6 thDTaP/DT/Td/Tdap (Diphtheria,Tetanus, Pertussis)PolioMMR (Measles, Mumps, <strong>and</strong> Rubellacombined)HBV (Hepatitis B Vaccine)Varicella (Chicken Pox)HIB (Hemophilus Influenzae Type B)PCV7 (Pneumococcal Conjugate)HEP A (Hepatitis A)Rotavirus **Recommended 6 mo of age; not requiredHx of Disease:Physician SignatureDate of Illness:Section II.Complete this section only if your child is exempted from the law requiring immunizations [K.S.A. 65-508(d)].Section The following II. Complete two options Section are the below ONLY only exemptions if your child allowed is exempted by law. Please from check laws requiring either (A) requiring or (B) below <strong>and</strong>immunizations complete as required: [ K.S.A. 65-508(d) <strong>and</strong> K.S.A. 65-519(c) ] (A) Certification from licensed physician stating that immunization would endanger child’s life:Exempt from following immunizations:HibDTP Pertussis Only ____Tetanus ____Polio MMR Rubella Only Hep A Hep B_PCV7 ____OtherPhysician’s Signature (required): ________________________________________________Date:_______________ (B) My child is exempt under the law from immunizations. As the Parent or Legal Guardian, I statethat I am an adherent of a religious denomination whose teachings are opposed to immunizations.Section III.Parent/Guardian Signature:_________________________________________Date:________________2
CCL. 029aRev. 08/2011Child Health AssessmentThe Child Health Assessment form is to be completed <strong>and</strong> signed by a nurse approved by KDHE to perform Child HealthAssessments or a Licensed Physician. If a Physician Assistant (PA) completes the Child Health Assessment, the signatureof the Licensed Physician authorizing the PA is to be included at the bottom of this form.A Child Health Assessment, recorded on a KDHE <strong>For</strong>m or other acceptable <strong>For</strong>ms mentioned below, is required for allchildren including children of the provider or staff in Licensed Day <strong>Care</strong> Homes, Group Day <strong>Care</strong> Homes, Child <strong>Care</strong>Centers <strong>and</strong> Preschools. A Kan-Be-Healthy Assessment <strong>For</strong>m is a KDHE <strong>For</strong>m <strong>and</strong> is acceptable, a Physician HealthAssessment <strong>For</strong>m is acceptable, <strong>and</strong> a School Health Assessment <strong>For</strong>m is acceptable for school-age children or youth.The Health Assessment <strong>For</strong>m used should be attached to the KDHE <strong>Medical</strong> <strong>Record</strong> <strong>For</strong>m (CCL. 029).Child’s Name_________________________________________FirstLastDate of Birth___________________Health history <strong>and</strong> medical information pertinent to routine child care <strong>and</strong> emergencies(describe, if any): NoneAllergies to food or medicine (describe, if any): NoneList current medications (if any): NoneDo you see this child for regularhealth supervision: Yes NoLength/Height: ______IN/CM %ILE_______ Weight: _____LB/KB %ILE_______Physical Examination If Normal If Abnormal - CommentsHead/Ears/Eyes/Nose/ThroatTeethCardio/RespiratoryAbdomen/GIGenitalia/BreastsExtremities/Joints/Back/ChestSkin/Lymph NodesNeurologic & DevelopmentalScreening Tests Screening Date Note Here if Results are Pending or AbnormalLeadAnemia (HGB/HCT)Urinalysis (UA)HearingVisionHealth Problems or Special Needs, Recommended Treatment/Medications/Special <strong>Care</strong> (Attach additional sheets if necessary) NoneSignature of Licensed Physician or Nurse approved for Child Health AssessmentsDatePrint the Name of the Individual Signing AbovePhone NumberAddress City Zip Code3