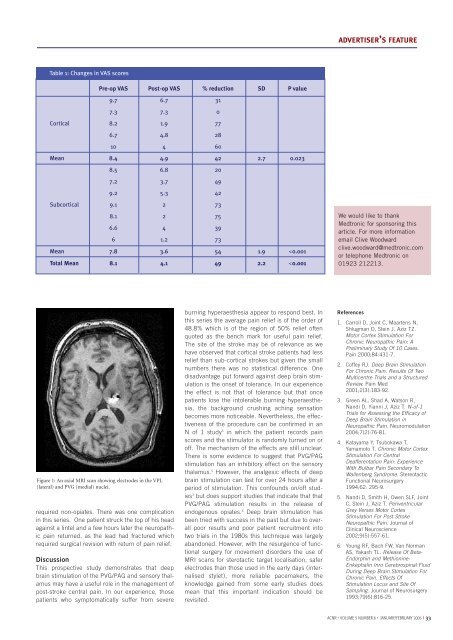
ADVERTISER’S FEATUREDeep bra<strong>in</strong> stimulation for the alleviation of poststroke neuropathic pa<strong>in</strong>IntroductionIntractable neuropathic pa<strong>in</strong> affects 2-8% of patients after a stroke. 1 Typically, a burn<strong>in</strong>g hyperaesthesia <strong>and</strong> ach<strong>in</strong>g affect areas thatare rendered numb after a stroke. Such pa<strong>in</strong> usually resists medical therapy leav<strong>in</strong>g these patients with no symptom alleviation. Inthe UK, an estimated 28,000 people will suffer from this predicament.Although motor cortex stimulation has been reported as a mode of therapy for this condition the published literature quotesextremely variable results. 2,3 Therefore, deep bra<strong>in</strong> stimulation has been the preferred mode of therapy for neuropathic pa<strong>in</strong> atOxford s<strong>in</strong>ce 1999. Dur<strong>in</strong>g this period, 15 post stroke patients with neuropathic pa<strong>in</strong> were treated with deep bra<strong>in</strong> stimulation. Herewe present the cl<strong>in</strong>ical results.Tipu AzizProfessor Tipu Z Aziz is aConsultant Neurosurgeon at theRadcliffe Infirmary, Oxford <strong>and</strong>Char<strong>in</strong>g Cross Hospital London.He is an expert <strong>in</strong> functional neurosurgery<strong>and</strong> has a special<strong>in</strong>terest <strong>in</strong> the surgical treatmentof movement disorders.Sarah LF OwenMiss Sarah Owen qualified as anOperat<strong>in</strong>g Department Practitionerfrom Selly Oak, Birm<strong>in</strong>gham <strong>in</strong>1988, <strong>and</strong> later ga<strong>in</strong>ed her firstneurosurgical position at theRadcliffe Infirmary <strong>in</strong> 1989. Shesubsequently read for a BA (hons)<strong>in</strong> Anthropology with a special<strong>in</strong>terest <strong>in</strong> the evolution of the primatebra<strong>in</strong> at Oxford BrookesUniversity, where she qualified <strong>in</strong>2004. She is currently read<strong>in</strong>g fora DPhil at Brasenose College,University of Oxford. Her research<strong>in</strong>volves <strong>in</strong>vestigat<strong>in</strong>g the sensorypathways <strong>in</strong>volved <strong>in</strong> pa<strong>in</strong>.Correspondence to:Professor TZ AzizDepartment of Neurosurgery,Radcliffe Infirmary,Woodstock Road,Oxford, OX2 6HE.Tel: 01865 228425,Email: tipu.aziz@physiol.ox.ac.uk32 I <strong>ACNR</strong> • VOLUME 5 NUMBER 6 • JANUARY/FEBRUARY 2006Patient population <strong>and</strong> surgeryOf the 15 patients <strong>in</strong> the study the average agewas 58.6 years, there were 3 female <strong>and</strong> 12 malepatients, 5 had cortical <strong>and</strong> 10 subcortical strokesof which 8 were thalamic, 1 pont<strong>in</strong>e, <strong>and</strong> 1 <strong>in</strong> the<strong>in</strong>ternal capsule. Average duration of pa<strong>in</strong> prior tosurgery was 5.2 years. The most disabl<strong>in</strong>g aspectof the pa<strong>in</strong> syndrome was a burn<strong>in</strong>g hyperaesthesia<strong>in</strong> the area of numbness that affected 7 of the15 patients. Also described was a severe cramp<strong>in</strong>gor crush<strong>in</strong>g sensation.Provided there were no over rid<strong>in</strong>g medical orpsychological contra<strong>in</strong>dications, deep bra<strong>in</strong> stimulationof the periventricular area <strong>and</strong> sensorythalamus were offered to these patients. Both targetswere chosen after exist<strong>in</strong>g literature by differentauthors quoted both as be<strong>in</strong>g effective. 4 Alsothere was no <strong>in</strong>dication of any superiority of onetarget over another. Preoperatively they filled <strong>in</strong>pa<strong>in</strong> charts us<strong>in</strong>g a visual analogue scale <strong>and</strong> theMcGill questionnaire. They also underwent a comprehensiveneuropsychological assessment. Deepbra<strong>in</strong> stimulation for neuropathic pa<strong>in</strong> hasapproval of the local ethics committee.All patients had a T-1 weighted axial MRI scanprior to surgery, <strong>and</strong> a CRW base r<strong>in</strong>g was appliedto the patients’ head under local anaesthesia. Astereotactic CT scan was then performed <strong>and</strong>us<strong>in</strong>g the Radionics Image Fusion‚ <strong>and</strong>Stereoplan‚ programme the MRI scan is volumetricallyfused to the sterotactic CT scan. This is atechnique that has been adopted s<strong>in</strong>ce 1995 toelim<strong>in</strong>ate the errors of us<strong>in</strong>g MRI sterotaxy alonethat arise from the spatial distortions <strong>in</strong>tr<strong>in</strong>sic tomagnetic fields. The co-ord<strong>in</strong>ates for the PVG <strong>and</strong>VPL were then calculated. Patients with strokes <strong>in</strong>the sensory thalamus were only implanted <strong>in</strong> thePVG/PAG with a Medtronic 3387. The VPL wasimplanted with a Medtronic 3387 electrode wherestimulation <strong>in</strong>duced parasthesia <strong>in</strong> the area ofpa<strong>in</strong> <strong>and</strong> the PVG/PAG with a Medtronic 3387electrode where stimulation <strong>in</strong>duced relief of pa<strong>in</strong>or a sensation of warmth <strong>in</strong> the area of pa<strong>in</strong>. Thedeepest electrode was noted to be <strong>in</strong> a satisfactoryposition if eye bobb<strong>in</strong>g was <strong>in</strong>duced at an <strong>in</strong>tensityof stimulation at least twice that required forsensory effects. The electrodes were fixed to theskull with a m<strong>in</strong>iplate prior to externalisation.In all patients the electrodes were externalisedfor a week of trial stimulation. Pa<strong>in</strong> was assessedbefore surgery <strong>and</strong> dur<strong>in</strong>g stimulation by a selfratedvisual analogue scale. Post stroke pa<strong>in</strong> dur<strong>in</strong>gthe trial period responded better to stimulationof the PVG compared to the VPL. If the patientswere satisfied with the degree of pa<strong>in</strong> relief, fullimplantation of a Medtronic pulse generator wasperformed <strong>in</strong> the follow<strong>in</strong>g week under generalanaesthesia.ResultsDur<strong>in</strong>g a trial period of one week follow<strong>in</strong>g surgery,3 patients did not feel there was significant pa<strong>in</strong>relief to proceed to full implantation of the pacemaker<strong>and</strong> the electrodes were removed underlocal anaesthesia. The 12 rema<strong>in</strong><strong>in</strong>g underwentfull implantation of the extension cables <strong>and</strong> thepacemaker (SYNERGY, Medtronic Inc). Althoughdual channel, all patients were implanted with aSYNERGY because of the longer battery life, if onechannel is used a plug is used to close off the<strong>in</strong>active channel. The patients were then revieweda month later to optimise the sett<strong>in</strong>gs for maximumpa<strong>in</strong> relief <strong>and</strong> were reviewed 6 monthlythereafter.Follow upAverage follow up was 15 months. N<strong>in</strong>e patientspreferred chronic stimulation of the PVG, one <strong>in</strong>the VPL <strong>and</strong> three preferred both electrodes to beactivated. The results are summarised <strong>in</strong> Table 1.Overall the reduction <strong>in</strong> pa<strong>in</strong> scores was 48.8%(SD 2.2, p
ADVERTISER’S FEATURETable 1: Changes <strong>in</strong> VAS scoresPre-op VAS Post-op VAS % reduction SD P value9.7 6.7 317.3 7.3 0Cortical 8.2 1.9 776.7 4.8 2810 4 60Mean 8.4 4.9 42 2.7 0.0238.5 6.8 207.2 3.7 499.2 5.3 42Subcortical 9.1 2 738.1 2 756.6 4 396 1.2 73Mean 7.8 3.6 54 1.9