information manual - for liver transplant recipients and their families
information manual - for liver transplant recipients and their families
information manual - for liver transplant recipients and their families
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
INFORMATION MANUALFOR LIVER TRANSPLANTRECIPIENTS ANDTHEIR FAMILIESJune 2012AUSTRALIAN NATIONAL LIVERTRANSPLANTATION UNIT
THE LIVER TRANSPLANT UNITCONTENTSIntroduction...................................................................................................................................... 3Section 1. How the <strong>liver</strong> works 4Section 2. Assessment 6Section 3. Nutrition in <strong>liver</strong> <strong>transplant</strong>ation 9Section 4. In<strong>for</strong>mation you might need 10Section 5. Waiting <strong>for</strong> the <strong>transplant</strong> 12Section 6. The right donor <strong>for</strong> you 13Section 7. Preparation <strong>for</strong> surgery 15Section 8. The <strong>transplant</strong> itself 16Section 9. After surgery 18Section 10. The immune system 19Section 11. Infection 20Section 12. Rejection 21Section 13. Nutrition following <strong>liver</strong> <strong>transplant</strong>ation 22Section 14. Recurrence of original disease 25Section 15. Drugs used in <strong>transplant</strong>ation 26Section 16. Patient <strong>in<strong>for</strong>mation</strong> about drug trials 30Section 17. Other post-<strong>transplant</strong> problems 31Section 18. Outpatient visits 33Section 19. Follow-up medical care 34Section 20. Travel 35Section 21. Vaccinations 36Section 22. After discharge 37Section 23. Common Tests Per<strong>for</strong>med 41Appendix A: Glossary 43Appendix B: Copy of Consent Form 48Appendix C: Contact numbers 49Appendix D: Liver Support Group Application Form 50Appendix E: The RPA Transplant Institute 52Professional Websites 53Notes 541INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUAL2
THE LIVER TRANSPLANT UNITINTRODUCTIONThis booklet has been designed to give you the <strong>in<strong>for</strong>mation</strong> you <strong>and</strong> your family need to help youunderst<strong>and</strong> what is involved in <strong>liver</strong> <strong>transplant</strong>ation. Various members of the Transplant Team willdiscuss this <strong>in<strong>for</strong>mation</strong> with you. You are encouraged to ask questions or talk about any anxietiesconcerning any of this <strong>in<strong>for</strong>mation</strong>. Our aim is to in<strong>for</strong>m you about <strong>liver</strong> <strong>transplant</strong>ation, so that you canmake decisions about your treatment based on a good knowledge of the procedures, benefits <strong>and</strong> risksof <strong>liver</strong> <strong>transplant</strong>ation.The Liver Transplant Unit at Royal Prince Alfred Hospital was opened in 1986. Since then the Unit hasper<strong>for</strong>med more than 1000 <strong>liver</strong> <strong>transplant</strong>s.The general goals of <strong>liver</strong> <strong>transplant</strong>ation are to prolong life <strong>and</strong> improve the quality of life whileoptimising the use of available <strong>liver</strong> donors. The <strong>liver</strong> <strong>transplant</strong> process continues to evolve <strong>and</strong>improve, demonstrating excellent survival rates, now over 90% one year patient survival rates.Most diseases that end with <strong>liver</strong> failure have been successfully treated by <strong>liver</strong> <strong>transplant</strong>ation. Themost common indications <strong>for</strong> <strong>liver</strong> <strong>transplant</strong>ation in adults are chronic hepatitis C, hepatitis B, primary<strong>liver</strong> cancer (also known as hepatocellular carcinoma), primary biliary cirrhosis, primary sclerosingcholangitis, autoimmune <strong>liver</strong> disease <strong>and</strong> alcoholic <strong>liver</strong> disease. Other indications include metabolic<strong>liver</strong> diseases including haemochromatosis <strong>and</strong> Wilson’s disease, acute <strong>liver</strong> failure <strong>and</strong> massive <strong>liver</strong>enlargement due to a variety of causesLiver <strong>transplant</strong>ation is usually recommended when there is a progressive deterioration in <strong>liver</strong> function.Liver failure is manifested by a number of physical <strong>and</strong> clinical symptoms (eg: ascites (abdominalswelling due to fluid accumulation), variceal bleeding (bleeding from large veins in the oesophagus),hepatic encephalopathy (confusion <strong>and</strong> vagueness), or malnutrition) <strong>and</strong> by changes in blood resultsthat suggest deteriorating <strong>liver</strong> function (eg: low albumin, rising bilirubin <strong>and</strong> blood clottingabnormalities).3INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 1:HOW THE LIVER WORKSLiver functionsThe <strong>liver</strong> is the largest <strong>and</strong> one of the mostcomplex organs in the body. It has manyfunctions; some of the most important include:• as a biochemical factory, it processesnutrients absorbed from the gut, <strong>and</strong> makesthem available <strong>for</strong> use by other parts of thebody• the production of bile <strong>and</strong> its excretion intothe intestine is important <strong>for</strong> absorption offats <strong>and</strong> certain vitamins• the production of blood factors includingmany of those necessary <strong>for</strong> blood clotting,<strong>and</strong> <strong>for</strong> normal body fluid balance• the removal of toxins from the bloodincluding those produced by bacteria in thegut <strong>and</strong> <strong>for</strong> the breakdown of alcohol <strong>and</strong>many drugs• the removal of germs in the blood absorbedfrom the gut• the processing of some hormones <strong>and</strong>vitaminsLiver diseaseUnless <strong>liver</strong> damage is fairly severe or advanced,diseases of the <strong>liver</strong> are often “silent” <strong>and</strong>patients may be unaware of any problem.The signs <strong>and</strong> symptoms of <strong>liver</strong> disease can beexplained by considering the various <strong>liver</strong>functions. Different <strong>liver</strong> diseases may affectsome functions more than others, resulting invariability between patients.The impairment of processing of nutrientsresults in wasting of tissues, particularly muscle.Impairment of the <strong>liver</strong>’s ability to excrete bilecauses accumulation of its constituentsincluding bilirubin pigment, responsible <strong>for</strong> theyellow discolouration of skin <strong>and</strong> urine4(jaundice), <strong>and</strong> bile acids which may beresponsible <strong>for</strong> the chronic itch suffered bysome patients.The decreased absorption of vitamin K <strong>and</strong>inadequate production of blood clotting factorscauses easy bruising <strong>and</strong> bleeding, initially fromthe gums.Massive bleeding from the gut is due, in part, toblood from the gut being diverted away from itsusual course through the <strong>liver</strong>, to other channelsin the oesophagus (gullet), which may ruptureunder pressure.The decreased production of blood proteinsinvolved in body fluid balance <strong>and</strong> the scarringof the <strong>liver</strong> contribute to the accumulation offluid in the abdomen <strong>and</strong> legs.The failure of the <strong>liver</strong> to deal adequately withpoisons produced in the gut can causedrowsiness, <strong>for</strong>getfulness, <strong>and</strong> lack ofconcentration, confusion <strong>and</strong> coma.A damaged <strong>liver</strong> is also much slower at dealingwith alcohol <strong>and</strong> drugs causing increasingsensitivity to <strong>their</strong> use.Inadequate removal of micro-organisms or“germs” from the blood coming from the gutpartly explains the increased incidence ofserious infections in patients with <strong>liver</strong> disease.Signs <strong>and</strong> symptoms of cirrhosisAs continued scarring <strong>and</strong> damage to the <strong>liver</strong>occur, the following signs <strong>and</strong> symptoms mayappear:• Loss of appetite• Weight loss• Jaundice - yellow discoloration of the whitesof the eyes <strong>and</strong> skin occurs because bilepigment can no longer be removed from the<strong>liver</strong>• Itching – due to the retention of bileproducts in the skin• Ascites – abdominal swelling due to anaccumulation of fluid caused by theobstruction of blood flow through the <strong>liver</strong>• Vomiting of blood – frequently occurs fromswollen ruptured varices (veins that burst) inthe lower end of the oesophagus due to the
THE LIVER TRANSPLANT UNITincreased pressure in these vessels causedby scar tissue <strong>for</strong>mation• Encephalopathy (impending coma) – subtlemental changes ranging from poorconcentration advancing to profoundconfusion <strong>and</strong> coma.Treatment <strong>for</strong> these conditions• Ascites is treated by reducing the intake ofsalt <strong>and</strong> the administration of medications toimprove excretion of salt <strong>and</strong> water by thekidneys (fluid tablets or diuretics). Somepeople are unable to take fluid tabletsbecause of side-effects. In some instances,large amounts of fluid are removed by directcatheter drainage through the abdominalwall (a ‘tap’).• Treatment of encephalopathy includes useof specific medication such as lactulosesyrup.• Treatment of bleeding from varices (internalvaricose veins) includes taking medicationto reduce the likelihood of bleeding orrebleeding, ‘b<strong>and</strong>ing’ (the placement ofrubber b<strong>and</strong>s on the varices at the time ofendoscopy), <strong>and</strong> occasionally, a radiologicalprocedure called transjugular intrahepaticportosystemic shunt (TIPSS).Management of encephalopathyWhen this condition develops at home it can bedistressing to deal with, so if you have noticedany worrying mental changes in your familymember or friend, please feel free to discuss itwith a member of the <strong>transplant</strong> team. We cangive you strategies to help prevent it or manageit, if it occurs.5INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 2: ASSESSMENTReferral <strong>for</strong> TransplantIdeally, patients with cirrhosis should be referredto the <strong>liver</strong> <strong>transplant</strong> unit when they developevidence of deteriorating <strong>liver</strong> function,experience <strong>their</strong> first major complication e.g.ascites, variceal bleeding, spontaneous bacterialperitonitis (an infection that can develop in theabdominal fluid), encephalopathy ormalnutrition.Patients with hepatocellular cancer (primary <strong>liver</strong>cancer) <strong>and</strong> cirrhosis should be referred <strong>for</strong>assessment by the <strong>liver</strong> <strong>transplant</strong> team as soonas the tumour is discovered, so that optimaltreatment can be decided.Transplant AssessmentA detailed assessment is carried out prior todeciding whether a patient is a c<strong>and</strong>idate <strong>for</strong><strong>liver</strong> <strong>transplant</strong>ation.As a general rule there are four basicrequirements, which would indicate that youmay be considered suitable <strong>for</strong> assessment:a. irreversible, progressive <strong>liver</strong> diseaseb. the <strong>liver</strong> disease fails to respond to all other<strong>for</strong>ms of medical <strong>and</strong> surgical treatmentc. absence of other major diseasesd. ability to underst<strong>and</strong> the nature <strong>and</strong> risks of<strong>liver</strong> <strong>transplant</strong>ationThe assessment processThere are a number of tests that will need to beper<strong>for</strong>med while you are undergoing assessment<strong>for</strong> <strong>transplant</strong>ation. The results of these testsprovide an overall assessment of your currentstate of health <strong>and</strong> help determine if<strong>transplant</strong>ation is the right option <strong>for</strong> you. Thereare a number of baseline tests that all patientsneed to undergo; extra tests are tailored to theindividual situation.In most people, these tests are per<strong>for</strong>med on anoutpatient basis.Time:usually 2 - 3 weeks needed to completetests.6The assessment period may vary greatlydepending on the availability of test procedures,personnel <strong>and</strong>, in particular, the complexity ofthe individual case.An outline of the tests you will need toundergoBlood testsA number of tests including:• Biochemistry• Haematology• Blood clotting profile• Cross-matching• Tissue typing• Hormone levels• Hepatitis screening• Screening <strong>for</strong> exposure to certain viruses,which will help to optimise your post<strong>transplant</strong> management• A 24-hour urine collection to assess kidneyfunctionOther tests include:• Chest X-ray, hip X-ray, spine X-ray• ECG <strong>and</strong> cardiac ECHO• Lung function tests• Abdominal CT scan (This computerisedimage will show the size <strong>and</strong> shape of the<strong>liver</strong> <strong>and</strong> major blood vessels. At times, thistest reveals previously unsuspected <strong>liver</strong>tumour.)• Bone density scan• Endoscopy• Female patients must have a Mammogram<strong>and</strong> Pap smear• Dental checkOther tests as individually indicatedTissue typingAlthough we per<strong>for</strong>m tissue typing on all patientsawaiting <strong>transplant</strong>ation, we do not matchdonors on the basis of tissue type. There arethree reasons:1. It does not seem to make any difference tothe outcome.2. There is usually insufficient time toaccurately tissue type a donor.3. There is a shortage of donors, so we wouldnever do any <strong>liver</strong> <strong>transplant</strong>s if we had towait to have a tissue-type match.
THE LIVER TRANSPLANT UNITSECTION 3: NUTRITION IN LIVERTRANSPLANTATIONAdequate nutrition is a very important aspect of<strong>liver</strong> <strong>transplant</strong>ation. Your nutritionalrequirements will change over a relatively shortperiod of time depending upon where you are inthe <strong>transplant</strong>ation process i.e. be<strong>for</strong>e the <strong>liver</strong><strong>transplant</strong>, in hospital after the <strong>transplant</strong> ormonths to years after the <strong>transplant</strong>.Your diet whilst you are awaiting your<strong>transplant</strong>Many patients with severe <strong>liver</strong> disease have losta significant amount of <strong>their</strong> body fat stores <strong>and</strong>body protein stores by the time they are referredto the <strong>liver</strong> <strong>transplant</strong> unit. The most importantnutritional goal whilst waiting <strong>for</strong> your <strong>transplant</strong>is to eat enough food to stop your body losingmore fat <strong>and</strong> more protein. This may be difficultif your appetite is poor. You will really need towork very hard at eating <strong>and</strong> this job does notend until some months after the <strong>transplant</strong>. Ifyou have been advised to restrict some foods,you will need to be more careful of the sorts offood that you eat but it is still important that youwork very hard to keep up a high energy/highprotein intake.The diet you were following when you first metthe <strong>transplant</strong> team may be changed whilst youare waiting <strong>for</strong> <strong>transplant</strong>ation. The dietitian <strong>and</strong>the doctors will discuss your individualrequirements with you.The most common restriction <strong>for</strong> people waiting<strong>for</strong> a <strong>liver</strong> <strong>transplant</strong> is a salt (sodium) restriction.If you have been advised to reduce your saltintake you will need to discuss this with one ofthe dietitians as salt occurs in many foods, bothprocessed <strong>and</strong> naturally occurring. You will needsome professional advice about reducing yoursalt intake at the same time as maintaining ahigh energy/high protein intake. If you continueto eat foods with a high salt content it will bemore difficult to control the fluid in yourabdomen <strong>and</strong> legs.Most people waiting <strong>for</strong> a <strong>liver</strong> <strong>transplant</strong> havean increased need <strong>for</strong> protein <strong>and</strong> energy. If you9cannot eat enough to meet your body’sincreased energy <strong>and</strong> protein requirements youwill be asked to use dietary supplements suchas Ensure, Fortisip, Resource Protein, Polyjouleor Hepatamine or any combination of these.The Social Worker’s Role in the LiverTransplantation UnitThe Social Worker on the team is available towork together with you <strong>and</strong> your family, to assistyou with the ongoing process of <strong>liver</strong><strong>transplant</strong>ation <strong>and</strong> to support you in thedecisions you need to make.Some of the ways the Social Worker can assistare:*helping with the adjustment to living with anillness <strong>and</strong> negotiating the <strong>transplant</strong>process*relationship <strong>and</strong> family concerns*advising individuals of <strong>their</strong> rightsPeople can require added assistance withpractical concerns such as:*hospital procedures <strong>and</strong> documentation*financial concerns, such as Centrelinkoptions*accommodation – in or near the hospital*travel issues eg IPTAAS (Isolated Patients’Travel <strong>and</strong> Accommodation AssistanceScheme)*provide education resources eg books, webpages about <strong>liver</strong> <strong>transplant</strong>ation*lifestyle options such as recreation activities*organise interpreters <strong>and</strong> liaise with culturalcommunity services*discharge planning eg community supportreferralsThe social work service is free <strong>and</strong> confidential<strong>and</strong> available to all patients, <strong>their</strong> <strong>families</strong> <strong>and</strong>carers.You can contact a Social Worker through theSocial Work Department telephone 9515 3787or ask the staff of the <strong>liver</strong> <strong>transplant</strong> team tocontact a social worker by page.INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 4: INFORMATION YOUMIGHT NEEDAccommodationThe hospital does not provide patient/relativeaccommodation on site. There isaccommodation available at a hostel in Ashfieldwhich is about 15 minutes drive from thehospital. The hostel consists of 26 rooms, someof which contain one single bed <strong>and</strong> four roomshave two single beds. The cost ofaccommodation is $65 double <strong>and</strong> $45 persingle per night.Accommodation bookings <strong>for</strong> the hostelcan be made by contacting the RPAAccommodation Coordinator, Noeleen Frankson (02) 9515 9901. She will be able to adviseyou regarding other accommodation options inthe area. After hours phone NursingAdministration on (02) 9515 6111 to assist withorganising emergency accommodation.Ambulance fundIt is ABSOLUTELY VITAL that you have or getambulance cover while you are on the waitinglist. If you are on a Social Security Pension orBenefit you are already covered. You can checkthis with the Department of Social Security. Ifyou have private health insurance, you areprobably covered. You should check with yourinsurance company. If you have neither, youshould obtain ambulance cover from a privatehealth insurance company (eg: NIB orMedibank Private).Travel <strong>and</strong> accommodation expensesYou are responsible <strong>for</strong> your own travel <strong>and</strong>accommodation expenses. However, if you livemore than 100 kilometres away from thehospital, you may be entitled to a refund of partof your travel <strong>and</strong> accommodation expenseswhen you come to the hospital to see a doctor.IPTAAS (Isolated Patients Transport <strong>and</strong>Accommodation Assistance Scheme)IPTAAS provides reimbursement <strong>for</strong> travel <strong>and</strong>accommodation costs to people who need totravel more than 100 kilometres one way from<strong>their</strong> home to obtain specialist medical10treatment. IPTAAS <strong>for</strong>ms can be obtained viayour local doctor or the links below:NSW:www.health.nsw.gov.au/living/transport/pdf/terms.pdfACT:www.health.act.gov.au/iptas (ACT patients tocomplete prior to <strong>transplant</strong>).Income issuesIf you are still working, you may need to plannow <strong>for</strong> the time when you are not workingbecause of deteriorating health or while you arerecovering from your <strong>transplant</strong>. You may beentitled to a Department of Social SecurityBenefit or Pension, especially if you have noother income. Your carer may be entitled to aCarers Pension. Please see the Social Worker ifyou have any questions about this.Hospital chargesPatients' costs <strong>for</strong> Liver Transplant1. Do I have to pay <strong>for</strong> the <strong>liver</strong> <strong>transplant</strong>ation?The Australian National Transplant Unit isfunded by the New South Wales StateGovernment. All your patient costs in hospital <strong>for</strong>the <strong>transplant</strong> admission are covered by thisfunding. You should not receive any billassociated with your <strong>liver</strong> <strong>transplant</strong> procedure.This applies to your hospital admissions <strong>for</strong> the<strong>transplant</strong> procedure. Once you are discharged,you will require ongoing drug prescriptions viathe hospital Pharmacy. The Pharmacy willcharge you the st<strong>and</strong>ard nominal chargeassociated with hospital prescriptions <strong>for</strong> anoutpatient. If you require further hospitalisationafter your <strong>transplant</strong> <strong>for</strong> whatever reason, youhave the right to nominate your insurancecategory as you think most appropriate.The InternetYou may find <strong>in<strong>for</strong>mation</strong> about <strong>liver</strong><strong>transplant</strong>ation on the Internet. This <strong>in<strong>for</strong>mation</strong>may be of interest you. However, you shouldremember that most of it applies to the UnitedStates, Canada or Europe. The <strong>in<strong>for</strong>mation</strong>included may not apply to Australia or theAustralian National Liver Transplantation Unit inSydney. Please check with your doctors aboutany questions you have about material you havefound on the Internet.
THE LIVER TRANSPLANT UNITYou may be interested in looking up thefollowing sites <strong>for</strong> <strong>in<strong>for</strong>mation</strong>:1. http://www.cs.nsw.gov.au/gastro/<strong>liver</strong><strong>transplant</strong>2. http://www.gesa.org.au3. www.<strong>transplant</strong>.org.au4. www.myDr.com.au5. http://www.hepatitisaustralia.com6. http://www.hepatitisc.org.au7. http://www.<strong>liver</strong>foundation.org8. http://www.health.nsw.gov.au9. http://www.trioweb.orgINFORMATION MANUAL11
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 5: WAITING FOR THETRANSPLANTTo those people who have been told to prepare<strong>for</strong> placement on the Waiting List.(If you are unsure then you have not been told).(1) Have a mobile phone(2) Install “call waiting” on your home phone.(3) Make sure you have ambulance cover.(4) Let the Transplant Team know as soon aspossible <strong>for</strong> any changes in yourcircumstances.(5) Do not hesitate to contact us regarding anyissues that are of concern to you.(6) Become thoroughly familiar with this book.(7) It is strongly advised that you have all youraffairs in order prior to being actively listed<strong>for</strong> <strong>transplant</strong>. This includes making a will<strong>and</strong> organising power of attorney.(8) It will be very much to your advantage if youcan arrange <strong>for</strong> your GP to be involved inyour ongoing care after the <strong>transplant</strong>.Please discuss this with them.(9) Await further instructions.Meeting with Transplant CoordinatorIf you are considered as suitable <strong>for</strong> immediate“Listing” <strong>for</strong> Transplant, the TransplantCoordinator will contact you to arrange anappointment.At this appointment:• Details of the surgery will be discussed withyou.• Discussion will take place of what to dowhen the call comes.• The Coordinator will confirm your contactdetails with you, this will include all relevanttelephone numbers including a mobiletelephone number (you will need to becontactable at all times)• The Transplant Coordinator can becontacted on:Claire BakerMon-Fri 7.00am - 3.30pmTel: 9515 7274After hours:Switchboard 9515 6111 <strong>and</strong> ask to speak tothe Transplant Coordinator on-call12Once you have been accepted on the waitinglist, the final decision to have a <strong>transplant</strong> is stillup to you. Be ready <strong>and</strong> available <strong>for</strong> a<strong>transplant</strong> call at all times, unless otherwisediscussed with medical staff <strong>and</strong> the TransplantCoordinator.You will need to be contactable 24 hours a day,7 days a week. The Liver Transplant Coordinatorwill discuss this with you. They also discusstravel <strong>and</strong> accommodation arrangements withyou. Waiting time can vary from one day to manymonths, possibly years. There can be muchanxiety <strong>and</strong> stress whilst you wait <strong>for</strong> a suitableorgan.Whilst waiting <strong>for</strong> <strong>transplant</strong>, you will return tothe clinic <strong>for</strong> regular follow up, usually on amonthly basis. You need to notify us if youbecome unwell or if you are admitted to hospital<strong>for</strong> any reason.WHAT TO DO IF YOU BECOME UNWELLAT HOME OR HAVE ANY CONCERNSRELATED TO YOUR TREATMENT:• Contact Margaret Gleeson at theAW Morrow Liver Centre, Monday - Friday8am - 4.30pm. Tel. 9515 7263• After hours: Call Liver Registrar on-callTel. 9515 6111• If you feel your illness is unrelated to your<strong>transplant</strong> or <strong>liver</strong> disease, you should seeyour local General Practitioner (GP)• If you are admitted to another hospital,please ask the team caring <strong>for</strong> you tocontact the <strong>transplant</strong> unit to in<strong>for</strong>m us ofyour condition
THE LIVER TRANSPLANT UNITSECTION 6:THE RIGHT DONOR FOR YOUSelection of a suitable donorIt is important to underst<strong>and</strong> that no one knowsexactly when a donor organ will be available <strong>for</strong>you. In Australia, only around 1% of all deathsoccur in such a way that organ donation ispossible. Injuries or illnesses that result in org<strong>and</strong>onation may include bleeding into the brain,accidents, infections or tumours. Potential org<strong>and</strong>onors are always on a mechanical ventilator<strong>and</strong> in hospital (because without a supply ofoxygen, organs would not be suitable <strong>for</strong><strong>transplant</strong>ation). The vast majority of org<strong>and</strong>onors in Australia are ‘Brain Dead’. Brain deathis the permanent loss of brain function which isdetermined by rigorous testing. Brain deadpeople are able to donate because the heart isstill beating blood around to the organs. Thealternate deceased donor is one who donatesafter ‘Cardiac Death’.Donation after Cardiac Death (DCD)Donation after cardiac death is a newer initiativeto allow more people to be deceased org<strong>and</strong>onors. These donors have severe <strong>and</strong>irreversible injuries or illnesses. Following anindependent decision by the family <strong>and</strong> treatingmedical team to withdraw active treatment,some <strong>families</strong> request that organ donation beconsidered. When suitable, organ donation canoccur in this setting particularly <strong>for</strong> kidneys, <strong>liver</strong><strong>and</strong> lungs. Following withdrawal of treatment,organs are retrieved as rapidly as possible afterthe donor has died (determined by the heartstopping) according to a strict NSW governmentapproved protocol. There is a small amount ofdamage that can occur during the dying phaseespecially to the <strong>liver</strong>, so the <strong>transplant</strong> doctorsare very selective about the donors they woulduse <strong>for</strong> <strong>liver</strong> <strong>transplant</strong>ation to minimiseproblems <strong>for</strong> the recipient.Equally important is the decision to donate. Ifthe deceased did wish to donate his/her organs<strong>and</strong> the family support that decision, then allsteps will be taken to ensure those wishes arefulfilled. Over 90% of Australians support org<strong>and</strong>onation ‘in-principle’. However, actual consentsin the hospital setting are lower, at around 50%.13Following rigorous tests to confirm brain death<strong>and</strong> after consent <strong>for</strong> organ donation is obtainedfrom the next of kin , the donor will be assessed<strong>for</strong> <strong>their</strong> suitability to donate. If the donor issuitable to donate organs, they will be taken tothe operating theatre <strong>for</strong> organ retrieval surgerythat takes several hours to complete. Donororgans are allocated by matching the bloodgroup, size of the donor <strong>and</strong> the recipient. The<strong>liver</strong> is offered to the neediest patient on thewaiting list who is the best match.Increasingly, donor organs that are offered <strong>for</strong><strong>transplant</strong>ation have some reason why they arenot absolutely optimal. With the poor org<strong>and</strong>onation rates in Australia, <strong>and</strong> the increasingnumber of people that need a <strong>transplant</strong>, evensuboptimal donor organs are considered <strong>for</strong><strong>transplant</strong>ation. Thus, donors may be older,have some evidence of excess fat in the <strong>liver</strong> orhave evidence of exposure to hepatitis virusinfection.Hepatitis C-positive donor <strong>liver</strong>s (that do nothave evidence of significant <strong>liver</strong> disease) areoffered to <strong>recipients</strong> with chronic hepatitis C. Inall patients with hepatitis C, the hepatitis Cinfection comes back after <strong>transplant</strong>, <strong>and</strong> thereis no evidence that the course of the hepatitis Cin the new <strong>liver</strong> is any different if the donor <strong>liver</strong>has hepatitis C as well. Such a <strong>liver</strong> will not beused in a recipient who does not already havehepatitis C.Some donors have evidence of previousexposure to another hepatitis virus, hepatitis B.In most of these cases the donor does not haveevidence of active infection, but on the basis ofblood tests, we can tell that there are smallquantities of the virus in the <strong>liver</strong>. Withoutpreventative medication, this virus can reactivatein the new <strong>liver</strong> <strong>and</strong> cause long-term problems.There<strong>for</strong>e, it is policy of <strong>transplant</strong> units to<strong>transplant</strong> such a <strong>liver</strong> <strong>and</strong> then to use highlyeffective preventative medicine (an extra tablet aday, called lamivudine) to prevent reactivation.If it is thought that it is in your best interest toaccept such a donor, the issues will bediscussed with you prior to proceeding to<strong>transplant</strong>.In all cases, the <strong>transplant</strong> team will consider thequality of the donor organ carefully, <strong>and</strong> will notINFORMATION MANUAL
THE LIVER TRANSPLANT UNITproceed to <strong>transplant</strong>ation if it is thought that therisks to the recipient are too high. A decision not toproceed may be made fairly early in the process,just after a recipient has been notified, or if new<strong>in<strong>for</strong>mation</strong> comes available, may be made evenafter the recipient has been transferred to theoperating room. While this is obviouslydisappointing, it is in the patient’s best interest notto proceed to <strong>transplant</strong>ation under suchcircumstances.WRITING TO THE DONOR FAMILYFor the family of an organ donor, receiving a cardor letter of thanks from a <strong>transplant</strong> recipient isvery special. Donor <strong>in<strong>for</strong>mation</strong> <strong>and</strong> details areconfidential, but if you would like to send ananonymous card or letter to the donors’ family,contact the Transplant Coordinator.INFORMATION MANUAL14
THE LIVER TRANSPLANT UNITSECTION 7:PREPARATION FOR SURGERYWhen a suitable donor has been foundWhen a suitable donor has been found, you willbe contacted <strong>and</strong> asked to activate the travelarrangements as discussed with the LiverTransplant Coordinator. The <strong>for</strong>m of transportchosen <strong>for</strong> your journey to the hospital willdepend upon your health <strong>and</strong> the distancetravelled. Private cars are the usual first option.Ideally, you should travel with at least onemember of your family, although this is notalways possible.Once the call has been received, you mustcommence fasting <strong>for</strong> surgery, that is, you mustnot have anything more to eat or drink.When you arrive at the hospital, you shouldreport to the Emergency Department. Youshould in<strong>for</strong>m the staff that you have been calledin to have a <strong>transplant</strong>.with your legal rights in the event of negligence.Following admission to hospital you will be askedto sign a separate hospital consent <strong>for</strong>m prior totransfer to the operating theatre.Cancellation of surgeryThe fact that you have been called to thehospital does not guarantee that you will have a<strong>transplant</strong>. It is quite possible that you could becontacted on more than one occasion withoutthe <strong>transplant</strong> going ahead. If the <strong>liver</strong> is foundto be unsuitable <strong>for</strong> you at any point then theprocedure will be cancelled These facts cansometimes only be ascertained in the last hoursbe<strong>for</strong>e the <strong>transplant</strong> goes ahead. In thesecircumstances, it is in your best interest not toproceed with the surgery.Consent <strong>for</strong> surgeryAt the time of entry on to the Waiting List orbe<strong>for</strong>e, you will be required to sign a “Consent<strong>for</strong> an operation <strong>for</strong> <strong>liver</strong> <strong>transplant</strong>ation”. A copyof this <strong>for</strong>m can be found on the at the back ofthis booklet. It says the risks from the operationare three kinds. Firstly, although every ef<strong>for</strong>t hasbeen made to screen the donor <strong>for</strong> transmissibledisorders, there can be no guarantee that thedonor did not have such a disorder. Secondly,the drugs required to control rejection have sideeffects specific <strong>for</strong> each drug. Thirdly, thecomplications of the operation itself includeinfection, bleeding, poor function <strong>and</strong> rejectionof the <strong>liver</strong>. There is a possibility (currently aboutone in ten) of death. This <strong>in<strong>for</strong>mation</strong> needs tobe explained to you in detail be<strong>for</strong>e you sign theconsent.You will need to sign that you underst<strong>and</strong> that<strong>liver</strong> <strong>transplant</strong>ation is a treatment <strong>for</strong> <strong>liver</strong>failure, not a cure, <strong>and</strong> that you underst<strong>and</strong> youwill need to take drugs to suppress rejectionindefinitely. You need to be satisfied with theexplanation of the risks of <strong>liver</strong> <strong>transplant</strong> <strong>and</strong>discuss it further with your doctors if you needto. Signing of the consent <strong>for</strong>m does not interfere15INFORMATION MANUAL
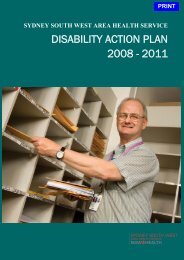
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 8:THE TRANSPLANT ITSELFThe surgical procedureThe diseased <strong>liver</strong> is removed <strong>and</strong> a normal <strong>liver</strong>is <strong>transplant</strong>ed into the space where thediseased <strong>liver</strong> was located, ie. on the right-h<strong>and</strong>side of the upper abdominal region. Thisrequires a large incision on the upper abdomen.The operation is very complicated <strong>and</strong> takesapproximately four to eight hours. Removing theold <strong>liver</strong> can be extremely difficult, particularly ifyou have had previous abdominal operations.Diagram of the operationFig.1IVCPortalVeinArteryDuring surgery your old diseased <strong>liver</strong> will beremoved <strong>and</strong> a new healthy looking <strong>liver</strong><strong>transplant</strong>ed in its place. (A gallbladder will notbe <strong>transplant</strong>ed with the <strong>liver</strong>).16The Liver Transplant Operation.The <strong>liver</strong> is attached to a number of vitalstructures, all of which have to be cut <strong>and</strong>rejoined.These are:o the inferior vena cava (IVC), the major veinthat drains into the heart above the <strong>liver</strong>o the portal vein, the vein that feeds bloodfrom the intestines into the <strong>liver</strong>o the hepatic artery that carries oxygen to the<strong>liver</strong>o the common bile duct, the major ducttransporting bile from the <strong>liver</strong> to theintestineOnce all these major structures have beenjoined from the donor <strong>liver</strong> to yours theabdominal cavity is washed with warm saline.Two white drains called Jackson Pratt drains areinserted into your abdominal cavity. They will beattached to another suction container. The fluidwhich drains into them will be blood stained.This is quite normal. Your abdomen is closed inlayers of muscle under the skin.You will be transferred to ICU from the operatingtheatre where the staff will observe the drainage.Once drainage ceases, the Jackson Pratt drainswill be removed, usually one to two days afterthe operation.Gall bladderBoth your own gallbladder (if you still have one),<strong>and</strong> the gallbladder attached to the <strong>transplant</strong>ed<strong>liver</strong> will be removed at the time of the operation.Do check with your surgeon if you have anyquestions.DressingsWe use clear dressings to cover the incision.The skin clips used to close the skin are visiblethrough them. The dressings are permeable towater vapour but impermeable to organisms.Sometimes blood or fluid will be visible but it willnot effect the skin healing. The dressings are lefton <strong>for</strong> up to 7 days. You are able to shower withthem on.Split-Liver TransplantationBecause of the disparity between the increasingnumbers of people waiting <strong>for</strong> <strong>transplant</strong>, <strong>and</strong>the numbers of donor <strong>liver</strong>s available, ways are
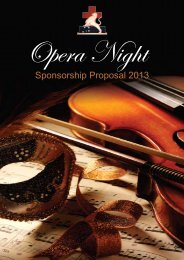
THE LIVER TRANSPLANT UNITalways being undertaken to increase the numberof people able to undergo <strong>transplant</strong>ation. Astrategy that is used in many <strong>transplant</strong> centresaround the world, including RPAH, is split-<strong>liver</strong><strong>transplant</strong>ation. In this procedure, a donor <strong>liver</strong>is divided in two parts, a larger right lobe, <strong>and</strong> asmaller left lobe (see figure 2). With this strategy,an adult <strong>and</strong> a child can be <strong>transplant</strong>ed fromthe same donor organ. Not all people waiting <strong>for</strong><strong>transplant</strong>s are suitable to have a right lobe<strong>transplant</strong> <strong>and</strong> the <strong>transplant</strong> team will alwaysselect an appropriate recipient. The chance ofdeveloping complications from a split <strong>liver</strong><strong>transplant</strong> is slightly higher than if a whole <strong>liver</strong>graft is used. Within the first few months after<strong>transplant</strong>ation, the split <strong>liver</strong> increases in sizeuntil it is the size of a full-sized <strong>liver</strong>. Since theimplementation of split <strong>liver</strong> <strong>transplant</strong>ation, thenumber of children waiting <strong>for</strong> <strong>transplant</strong>ation inAustralia has significantly reduced.Fig.2Donation after Cardiac Death (DCD)Livers retrieved from these donors (see section6.) have been under more stress than normaljust prior to the donor surgery. This can mean aslight increase in both early <strong>and</strong> latecomplications. Early on the experience is thatthere is a slightly higher risk of the <strong>liver</strong> notworking straight away after <strong>transplant</strong>. Later onthere seems to be a higher risk of problems withthe bile ducts. We reduce these risks by beingvery cautious about which of these <strong>liver</strong>s we willaccept <strong>for</strong> you.Transplantation from living donorsAdult to Child <strong>transplant</strong>ationLiver donation from living relatives to paediatric<strong>recipients</strong> is per<strong>for</strong>med when the circumstancesjustify it. The procedure is almost identical to thesplit procedure. There is a separate <strong>in<strong>for</strong>mation</strong>booklet <strong>for</strong> live donor <strong>transplant</strong> to paediatric<strong>recipients</strong>. If you are interested please speak tothe <strong>liver</strong> <strong>transplant</strong> coordinator.Figure 2. Split <strong>liver</strong> <strong>transplant</strong>ation. The left lobeis used <strong>for</strong> a child, <strong>and</strong> the right lobe is used <strong>for</strong>an adult.17Adult to Adult <strong>transplant</strong>ationA new initiative is adult to adult live donor <strong>liver</strong><strong>transplant</strong> where an adult patient can receive aportion of <strong>liver</strong> from a relative or close friend.The donor is a healthy adult 18-55years old. Thedonation must be completely voluntary. Thedonor undergoes rigorous testing to ensure <strong>their</strong>safety <strong>and</strong> that there is a good match with therecipient. The operation to donate a large part ofthe <strong>liver</strong> to an adult is a major one <strong>and</strong> carries arisk of dying that is as high as 1 in 200 chance.There is a separate <strong>in<strong>for</strong>mation</strong> booklet aboutadult to adult live donor <strong>liver</strong> <strong>transplant</strong>ation. Ifyou are interested, you should check with your<strong>transplant</strong> doctors to see if you are suitable <strong>and</strong>ask <strong>for</strong> a copy of the live donor <strong>transplant</strong>booklet.Survival chancesLiver <strong>transplant</strong>ation is a major operation.However, due to various recent advances theperi-operative mortality is now less than 10%.The 10-year post-<strong>transplant</strong> patient survival isabout 70%. No doubt, these figures willcontinue to improve.INFORMATION MANUAL
THE LIVER TRANSPLANT UNITSECTION 9: AFTER SURGERYIntensive careFollowing surgery you will return from theoperating theatre to the Intensive Care Unit,which is located on Level 3 of the hospital. Whenyou first wake up, you may be a little drowsy.The anaesthetic drugs take a while to wear off.You will be given pain relief intravenously duringthe early postoperative period. These can alsomake you sleepy. A stay in the intensive careunit allows your body time to recover its basicbodily functions (e.g. breathing, heart rate, bloodpressure).Most patients will have a breathing tube still inplace attached to a breathing machine called aventilator <strong>for</strong> the first 24 hours. You will alsohave a number of intravenous lines (tubes) inplace, one in your neck <strong>and</strong> also attached toblood vessels in your arms. You will have a nasogastrictube coming from your nose, a smalltube to empty your bladder <strong>and</strong> a number oftubes draining fluid from your abdomen. You willalso be attached to a heart monitor, which willrecord your vital signs. The staff who work in anintensive care unit have been specially trained tosee you safely through this period. Family will beallowed to visit once you are settled in intensivecare. If you cannot talk, you will be provided witha message board to write on. As time passes,the I.V. lines <strong>and</strong> drainage tubes will gradually beremoved. All tubes should be able to beremoved in the days following the operation.You will not be able to eat straight away, but canusually have something to drink within hours ofthe breathing tube being removed, <strong>and</strong>something to eat a day or so later.Your sleep pattern may be disrupted initially.This is not uncommon after major surgery <strong>and</strong> astay in the ICU, which can be noisy at night. Thehigh doses of anti-rejection medication dosesyou are given in the first few days can also bedisruptive to your sleep, but this usually settlesdown after a few days on the <strong>transplant</strong> ward.Your daily routine will include, daily blood tests,showering, wound dressings, assistance withactivities of daily living until you graduallybecome more independent. There will be regularward rounds by the Transplant Team, whichinclude Surgical <strong>and</strong> Medical Doctors. Yourmedications will be given intravenously at first,<strong>and</strong> then by mouth once you commence solidfood.Family <strong>and</strong> friends are encouraged to visit <strong>and</strong><strong>their</strong> help <strong>and</strong> support plays an important role inyour recovery. As you recover your health, youwill be expected to become more active. Thismeans spending more time out of bed, <strong>and</strong>walking a little more each day.The hospital has chaplains from manydenominations <strong>and</strong> religions. If you would like avisit from a member of your own religion, pleaselet the ward staff know.Recovery timeThe average stay in the Intensive Care Ward is 2to 3 days. The average stay in hospital wards is1 to 4 weeks. This may be extended due tocomplications. Most people, although well, takemany months to get over the effects of thesurgery <strong>and</strong> may not feel <strong>their</strong> normal selvesagain <strong>for</strong> several months.INFORMATION MANUALThe Transplant WardAfter a short stay in the intensive care unit youwill be transferred to the <strong>transplant</strong> ward onLevel 9. Once on the <strong>transplant</strong> ward you will beencouraged to mobilise as early as possible tofacilitate your recovery. You will have regularchest physiotherapy to help with your breathing<strong>and</strong> you will also be given breathing exercises todo. If at all possible the nursing staff will assistyou to get out of bed to shower by day two orthree at the latest.18
THE LIVER TRANSPLANT UNITSECTION 10:THE IMMUNE SYSTEMYou will be on anti-rejectiondrugs <strong>for</strong> the rest of your life.The immune system creates our defence againstinfectious organisms, such as bacteria <strong>and</strong>viruses, <strong>for</strong>eign substances or <strong>transplant</strong>edorgans, including a new <strong>liver</strong>.Your body will recognise your new <strong>liver</strong> as<strong>for</strong>eign tissue <strong>and</strong> your immune system willattempt to reject it. This is a normal reaction.After your operation, medications such astacrolimus/cyclosporin, prednisone <strong>and</strong>mycophenolate/azathioprine are used to loweryour body’s immune response(immunosuppression), so as to lessen thechance of rejection.These medications do result in less rejection.However, because they alter your immuneresponse, they also make you more likely tosuffer from infections, because the immunesystem also serves as a defence mechanismagainst bacteria <strong>and</strong> viruses entering your body.In many ways your medication treatment is acareful balancing act - to give enough so thatyour body does not reject your new <strong>liver</strong> but nottoo much so as to predispose you to infectionsor other side-effects. Because these medicationshave such an important function, they aremedications that you will always have to take.You will also have to be closely followed by theTransplant Team.Despite the tremendous progress in <strong>liver</strong><strong>transplant</strong>ation, it is still not a cure. It is atreatment <strong>for</strong> your <strong>liver</strong> disease. This is why it isso important <strong>for</strong> you to follow the medication <strong>and</strong>lifestyle regime that will be recommended <strong>for</strong>you. Your ef<strong>for</strong>ts, together with those of theTransplant Team, are intended to increase yourquality of life <strong>and</strong> return you to as normal life aspossible. Complications that can be preventedwill be picked up early with regular follow-up<strong>and</strong> allow treatment to be given straight away.19INFORMATION MANUAL
THE LIVER TRANSPLANT UNITSECTION 11: INFECTIONWith immunosuppression, your ability to fightinfection is decreased; this is particularly so inthe first few months when the doses ofimmunosuppressive medications are relativelyhigh.Common sense precautions need to be taken:avoid exposure to sources of infection, such aspeople with the flu <strong>and</strong> colds, children withchicken pox or other viral infections, dirty <strong>and</strong>dusty buildings (buildings under construction ordestruction), <strong>and</strong> large compact crowds at leastinitially. Normal hygiene precautions should helpprevent infection <strong>and</strong> no extra measures need tobe taken.Care of your skin is very important. If a cut orgraze does occur, cleanse the area <strong>and</strong> apply aclean, dry dressing or plaster <strong>and</strong> watch <strong>for</strong>signs of infection. Should healing be prolonged<strong>and</strong>/or pain, swelling, redness, or infection benoted, you should notify your GP or theTransplant Team. Symptoms of cystitis (urinarytract infection), sore throat, cold sores or mouthsores should also be reported to your GP or yourTransplant doctor if visiting clinic.As your general health improves, the dosages ofyour immunosuppressive medications areusually reduced, which means that you willregain resistance to most infections.Pay careful attention to personal hygiene. Thisinvolves regular showering <strong>and</strong> keeping yourmouth clean, regular brushing of your teeth aftereach meal <strong>and</strong> last thing at night with a softtoothbrush.INFORMATION MANUAL• Avoid changing cat litter boxes or birdcages; they can be major sources ofinfection• Wash your h<strong>and</strong>s as often as possible20
THE LIVER TRANSPLANT UNITSECTION 12: REJECTIONRejection is common following <strong>liver</strong><strong>transplant</strong>ation. Your body recognises the<strong>transplant</strong>ed <strong>liver</strong> as a <strong>for</strong>eign object <strong>and</strong> tries todestroy it through a process known as rejection.It is not uncommon to experience one or moreepisodes of rejection during the recovery period.It most commonly occurs 7 - 10 days aftersurgery. It is controlled in over 90% of cases bytransient increases in medication.The chances of rejection diminish with time, butrejection can occur at ANY TIME following<strong>transplant</strong>ation. Frequently an episode ofrejection is not associated with symptoms,however it is important that you be aware ofsome signs <strong>and</strong> symptoms of possible rejection.- Intravenous steroids (IV methylprednisolone)(a ‘pulse’)- Other immunosuppressive drugs such asAzathioprine (Imuran), Mycophenolate(Cellcept) or ATG.The onset of rejection does not mean that your<strong>liver</strong> will be lost but prompt treatment isimportant.Very rarely, a <strong>transplant</strong>ed <strong>liver</strong> fails to functionor undergoes irreversible rejection. There is nodialysis treatment <strong>for</strong> <strong>liver</strong>s as with kidneys.Thus, if a <strong>liver</strong> fails completely, the only hope is<strong>for</strong> a second <strong>transplant</strong>.Signs <strong>and</strong> symptoms of rejection mayinclude:1. Fatigue, lethargy or malaise2. Lack of appetite3. Fever4. Abdominal pain or tenderness5. Light coloured stools (faeces from thebowel)6. Dark coloured urine7. Yellow eyes <strong>and</strong> skin8. Elevations in <strong>liver</strong> function tests9. Flu-like symptoms - fever, joint <strong>and</strong>muscle pain.If you develop any of these signs or symptoms ofrejection once you leave hospital, notify the LiverTransplant team. However these symptoms donot always appear be<strong>for</strong>e a rejection episode.Many episodes are picked up by routine bloodtests at the time of your outpatient visits. Abiopsy may be required to make a definitivediagnosis.Rejection may be mild or severe. In most cases,<strong>liver</strong> rejection can be controlled satisfactorily iftreated promptly.There are many methods <strong>for</strong> controlling rejection<strong>and</strong> they may include:- Tacrolimus or Cyclosporin dosageadjustment21INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 13: NUTRITIONFOLLOWING LIVERTRANSPLANTATIONYour diet during your hospital stayafter <strong>transplant</strong>ationMost patients do not start to eat until the secondor third day after the <strong>transplant</strong>. Your first mealwill usually consist of fluids <strong>and</strong> you will progressrapidly to a full ward diet.By the end of the first week of eating you willfind that the nursing staff, the doctors <strong>and</strong> thedietitian are all very concerned about how muchfood you are eating <strong>and</strong> you will receive constantinquiries about your food <strong>and</strong> fluid intake.The reason <strong>for</strong> the concern is that most patientscome to <strong>transplant</strong> in a malnourished state inspite of pushing themselves hard to eat. Manystudies have shown that people who are poorlynourished take longer to recover <strong>and</strong> longer toheal <strong>their</strong> wounds after an operation <strong>and</strong> may bemore susceptible to infections.There are studies to show that <strong>liver</strong> <strong>transplant</strong><strong>recipients</strong> need a high protein intake as well as ahigh-energy intake in the period after theoperation. It also seems that <strong>liver</strong> <strong>transplant</strong>patients go through a period where they needlots of calories just to maintain <strong>their</strong> weight <strong>and</strong>in fact may lose weight rapidly even on a veryhigh energy intake.At this stage eating may seem to be one of thehardest things you have ever had to do. You willreceive constant reminders from all theTransplant Team about eating enough food tohelp your wound to heal <strong>and</strong> to prevent furtherweight loss.You will be asked to supplement your intake withhigh protein drinks such as Resource Protein,Fortisip, Resource Fruit Beverage or Sustagen .You may receive large meals. You are notexpected to eat all the food at one meal butrather to spread it out over the day, so that youspend your day grazing. Your family is22encouraged to bring in some of your favouritehome-prepared foods in an ef<strong>for</strong>t to increaseyour intake.Occasionally it may be necessary to supplementa patient’s intake by feeding through a fine tubewhich passes from the nose down the back ofthe throat <strong>and</strong> into the stomach. This happenswhen the team identifies that the patient iseating poorly, <strong>and</strong> not able to drink enoughsupplements in the presence of significantweight loss or poor wound healing. This feedingmay be either over twenty fours hours or onlyovernightThe dietitian will monitor your weight <strong>and</strong>nutritional progress closely <strong>and</strong> you willconstantly be pushed to increase your protein<strong>and</strong> energy intake. It will be reassuring <strong>for</strong> you toremember that these increased requirements donot last <strong>for</strong>ever.The dietitian will discuss your ideal or preferredweight with you. When you are nearing this goalyou will need to reduce your food intakedramatically, as there is a great tendency to gainweight rapidly several months after <strong>transplant</strong>.Long-term weight control may be a seriousproblem in the future if you do not reduce yourintake when advised to do so.Any dietary restrictions that were needed be<strong>for</strong>eyour <strong>transplant</strong> are no longer necessary. Somepatients have high blood sugar levels after <strong>their</strong><strong>transplant</strong> <strong>and</strong> this may be related to <strong>their</strong>medication doses. It is not necessary to go ontoa special diet to control the blood sugar levels atthis stage. Insulin is used to control blood sugarlevels as it is much more important to eatenough foods rich in protein <strong>and</strong> energy orcalories. As the medication is reduced the bloodsugar levels often normalise.If you continue to have problems with fluidretention after the <strong>transplant</strong> reducing your saltintake may help to make it easier to control theexcess fluid.
THE LIVER TRANSPLANT UNITYour diet when you go home after<strong>transplant</strong>Around two to three months after leavinghospital the emphasis on eating changes.Food starts to taste good again, your appetiteincreases <strong>and</strong> you start to gain weight.Un<strong>for</strong>tunately this combined with the fact thatyou now have a <strong>liver</strong> that works <strong>and</strong> the highprednisone doses means that it is now all tooeasy to gain weight.Prednisone has the effect of stimulating yourappetite at the doses you are taking when you gohome. Patients frequently say that they nolonger know when they have eaten enough <strong>and</strong>that they are always hungry. They also say thatthis effect may last <strong>for</strong> years.It is very important to reduce your food intakewhen you are within three to four kilograms ofyour goal or desired weight. You will gain theremaining weight without really trying.Weight control is the most important nutritionalissue when you are discharged after<strong>transplant</strong>ation. Rapid excessive weight gainmay affect your <strong>liver</strong> function tests. Regularexercise <strong>and</strong> a sensible eating plan will help tocontrol your weight.Your exercise program should start from the timeyou leave hospital even if you are stillsignificantly underweight at this stage. Gentleregular exercise will not harm your new <strong>liver</strong> norwill it open up the scars.The following guidelines will help you in thestruggle to control your weight:• Try to eat regular meals• Frequent snacking between meals will makeit difficult <strong>for</strong> you to control your weight. Ifyou need to eat between meals, choosehigh-fibre foods such as crisp crunchyvegetables. Vegetable soups are oftensatisfying on a cold winter’s day <strong>and</strong> are lowin fat <strong>and</strong> calories.• High fat foods are high in calories orkilojoules. Try to choose the reduced fatalternatives at all times. These include leanmeats, lean poultry, fish, reduced-fatspreads <strong>and</strong> low-fat or reduced-fat dairy23products. Try to avoid fried foods <strong>and</strong> foodsladen with oil or cream.• Fluids are important. Choose low caloriedrinks such as iced water, tea or coffeewithout sugar, plain mineral water or sodawater, diet soft drinks <strong>and</strong> diet cordial.• Vegetables, including potatoes <strong>and</strong> cerealssuch as bread, rice <strong>and</strong> pasta shouldprovide the basis of your meals with smallerserves of lean meats, lean poultry, fish etcrather than the other way around.• Choose fresh fruit or fresh fruit combinationsto finish off a meal rather than the highercaloriealternatives.• Sucking sweets or lollies or eatingchocolates regularly makes it difficult tocontrol your weight.Some patients may go home with high bloodsugar levels <strong>and</strong> may require insulin injections ortablets to control <strong>their</strong> blood sugar levels. If thispersists <strong>for</strong> six months you will need to go on toa special diet to make it easier to control yourblood sugar levels. Regular exercise also makesit easier to control your blood sugar levels.The dietitian will discuss your diet details withyou <strong>and</strong> your family prior to discharge. This willbasically involve eating at regular intervals withan emphasis on reducing the amount of fat youeat <strong>and</strong> avoiding foods with a high concentrationof sugar.You may find that your blood sugar levelsnormalise within twelve months after<strong>transplant</strong>ation <strong>and</strong> that you are then able to eatan unrestricted diet. Remember, that if this doeshappen then you still have the ability to gainweight easily.Fluid retention may be a problem even by thetime you go home. Avoiding added salt <strong>and</strong> foodwith an obviously high salt content would assistin controlling this excess fluid. Many patientsmay have been on a salt restriction prior to<strong>transplant</strong>ation. It is not necessary to limit yoursalt intake as severely after your <strong>transplant</strong>.As <strong>transplant</strong>ed patients are immunosuppressedit is important to be aware of the possibility offood poisoning. There are two bacteria inparticular which may be a serious problem <strong>for</strong>patients who may be immunosuppressed. TheyINFORMATION MANUAL
THE LIVER TRANSPLANT UNITare Listeria monocytogenes <strong>and</strong> Vibriovulnificans.Vibrio vulnificans is a bacterium that may bepresent in raw shellfish. It is particularly harmfulin people with a suppressed immune system.Although contamination with the bacteria is rare,all <strong>transplant</strong> patients are advised not to eat anyraw shellfish.Listeria monocytogenes is a bacterium that ismore widespread in our food supply. It also lovesto grow in the cold. Keeping foods in therefrigerator will not safeguard you from this“bug”. Careful h<strong>and</strong>ling of food <strong>and</strong> anawareness of possible contamination of specificfoods will help prevent infection. You will receivea detailed brochure about this “bug” <strong>and</strong> itspossible food sources from the dietitian whenyou have your <strong>transplant</strong>.Finally, you always have access to the <strong>liver</strong><strong>transplant</strong> dietitian. If you have any inquiriesabout your nutrition at any stage, you should nothesitate to contact the dietitian. Similarly if youare having difficulty controlling your weight athome after your <strong>transplant</strong> you should contactthe dietitian earlier rather than later.You can contact the dietitian through theDepartment of Nutrition <strong>and</strong> Dietetics - telephonenumber (02) 9515 8053. Alternatively you canask the staff at the Liver Transplant clinic tocontact the dietitian.INFORMATION MANUAL24
THE LIVER TRANSPLANT UNITSECTION 14: RECURRENCE OFORIGINAL DISEASERecurrence of your original disease may occur,particularly if your original disease is due to viralhepatitis. B or C. Hepatitis B recurrence afterthe <strong>transplant</strong> was previously fairly high riskwithout preventative treatment. Nowadays thereis good preventative treatment available againstrecurrence, in the <strong>for</strong>m of anti viral drugs thatact against the hepatitis B virus. Treatment isusually commenced in the pre-<strong>transplant</strong> phase<strong>and</strong> continues indefinitely post <strong>transplant</strong> inconjunction with regular monthly injections ofHepatitis B Immunoglobulin.Recurrence of the Hepatitis C virus is universalfollowing <strong>transplant</strong>ation. The majority ofpatients will have a mild recurrence which willnot cause significant problems <strong>for</strong> the first fiveyears after <strong>transplant</strong>. Problems beyond thistime may emerge. A small group of patients willdevelop a more severe recurrence with thedevelopment of cirrhosis within three to fiveyears of <strong>transplant</strong>ation. Most patients who havea <strong>transplant</strong> <strong>for</strong> hepatitis C will have regular <strong>liver</strong>biopsies (perhaps once or twice a year) tomonitor <strong>for</strong> any damage caused by the virus.Your <strong>transplant</strong> doctor may make alterations toyour immunosuppression medications <strong>and</strong> mayrecommend a course of antiviral treatment withpeginterferon <strong>and</strong> ribavirin. Some patients canclear hepatitis C infection after <strong>transplant</strong> witha course of antiviral treatment. This is an areaof active research <strong>and</strong> treatments are beingdeveloped to prevent <strong>and</strong> treat viral recurrencepost <strong>transplant</strong>.If you had a <strong>liver</strong> cancer in your old <strong>liver</strong>, there isa possibility this may recur after <strong>transplant</strong>ation.Your doctors will take all steps to minimise thechance of this occurring, but it is always a risk.Recurrence of <strong>liver</strong> cancer, may first be noticedin the bones or the lungs, rather than in the new<strong>liver</strong>. Your doctor will be constantly monitoringyour condition.Recurrence of primary biliary cirrhosis,autoimmune chronic active hepatitis <strong>and</strong>primary sclerosing cholangitis are reported butthe incidence is rare.25INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALSECTION 15: DRUGS USED INTRANSPLANTATIONIn order to control rejection a combination ofdrugs are given which suppress or reduce theeffectiveness of the body’s immune system.These drugs are called immunosuppressives<strong>and</strong> must be taken <strong>for</strong> life. Other drugs are used<strong>for</strong> a period of time after <strong>transplant</strong> to preventinfections <strong>and</strong> to manage other health problems.All patients will have a MEDICATION CARD, onwhich current medications <strong>and</strong> dosages arerecorded. This card should be brought to allclinic appointments.Immunosuppression DrugsLife-long immunosuppression is necessary <strong>and</strong>tablets must be taken daily. Some patients mayremain on a small dose of prednisone. Currently,most patients also take tacrolimus (Prograf) orcyclosporin (Neoral) twice daily, with the dosebeing decided on the basis of blood test levelstaken just be<strong>for</strong>e the morning dose is due. Somepatients require a third drug, azathioprine(Imuran) or mycophenolate (Cellcept), takenonce or twice a day. All drugs as an outpatientare taken orally (by mouth).Side-effectsAny <strong>for</strong>m of long-term immunosuppressionbrings with it an increased risk from infection.The risk is highest during high-dose prednisonetherapy, so during such times patients need tobe isolated from anyone suffering from aninfection. Other risks include the developmentof diabetes, high blood pressure, highcholesterol <strong>and</strong> kidney damage. Most of thesecomplications can be managed by reducing orchanging the immunosuppressive drugs or usingadditional medications. In the long-term, there isalso a slightly increased risk of malignancy inpatients taking immunosuppressive drugs.These risks have to be balanced against thenecessity to take the drugs that prevent the bodyfrom rejecting the <strong>liver</strong>.There are three main drugs used <strong>for</strong> <strong>liver</strong><strong>transplant</strong> patients <strong>and</strong> your <strong>liver</strong> specialist willdetermine which drugs <strong>and</strong> dosages are bestsuited to you.26Here is a list of the drugs that may be used aftera <strong>liver</strong> <strong>transplant</strong>, giving the reasons <strong>for</strong> <strong>their</strong> use<strong>and</strong> possible side effects.Tacrolimus (FK506) (Prograf)Stops special white cells (T cells) from becomingactive in your blood <strong>and</strong> attacking your<strong>transplant</strong>ed <strong>liver</strong>Tacrolimus <strong>and</strong> cyclosporine are similar drugs<strong>and</strong> work in a similar way but have somedifferent side effects. Tacrolimus/Cyclosporin arethe mainstay of the immunosuppression post<strong>liver</strong> <strong>transplant</strong>. Doses are adjusted according toblood levels. They are never used togetherbecause of <strong>their</strong> shared toxicities.Side effects of Tacrolimus include:i) impaired kidney function (picked up onroutine blood tests).ii) increase in blood pressure.iii) neurological side effects that includeheadaches, mild tremors, insomnia,possible nightmares. Rarely patients mayexperience severe side effects includingconfusion, seizures <strong>and</strong> coma.iv) raised blood sugar levels or diabetes.v) increased risk of infection.vi) raised potassium level.vii) nausea <strong>and</strong> vomiting.viii) mild hairlossCyclosporin (Neoral)Again Cyclosporin is a strongimmunosuppressive drug that stops specialwhite cells (T-cells) from becoming active in yourblood <strong>and</strong> attacking your <strong>transplant</strong>ed <strong>liver</strong> thatnormally fight against <strong>transplant</strong>ed tissueintroduced into your body. It is almost alwaysgiven along with prednisone.Side-effects of Cyclosporin include:i) impaired kidney function (picked up onroutine blood tests).ii) high blood pressure.iii) hot flushes or sweating.iv) numbness or tingling in the h<strong>and</strong>s, feet ormouth.v) shaking or trembling h<strong>and</strong>s <strong>and</strong> feet, butthis decreases with the reduction in doseover time.vi) hair growth, most commonly noted on theface, arms <strong>and</strong> legs but this decreaseswith reduction in dose over time.
THE LIVER TRANSPLANT UNITvii) overgrowth of gums, sometimesassociated with soreness, swelling <strong>and</strong>redness, hence the need <strong>for</strong> regularmouth care.viii) sinus drainage, “runny” or “stuffy” nose.ix) increased risk of infection.How to take your Tacrolimus(Prograf) or Cyclosporin (Neoral).i) Tacrolimus/cyclosporin is given in twodivided doses 12 hours apart usuallytaken at 8am <strong>and</strong> 8pm.ii) It is very important to taketacrolimus/cyclosporin regularly exactlyas prescribed. You must not alter thedose or time taken without medicaladvice.DO NOT RUN OUT OF CAPSULES.iii) Tacrolimus/cyclosporin is usuallydispensed initially through the hospitalpharmacy. In patients who are onstable doses, the medication may beavailable from your local pharmacyusing an Authority Script.iv) Do not take your Tacrolimus orCyclosporin prior to having your bloodtaken on the morning of your visit.Bring your morning dose of medicationwith you <strong>and</strong> take as soon as possibleafter the test. Some people takingCyclosporin will be asked to have <strong>their</strong>blood tests exactly 2 hours after takingthe morning dose.Generic MedicationThere are now some generic br<strong>and</strong>s ofimmunosuppression medication on the market.You may be dispensed one of these if you getyour medications from a pharmacy other thanhere at RPA. As a general rule, it is preferredyou continue on the same br<strong>and</strong> as supplied bythe hospital. Please discuss with your Doctorbe<strong>for</strong>e taking any generic immunosuppression.27Once Daily TacrolimusSome patients on stable doses of twice dailytacrolimus may be swtiched to a once dailyprolonged release <strong>for</strong>mulation (Prograt XL). Thisshould be taken at least 1 hour be<strong>for</strong>e breakfastor 2-3 hours after breakfast. It is much easier toremember to take a capsule once a day! Bloodtests to monitor the level are taken just prior totaking the next dose.Prednisone is a steroid hormone similar tocortisol, which your body produces normally. Itreduces the number of circulating white cells inthe blood by dampening down the inflammatoryresponse. The dose given is initially high post<strong>transplant</strong> <strong>and</strong> is gradually tapered down untilyou are on fairly small dose. It is given inconjunction with other drugs to preventrejection.Side-effects include:i) Stomach irritation that may occasionallycause stomach ulcers. Never takeprednisone on an empty stomach so youshould take it after breakfast each day.ii) Fluid retention, high blood pressure <strong>and</strong>swelling of the face, h<strong>and</strong>s or ankles.iii) Weight gain due to an increase in yourappetite <strong>and</strong> subsequent increase in foodintake.iv) Increased risk of infection, especially inthe first few months after <strong>transplant</strong>ationwhile your prednisone dose is high.v) High blood sugar (diabetes) may occurwith high doses of prednisone therapy.This is called “steroid-induced” diabetes.If you are a diabetic, you may requireadditional insulin to maintain a normalblood sugar. You will be instructed in adiet that will help you control this sideeffectif necessary.vi) Skin changes such as acne, rashes orbruising.vii) Mood changes that may swing fromfeeling “up” to feeling “down”.viii) Softening of the bones (osteoporosis)can be experienced after long-term useof steroids. A diet high in calcium orsupplementation with calcium <strong>and</strong>vitamin D capsules will help, <strong>and</strong> theprednisone dose is reduced as soon aspossible after <strong>transplant</strong>.INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALNEVER STOP OR REDUCE PREDNISONEWITHOUT MEDICAL ADVICEAzathioprine (Imuran)Azathioprine is used <strong>for</strong> the suppression of yourimmune response. It acts on the bone marrowby decreasing the number of white blood cellswhich fight infection. With azathioprine there isan increased risk of infection <strong>and</strong> an increasedtendency <strong>for</strong> skin cancers.Side-effects include:i) Bone marrow depression - a low whitecell count is the most common problem,but a low platelet count <strong>and</strong> anaemia mayoccur.ii) Nausea or vomiting - so take your Imuranafter meals to lessen stomach upset.iii) Occasionally, people are allergic toazathioprine, <strong>and</strong> are unable to take it.Mycophenolate mofetil (Cellcept)One of the newer immunosuppressantmedications similar to azathioprine that may beadded to some patients drug regimen. It is takentwice a day 12 hours apart.Side – effects include:i) Vomitingii) Diarrhoeaiii) Low white cell countSirolimus/RapamycinThese belong to a newer generation ofimmunosuppressant drugs. They act bystopping special white cells (T cells) frombecoming active in your blood <strong>and</strong> attackingyour <strong>transplant</strong>ed <strong>liver</strong>. They have a differentside effect profile from tacrolimus/cyclosporine.They are taken once a day <strong>and</strong> the dose given isdependent on the level of the drug in your blood.Side – effects include:(i) Hyperlipidemia (high cholesterol levels inthe blood)(ii) Abdominal pain <strong>and</strong> diarrhoea(iii) Low red blood cell count (anaemia)(iii) Low white blood cell count(iv) Low platelet count (thrombocytopenia)(v) Acne <strong>and</strong> rash28Other Drugs used after TransplantationValganciclovir (Valcyte)Ganciclovir is used <strong>for</strong> the prevention <strong>and</strong>treatment of CMV (cytomegalovirus) viralinfection. This is a viral infection <strong>transplant</strong>edpatients may be prone to because of <strong>their</strong>suppressed immune systems <strong>and</strong> usuallyreactivates from prior infection in either therecipient or donor. It is given as capsules <strong>for</strong>3-6 months after <strong>transplant</strong>ation. Some patientsmay still develop CMV once ganciclovir tabletsare stopped <strong>and</strong> this will require treatment witheither intravenous (through a vein) gancicloviror oral (by mouth) valganciclovir.Valaciclovir (Valtrex)Valaciclovir is used <strong>for</strong> prevention <strong>and</strong> treatment<strong>for</strong> viruses know as herpes simplex (causingcold sores) <strong>and</strong> varicella zoster (which causeschickenpox). A large proportion of thepopulation have been exposed to the herpesvirus <strong>and</strong> it may become activated during timesof stress, or when a person isimmunocompromised (lowered resistance toinfection, by medication or disease). Thismedication is not used routinely after <strong>transplant</strong>.Bactrim/ResprimOne Bactrim/Resprim tablet is given three timesa week to all patients after <strong>transplant</strong> to preventa type of chest infection called Pneumocystiscarinii (PCP) which immunosuppressed patientsmay be prone to. This medication is continued<strong>for</strong> 12 months.PentamidineThis is an alternative drug to Bactrim, which isused as preventative treatment <strong>for</strong> PCP, <strong>for</strong>patients who are allergic to Bactrim or those whohave a low white cell count. It is inhaled througha nebuliser once a month <strong>for</strong> 12 months.FluconazoleFluconazole is a medication used <strong>for</strong> treatment<strong>and</strong> prevention of yeast infections. An exampleof a yeast infection is thrush. Fluconazole mayinteract with some of the other medications,so it is important not to start or stop fluconazolewithout direction from your <strong>transplant</strong> doctor. Itis usually stopped 1-2 months after <strong>transplant</strong>.
THE LIVER TRANSPLANT UNITAntihypertensivesAntihypertensives are drugs used to treat highblood pressure. Patients taking Cyclosporin orTacrolimus often get an increase in <strong>their</strong> bloodpressure. If this occurs, a variety of medicationscan be used.Listed below are other medications that may berequired after a <strong>transplant</strong>:InsulinInsulin may be required <strong>for</strong> patients who havehigh blood sugar levels after <strong>transplant</strong>.Oral diabetes medicationsSome patients develop only mild diabetes thatcan be managed with tablets such as gliclazide(Diamicron) or met<strong>for</strong>min (Diabex, Glucophage).Acid-lowering medications (proton-pumpinhibitors)Rabeprazole (Pariet), pantoprazole (Somac),esomeprazole (Nexium) <strong>and</strong> similar drugs areused to prevent the development of stomachulcers that can be caused by stress <strong>and</strong>/orprednisone.DRUG INTERACTIONSMany drugs have the potential to interact withyour <strong>transplant</strong> medications.Please check with your doctor about thepossibility of any drug interactions with your<strong>transplant</strong> medications be<strong>for</strong>e commencing anynew medication.Drugs that may increase blood levels oftacrolimus/cyclosporin include macrolideantibiotics such as erythromycin orroxithromycin (Rulide), antifungal medicationssuch as fluconazole, certain blood pressuremedication (calcium channel blockers), <strong>and</strong>grapefruit juice.Levels may be lowered by other medications,including rifampicin, St John’s Wort, <strong>and</strong> antiepileptics.Over-the-counter drugsCheck with your physician be<strong>for</strong>e you take ANYover-the-counter medications, such as cold orcough medications. These medications maymask a serious infection that must beinvestigated by your doctor. Unless specificallyordered by your physician do not take aspirin oranti-inflammatory drugs such as ibuprofen29(Nurofen), as they may cause stomach irritation<strong>and</strong> kidney impairment.Paying <strong>for</strong> your drugsOnce you are discharged you will be responsible<strong>for</strong> paying <strong>for</strong> your own drugs. This can beexpensive, especially at the beginning. You maybe entitled to one of the various concessioncards. Check with the Social Worker about this.As well, you will probably be able to takeadvantage of the Safety Net Scheme. Make sureyou keep your Prescription Record up-to-date sothat you will know when your safety net total isreached.You will then be able to get your drugs at areduced rate. Please talk with the pharmacistor Social Workers if you need further <strong>in<strong>for</strong>mation</strong>about these schemes.Compliance: a crucial factorWhen you, as a patient, are said to be“compliant”, it simply means that you are, to thebest of your ability, following the instructions ofthe doctors, nurses, <strong>and</strong> other professionalsresponsible <strong>for</strong> your care. Specific examples ofcompliance include:• not missing any of your follow-up visits <strong>and</strong>laboratory tests• exercising regularly <strong>and</strong> maintaining yourweight• learning all you can about the long-termcare of your <strong>transplant</strong>However, <strong>for</strong> <strong>transplant</strong> <strong>recipients</strong> the mostimportant aspect of compliance is taking yourmedication exactly as the <strong>transplant</strong> teaminstructed you - without missing a single dose -even if you feel fine. For as long as you have a<strong>transplant</strong>, you will have to takeimmunosuppressive drugs. Not taking yourimmunosuppressive medication at the right time<strong>and</strong> in the correct amount is one of the mostcommon reasons <strong>for</strong> rejection <strong>and</strong> <strong>transplant</strong>failure.INFORMATION MANUAL
THE LIVER TRANSPLANT UNITSECTION 16: PATIENTINFORMATION ABOUT DRUGTRIALSTransplantation has been improving steadily overthe years because of better surgical techniques<strong>and</strong> better use of immunosuppressive drugtherapy.In most <strong>transplant</strong> centres clinical trials arecarried out with the aim of finding the bestregime of immunosuppression to improve organsurvival rates, decrease the number of rejectionepisodes <strong>and</strong> to reduce side effects.The usual means of carrying out these trials isby comparing the “new” treatment with the bestavailable st<strong>and</strong>ard treatment. This is called acontrolled clinical trial.Where does this fit in <strong>for</strong> me as a patient on the<strong>transplant</strong> list? The <strong>transplant</strong> team will discussany clinical trials that the Liver Transplant Unit atRoyal Prince Alfred Hospital is currently involvedin. All trials are approved by the Ethics ReviewCommittee at the hospital. You may be invited toparticipate in such a clinical trial, <strong>and</strong> if so, youwill be provided with a written In<strong>for</strong>mation Sheet.By taking part in a trial you may have access totreatments that are not currently approved inAustralia <strong>and</strong> will also be helping to advancemedical science <strong>and</strong> thus improve prospects <strong>for</strong>patients in the future. Remember if you chooseto participate in a trial it should be your choice.If you choose not to participate you will receivethe st<strong>and</strong>ard treatment in use at the time.INFORMATION MANUAL30
THE LIVER TRANSPLANT UNITSECTION 17: OTHER POST-TRANSPLANT PROBLEMSYou may not have any problems after your<strong>transplant</strong> but most people experience at least afew minor or possibly more serious problems.These are some of the problems <strong>transplant</strong>patients may experience:-InfectionYou will be given fairly high doses ofimmunosuppressant medications during yourearly postoperative period to overcome the riskof your body rejecting your new <strong>liver</strong>. This willmake you more susceptible to infection. You willbe monitored <strong>for</strong> the presence of any infectionon an ongoing basis while you are recovering inhospital following your <strong>transplant</strong>. Any infectionthat is of concern will be treated promptly withappropriate antibiotics.During the first few weeks following <strong>transplant</strong>the most common sites of possible infection areyour chest, (particularly if you are not coughing<strong>and</strong> doing your breathing exercises) <strong>and</strong> yourwound.If you had a lot of ascites prior to <strong>transplant</strong>, thistends to persist <strong>for</strong> a short period after the<strong>transplant</strong> operation. It will eventually disappear,but is prone to cause infection <strong>and</strong> leakage.Wound ComplicationsIf wound infections develop, treatment consistsof opening the wound, changing the dressings,<strong>and</strong> allowing healing to occur spontaneously.You will also require antibiotic therapy.Occasionally infection may develop in theabdominal cavity, if this should happen it wouldbe diagnosed <strong>and</strong> treated promptly. A surgicalprocedure may be required.DiabetesThere is an increase in the frequency of diabetesin the first year following <strong>transplant</strong>. This is dueto the side effects of two of the <strong>transplant</strong>medications, in particular, prednisone <strong>and</strong>Tacrolimus. This often settles down over time asthe doses of your immunosuppressivemedication are reduced.Drugs that lower blood sugar levels may berequired. This may take the <strong>for</strong>m of tablets (oral31hypoglycaemic agents) or Insulin by injection.If it is likely that you will be discharged homerequiring regular Insulin injections, educationwill be provided by specialist Diabetic Sisters.Arrangements will be made <strong>for</strong> you to befollowed by the RPAH Diabetes Centre or yourown doctor.CMV InfectionPrior to the routine use of valganciclovir (Valcyte)after <strong>transplant</strong>, this was quite a commoninfection that could cause fevers, aches <strong>and</strong>pains <strong>and</strong> diarrhoea. Now it is extremelyuncommon early after <strong>transplant</strong> but may comeon weeks to months after stoppingvalganciclovir. If you get this infection, you willreceive anti-viral treatment (either oralvalganciclovir or intravenous ganciclovir) <strong>and</strong>may require admission to hospital.Other possible post operative problemsThese include problems related to the flow ofbile from your <strong>liver</strong>, either a bile leak (whichusually results in abdominal pain) or thedevelopment of a stricture (narrowing) in one ofthe bile ducts which may cause abnormal <strong>liver</strong>tests <strong>and</strong> jaundice. There may be problems withflow with the blood vessels going into the <strong>liver</strong>.These complications may require invasiveprocedures or even surgery to correct.Emotional changes to expectNot only does <strong>transplant</strong>ation involve manyphysical changes to the body, but it also meansmany emotional changes. It is a tense, anxioustime <strong>for</strong> both patient <strong>and</strong> family while they livethrough the waiting period, the <strong>transplant</strong> itself<strong>and</strong> often a prolonged recovery period. Along theway they may encounter <strong>and</strong> have to cope withmany problems as they occur.The drugs given produce physical side effectsthat can be distressing to patients as they facechanges in <strong>their</strong> body image <strong>and</strong> can alsocontribute to increased mood changes. Suchmood changes may be irritability, depression<strong>and</strong> feelings of elation.High blood pressureHigh blood pressure may be caused by thetacrolimus/cyclosporin or prednisone. It this isINFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALa problem you may require treatment withantihypertensive medication or alteration in yourdrug dosage.PCP (Pneumocystis)This is a lung infection that doesn’t hurt healthypeople even though we are exposed to it all thetime. When the immune system is modified bydrugs, this infection can cause a serious <strong>for</strong>m ofpneumonia, especially in the first six monthsafter <strong>transplant</strong>. This is prevented by takingBactrim/Resprim three times a week <strong>for</strong> the firstyear following <strong>transplant</strong>ation.OsteoporosisBone mineral density can decrease during thefirst 3 months after <strong>transplant</strong>, due to the highdoses of immunosuppressant medicationrequired to prevent rejection. This ‘thinning ofthe bones’ may result in fracture, particularly inthe vertebrae (back-bones) or the ribs. OralCalcium <strong>and</strong> Vitamin D supplements are given toprevent this. Other treatments are also available<strong>for</strong> patients at higher risk.MRSA Infection (Golden Staph)MRSA is a bacterial infection that can beacquired in hospital. It is a bacteria that isresistant to a number of antibiotics. If you shouldhappen to acquire this infection while inhospital, you may be treated by an intravenousantibiotic (vancomycin). To stop the spread ofthis infection, you will be nursed in a single roomor in a ward with other patients who have thisinfection. Visitors will be asked to wear protectiveclothing.VREVRE st<strong>and</strong>s <strong>for</strong> Vancomycin ResistantEnterococcus. Enterococcus is a bacteria thatcan be found normally in the bowel. On rareoccassions it can go to other parts of the body<strong>and</strong> cause infection. Sometime VRE can befound in your body <strong>and</strong> not make you feel unwellor give you any signs or symptoms of infection.Most patients with VRE are colonised with thebacteria <strong>and</strong> do not have an infection. Patientswith VRE may be isolated from other patients toprevent the spread of bacteria.32Potential ongoing/long-term problemspost <strong>transplant</strong>Problems with Kidney functionRegular blood tests will monitor your kidneyfunction. Medication you are required to takefollowing your <strong>transplant</strong>, particularlytacrolimus/cyclosporin can cause deteriorationof your kidney function. Your renal function ismonitored in all your regular blood tests. The<strong>transplant</strong> team will adjust your medications tominimise the risk of kidney dysfunction. It is agood idea <strong>for</strong> you to maintain a good fluid intakeat all times, particularly in hot summer weatherto minimise any adverse effects your medicationregime may have on your kidney function.High cholesterol (hyperlipidaemia) <strong>and</strong>high blood pressureThese are common problems after <strong>transplant</strong>.Other risk factors, which may influence thedevelopment of hyperlipidaemia, include age,diabetes <strong>and</strong> obesity.Dietary reduction in calories <strong>and</strong> fat intake isrecommended, combined with exercise. Yourlipid (blood fat) levels will be monitored atregular intervals following your <strong>transplant</strong>. Yourblood pressure is also checked at each clinicvisit. Many patients require ongoing treatmentwith antihypertensive medication <strong>and</strong> yourdoctor may suggest the use of cholesterolloweringtherapy.Early recognition <strong>and</strong> treatment of high bloodpressure, control of hyperlipidemia, control ofobesity <strong>and</strong> good blood sugar control <strong>for</strong> diabeticpatients are important in preventing long-termcardiovascular problems, such as heartproblems or strokes.
THE LIVER TRANSPLANT UNITSECTION 18:OUTPATIENT VISITSFollowing discharge your progress will bemonitored in the Liver Transplant Clinic on 9 East.You will probably need to attend two to threetimes in the first week following discharge fromhospital, then once or twice a week <strong>for</strong> anotherweek or two, <strong>and</strong> then less frequently as timeprogresses. After one year from <strong>transplant</strong>ationmost patients will only be required to come <strong>for</strong>clinic visits every 3 months. However, lifelongfollow-up is necessary.Preparing <strong>for</strong> your outpatient visits:1. Check your medicine supply to seewhether you have enough medicationuntil your next visit. If not, remember toget a new prescription while at the clinic.2. Do not take your morning dose ofCyclosporin/Tacrolimus (Neoral) until afteryour blood has been taken.3. Bring your MEDICATION CARD, so that itcan be updated.4. If necessary, write down any questionsyou have so that you remember to askthem while at the clinic.Post-op surgical appointmentOn discharge, you will be given an appointmentcard to visit the surgeon around 6 weeks afteryour <strong>transplant</strong> operation. On the same day youwill have a Doppler Ultrasound of your <strong>liver</strong>per<strong>for</strong>med on Level 2 of the Missenden MedicalCentre, 54-60 Briggs Street, Camperdown(Tel. No. 9550-4733). This appointment will alsobe made prior to discharge.33INFORMATION MANUAL
THE LIVER TRANSPLANT UNITSECTION 19:FOLLOW-UP MEDICAL CAREthinning of the bones, or who require ongoinguse of signficant doses of prednisone. These areusually per<strong>for</strong>med every one to two years.INFORMATION MANUALDentist1. Routine dental care should bemaintained. However, gums may swellor bleed because of Cyclosporin therapy.2. You should make your dentist aware ofyour medications, particularly of yourCyclosporin regime.3. Cyclosporin may cause an overgrowth ofyour gums that will decrease when yourdosage is reduced.4. If you have your teeth cleaned or filledor require dental surgery, such as a toothextraction, or root canal work, you willneed to tell your dentist that you needantibiotics to prevent infection.OphthalmologistRoutine eye examinations are very importantbecause prednisone may cause a change inyour eyesight or blurry vision. You should alertyour eye doctor to all of your medications,especially your prednisone. It is recommendedthat you not change you glasses prescriptionuntil your doses of prednisone have stabilised.Pap smears <strong>and</strong> mammogramsWomen should continue to have second yearlypap smears <strong>and</strong> gynaecological examinations.Examine your breasts regularly, one week afteryour period <strong>and</strong> report to your doctor if anylumps develop. Mammograms should beper<strong>for</strong>med according to st<strong>and</strong>ardrecommendationsScreening <strong>for</strong> bowel cancerSome patients are at increased risk of bowelcancer after <strong>liver</strong> <strong>transplant</strong>ation. In particular,patients with a history of Primary SclerosingCholangitis, Inflammatory Bowel Disease,previous polyps or bowel cancer or a strongfamily history of bowel cancer should undergoregular colonoscopy after <strong>transplant</strong>.Monitoring <strong>for</strong> osteoporosisRegular bone density scans (DEXA) arerecommended <strong>for</strong> patients with a history of34
THE LIVER TRANSPLANT UNITSECTION 20: TRAVELThe major aim of <strong>transplant</strong>ation is to enable youto resume a normal or near-normal lifestyle. Thisincludes resuming work <strong>and</strong> enjoying leisureactivities.Many people want to take a holiday after theTransplant Team has given them clearance.This is both welcomed <strong>and</strong> encouraged.ALWAYSREMEMBER TOPLAN AHEAD.If you wish to travel, especially overseas or to aremote area, you need to make some extraplans. Check with the Transplant Team first,because there are special problems if you wantto travel in some countries.1. If travelling outside of Australia, you mustcarry a letter from your doctor detailingwhat medicine you are on, how much youare taking, <strong>and</strong> that the medicine is <strong>for</strong>your personal use.2. You must leave all medicine in its originalpackaging.3. Ensure you have enough supply ofmedications to last <strong>for</strong> the duration ofyour holiday. You should carry extra incase some are destroyed. If travellingoverseas, put some medications in yourluggage <strong>and</strong> carry spare stock in yourh<strong>and</strong> luggage. This is in case of loss ortheft of luggage.4. You should make a note of where localhospitals are in case of a problem <strong>and</strong>have a contact number <strong>for</strong> RPAH to givethem if you need to.5. NEVER travel with a depleted stock ofdrugs - this is both irresponsible <strong>and</strong>dangerous.6. You should travel overseas with some<strong>for</strong>m of travel insurance that covers you<strong>for</strong> illness associated with your <strong>transplant</strong><strong>and</strong> <strong>for</strong> other illnesses <strong>and</strong> accidents. Youmight find it very difficult, if notimpossible, to obtain insurance coverage<strong>for</strong> <strong>transplant</strong>-related conditions. Youshould be aware that overseas medicaltreatment can be very costly.7. Check with the doctors on the TransplantTeam be<strong>for</strong>e receiving any vaccinations.Transplant patients MUST NOT receivelive vaccines.35INFORMATION MANUAL
THE LIVER TRANSPLANT UNITSECTION 21: VACCINATIONSIf you are planning a holiday, please check withthe clinic about vaccinations.YOU MUST NOT RECEIVEANY LIVE VACCINES ATANY TIMELive vaccines:BCGYellow fever vaccineMMR (mumps, measles <strong>and</strong> rubella)vaccineVaricella-zoster virus vaccineSmallpoxOral polio (live) Sabin vaccineVaccines which you may have:Tetanus toxoidInactivated polio vaccine (IVP)Hepatitis B vaccineHepatitis A vaccineMeningococcal polysaccharide vaccineDiphtheriaInfluenzaPertussis (whooping cough)Pneumococcal vaccineCholera (in patients over 6 monthsof age)Typhoid (in patients over 12 monthsof age)If you come into contact with chicken pox orother viruses, notify the Transplant Teamimmediately.INFORMATION MANUALCheck with the doctors on the Transplant Teambe<strong>for</strong>e receiving any vaccinations.We recommend that all patients have an annual‘Flu Shot’. This can be obtained from your GP.Pneumococcal vaccine every 5 years may alsobe recommended <strong>for</strong> some patients.36
THE LIVER TRANSPLANT UNITSECTION 22: AFTER DISCHARGEThe whole purpose of your <strong>transplant</strong> is to returnyou to a normal lifestyle. There are very fewrestrictions. Here are some points to note thatmight answer some questions you have aboutyour new lifestyle.Activity <strong>and</strong> exerciseThis is very important in maintaining youroptimum health. It increases energy, reducesstress, aids sleep, improves digestion <strong>and</strong> helpsyour emotional <strong>and</strong> psychological stability.Build up your exercising gradually from walkingto more strenuous activities, such as running<strong>and</strong> cycling. Indoor/outdoor activities are limitedonly by threat of potential injury or limits ofphysical stamina. Swimming may be resumedafter about six months. Once you are dischargedyou are encouraged to return to your normalactivities. Your energy level will slowly increase.Each day you will find you can do more <strong>and</strong>more. Moderation is the key. You may take longwalks or walk up <strong>and</strong> down stairs.Muscle weakness is common in most <strong>liver</strong>diseases <strong>and</strong> it will be worse immediately after<strong>liver</strong> <strong>transplant</strong>ation. You should maintain aregular exercise program that is geared <strong>for</strong> yourindividual progress.Regular physical activity <strong>and</strong> exercise arenecessary post-<strong>liver</strong> <strong>transplant</strong> in order tomaintain normal weight, minimise thedestructive effects of prednisone on muscles<strong>and</strong> bones <strong>and</strong> to reverse pre-<strong>transplant</strong>deconditioning. It will also increase energy levels<strong>and</strong> fitness, reduce stress <strong>and</strong> help emotional<strong>and</strong> psychological wellbeing.You must maintain a regular exercise program,progressed specifically to your own individualneeds.Exercise - GuidelinesFrequency – daily - you should aim to exerciseon a daily basis.Intensity - light to moderate - you should still beable to talk whilst exercising.37Avoid strenuous activities particularly in theinitial stages post-<strong>transplant</strong>. These can beresumed once your energy levels <strong>and</strong> physicalstamina have improved.Duration - up to 45min of continuous exercise -15-20 mins if exercise is more strenuous.Initially you may need to exercise <strong>for</strong> shorterperiods several times a day until you build upstrength <strong>and</strong> endurance.Type - walking is recommended;Walking is an easy, effective <strong>and</strong> inexpensive<strong>for</strong>m of exercise, associated with very fewinjuries. Other safe <strong>for</strong>ms of exercise includeswimming <strong>and</strong> stationary cycling.Running/jogging/jumping <strong>and</strong> other high-impactactivities are not recommended due to theincreased risk <strong>and</strong> severity of injuries.Warm up/cool down;5 minutes of each is encouraged to help preventmuscle tears <strong>and</strong> unnecessary soreness withexercise. Gentle stretching is also encouragedprior to exercising.Sample of program progression:Week 1 walk 10minWeek 2 walk 15minWeek 3 walk 20minWeek 4 walk 30minWeek 5 walk 45min2 x day2 x day2 x day2 x day1 x day & thereafterRemember:i) start slowly & progress gradually;ii) a physiotherapist is available <strong>for</strong> furtheradvice.AlcoholPeople whose <strong>liver</strong> disease was caused byalcohol should never drink alcohol again.Alcohol should be avoided <strong>for</strong> the first year afteryour <strong>liver</strong> <strong>transplant</strong> under any circumstances.Alcohol is processed by the <strong>liver</strong> <strong>and</strong> mayproduce changes in your <strong>liver</strong> function tests.These changes can be confused with signs ofINFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALrejection or <strong>liver</strong> infection. Moderate alcoholconsumption may damage the new <strong>liver</strong>.If you wish, you may have an alcoholic beverageto celebrate special occasions. Please limit yourintake to one to two glasses of wine orchampagne or one to two glasses of beer.People whose <strong>liver</strong> disease was caused byalcohol, or people who have a history ofexcessive alcohol use that is thought to havecontributed to <strong>their</strong> <strong>liver</strong> disease, should notdrink again. This is sometimes a difficult task,<strong>and</strong> issues surrounding life-long abstinenceshould be explored prior to <strong>transplant</strong>. If you feelyou are having difficulties complying with thisrequirement following <strong>transplant</strong>, it is veryimportant you discuss these issues with your<strong>transplant</strong> doctor or nurse who will arrangeappropriate support.Birth controlThe choice to have children is an importantdecision that is influenced by a number offactors that should be discussed with yourpartner, <strong>transplant</strong> physician, generalpractitioner <strong>and</strong> obstetrician/gynaecologist.Medications you are taking may have an effecton a developing foetus, there<strong>for</strong>e it is unwise toembark on an unplanned pregnancy.Mycophenolate (Cellcept) is of particularconcern in pregnancy <strong>and</strong> should not be usedunless absolutely necessary. Women receivingMycophenolate who are of childbearing potentialmust use effective contraception be<strong>for</strong>e, during<strong>and</strong> <strong>for</strong> six weeks after receiving Mycophenolate.Female patients generally resume <strong>their</strong>menstrual cycle after <strong>liver</strong> <strong>transplant</strong>ation. Highdoseprednisone may stop the menstrual flow,but ovulation (the time when you are fertile) willcontinue. There<strong>for</strong>e, you may become pregnanteven though you are not yet having normalperiods, so birth control is necessary. Ask yourphysician <strong>for</strong> advice.Contact phone numbersIt is vitally important that you notify theTransplant Nurses on 9515 7263 or theReception Staff on 9515 7268 if you changeyour contact telephone number, eventemporarily. We sometimes need to notify you38urgently about blood test results <strong>and</strong> must havethe correct contact telephone numbers at alltimes. If you have an email address, you shouldensure we have it recorded.DietIf you are underweight, you need to gain weightto ensure that you have adequate nutritionalreserves <strong>for</strong> protection during any periods ofrejection or infection. Being overweightincreases the risk of developing other problems.Keeping your weight within an ideal range isthere<strong>for</strong>e most important. The dietitian will beable to discuss with you what your target weightshould be <strong>and</strong> how to attain it.DrivingAll States <strong>and</strong> Territories in Australia have lawsabout reporting health conditions that mightaffect a person’s ability to drive safely. Theselaws have been created to protect public safety.The laws require drivers to report to the DriverLicensing Authority any permanent or long-termillness that is likely to affect <strong>their</strong> ability to drivesafely.Your doctor or other members of the <strong>transplant</strong>team will not normally communicate directly withthe Driver Licensing Authority (RTA in NSW).However, your doctor will provide you withadvice about your ability to drive safely <strong>and</strong> canprovide a letter or report to take to the authority.The guidelines list a number of conditions thatdrivers MUST report to the Driver LicensingAuthority, if they wish to continue to hold adrivers license. These conditions include• If the person has chronic <strong>liver</strong> disease <strong>and</strong>clinical evidence of hepatic encephalopathy• If a person has had a <strong>liver</strong> <strong>transplant</strong>In both conditions, a conditional license may begranted. Further <strong>in<strong>for</strong>mation</strong> can be obtainedfrom the AUSTROADS website athttp://www.austroads.com.au.Most people can resume driving about six weeksafter the operation. Even if granted a conditionallicense, you should ask yourself the followingquestions be<strong>for</strong>e driving:
THE LIVER TRANSPLANT UNIT• Am I well enough to drive today?• Am I experiencing side-effects from mymedications that would interfere with my<strong>manual</strong> dexterity, such as severe tremors,blurry vision or light headedness?• Am I experiencing significant discom<strong>for</strong>taround my scar area that would stop mefrom being able to brake suddenly?Caution <strong>and</strong> restraint in this early post-operativeperiod will help assure your personal safety <strong>and</strong>the safety of others.Emotional issuesAlthough you will have been looking <strong>for</strong>ward tothe day when you leave the hospital, it is normalto feel slightly apprehensive <strong>and</strong> insecure. Thesefeelings usually only last a few days. Once yourealise that nothing awful is going to happenbecause you are not having your blood pressurechecked regularly, you will soon gain yourconfidence <strong>and</strong> independence.It may take time to adjust to your new healthyrole, not only in yourself <strong>and</strong> your capabilities,but also in your relationships with your family<strong>and</strong> friends. They too have to adjust to accepting<strong>and</strong> treating you as normal <strong>and</strong> healthy.At the same time, you may miss the constantattention you have received be<strong>for</strong>e <strong>and</strong>throughout your <strong>transplant</strong>. It is important toremember that family <strong>and</strong> friends have beenunder enormous pressure as well.Do not self-medicate with anymedication other than thoseprescribed by your doctor.LiftingYou may not lift anything that weighs more than7kg (15lbs) - about the weight of an average bagof groceries - <strong>for</strong> eight weeks after your surgery.Liver Support GroupThe Liver Support Group does valuable work <strong>for</strong><strong>liver</strong> patients. It also offers the chance <strong>for</strong> <strong>liver</strong><strong>recipients</strong> <strong>and</strong> <strong>their</strong> <strong>families</strong> to get togethersocially. Ask at the clinic <strong>for</strong> more <strong>in<strong>for</strong>mation</strong>or go to the websitehttp://www.<strong>liver</strong>supportgroup.org/.An Application Form to join the Liver SupportGroup can be found on the website <strong>and</strong> is alsoincluded in the back of this Manual. Pleasephotocopy it or tear it out if you want to join.Nursing care after dischargeWhen a patient goes home after a <strong>transplant</strong> it isvery rare <strong>for</strong> them to need full time nursing care.It may be necessary <strong>for</strong> a community nurse tovisit to do daily wound dressings. The nursingstaff will arrange this be<strong>for</strong>e you are discharged.Apart from that, you should be well enough to domost things, like showering <strong>and</strong> dressingyourself.Herbal remediesTransplant patients are advised not to take anyherbal remedies as abnormalities of LiverFunction Tests have been reported after use ofcertain herbal preparations, while the effects ofmany herbal preparations on the <strong>liver</strong> are notknown.There have been a number of rejection episodesreported in patient’s taking the herbalpreparation “St. John’s Wort”, which manypeople take <strong>for</strong> depression. Valerian is anotherpreparation which is known to causeabnormality in <strong>liver</strong> function tests.These preparations may interact with theabsorption or metabolism of yourimmunosuppressive medications,tacrolimus/cyclosporin <strong>and</strong> altering your bloodlevels.39School <strong>and</strong> workFollowing your <strong>transplant</strong> you should be able toreturn to your normal lifestyle. Most people areable to return to school or work. You will knowwhen you are ready <strong>for</strong> this. Going back to workpart-time, if possible, is a good way to build upyour stamina.You will be advised at the clinic about yourfitness <strong>for</strong> work. Individual circumstances willvary.Sexual activitySexual activity can be resumed as soon as youfeel able. It is a good <strong>for</strong>m of exercise! It maytake a while to regain confidence <strong>and</strong> your sexdrive, partly due to your medications <strong>and</strong> alsoyour previous feelings <strong>and</strong> attitudes fromINFORMATION MANUAL
THE LIVER TRANSPLANT UNITexperience of your illness. Please feel that youare able to discuss any concerns or worries withmembers of the Liver Transplant Team.Skin cancerThere is a much higher risk of skin canceramongst all <strong>transplant</strong> patients. There<strong>for</strong>e it ismost important to avoid sunlight <strong>for</strong> prolongedperiods of time. Wear long sleeves <strong>and</strong> a hat atall times when outdoors <strong>and</strong> avoid being out inthe sun between the hours of 11.00am to3.00pm daylight-saving time <strong>and</strong> 10.00am to2:00pm in Eastern St<strong>and</strong>ard Time. Apply SPF15or higher sun protection cream or lotion to anyexposed areas of the skin. If you are sittingoutdoors, you should sit in the shade.COMPLAINTS & FEEDBACKMaking a complaint will not affect your right toquality service <strong>and</strong> may help us to improve ourservice. If you feel there is difficulty in resolvingyour issue, please contact the PatientRepresentative on (02) 9515 5115. Positivefeedback is encouraged <strong>and</strong> welcomed.INFORMATION MANUALSportYou may wish to get involved in sport again. Ifyou do, do it gradually. Ask at the clinic <strong>for</strong> more<strong>in<strong>for</strong>mation</strong> about ‘come <strong>and</strong> try’ days withTransplant Australia (see below).Transplant AustraliaTransplant Australia activities include sports,social events, weekends away <strong>and</strong> fund raisingactivities. Transplant Australia organises theTransplant Games, held nationally <strong>and</strong>internationally. Phone: (02) 9531 2589 or visitwww.<strong>transplant</strong>.org.auREMEMBRANCE AND THANKSGIVINGSERVICE - RPAHThe Remembrance <strong>and</strong> Thanksgiving Service isheld annually at RPAH – usually in February.This service is held <strong>for</strong> anyone who has beentouched by organ donation or <strong>transplant</strong>.ANNUAL ECUMENICAL ORGAN DONORTHANKSGIVING & REMEMBRANCESERVICEThe Organ Donor Thanksgiving <strong>and</strong>Remembrance Service is held annually – usuallyin May. This service is held <strong>for</strong> anyone who hasbeen affected by organ donation or <strong>transplant</strong>.40
THE LIVER TRANSPLANT UNITSECTION 23:COMMON TESTS PERFORMED INPEOPLE WITH LIVER DISEASEOR AFTER TRANSPLANTUltrasound - This is the most commonly usedtechnique to get a picture of the <strong>liver</strong> <strong>and</strong> bileduct system. Ultrasound involves using atransducer or h<strong>and</strong>piece to generate soundwaves, which are bounced off the <strong>liver</strong> toproduct an image of it on a television screen.In this way, ultrasound can show how big the<strong>liver</strong> is <strong>and</strong> whether there are any changes,lumps or areas of abnormality. It also shows thesize of the bile ducts <strong>and</strong> whether they areblocked. If necessary, ultrasound can be usedto measure blood flow through the veins <strong>and</strong>arteries supplying the <strong>liver</strong> (doppler ultrasound).Ultrasound is done after six hours of fasting.It is an easy <strong>and</strong> painless test <strong>and</strong> does notinvolve x-rays.CT scan (Computed Tomography) - Inthis procedure, a series of x-rays are takenwhich a computer builds into a threedimensionalpicture of the area underinvestigation. The <strong>liver</strong>, blood vessels, gallbladder, bile ducts <strong>and</strong> nearby organs such asthe pancreas, spleen <strong>and</strong> kidneys can be seen,as can any cysts or tumours. It is usual to needto fast <strong>for</strong> 4 hours be<strong>for</strong>e the test. Just be<strong>for</strong>e thetest is per<strong>for</strong>med, you may be asked to drink aspecial liquid so that the stomach <strong>and</strong> intestinesare more easily identified. The radiologist mayinject a dye into the bloodstream to obtain aclearer picture of blood vessels. This dye maycause an allergic reaction in some people. If youknow you are allergic to iodine or contrast dye,you should notify your doctor. If your kidneys arenot functioning normally, your doctor maydecide to per<strong>for</strong>m the study without the injectionof dye. A CT scan takes about 45 minutes <strong>and</strong> isper<strong>for</strong>med lying down in a com<strong>for</strong>table position.Angiogram - This test is not required in allpatients. It involves passage of a fine catheterinto the artery in the groin, which is then passedinternally up to the artery supplying blood to the41<strong>liver</strong>. Contrast dye is injected through thecatheter <strong>and</strong> x-ray pictures are taken of theblood supply of the <strong>liver</strong>. In patients withsuspected or known <strong>liver</strong> cancer, this test maybe combined with a CT scan.MRI / MRCP (Magnetic ResonanceImaging) - MRI is another way of takingpictures of the <strong>liver</strong> <strong>and</strong> other internal organs,<strong>and</strong> does not involve x-rays. MRCP is a special<strong>for</strong>m of MRI that allows examination of the bileducts without insertion of any tubes or catheters.For an MRI scan, you have to lie on a narrowbed that slides inside a tunnel. People withclaustrophobia (fear of closed spaces) may findthis test difficult.ERCP (Endoscopic RetrogradeCholangio - Pancreatography) - This testis not required in all patients. It is a special test<strong>for</strong> examining the bile ducts. An endoscope ispassed down through the mouth <strong>and</strong> stomach<strong>and</strong> into the upper part of the small intestine.A special fluid that shows up on X-ray is theninjected into the opening of the main bile duct atthe point where it drains into the small intestine.The resulting x-ray picture is used to diagnosecertain diseases affecting the bile ducts.Additional procedures can be per<strong>for</strong>med at thesame time, such as removal of bile duct stones,or insertion of a plastic tube (stent) if bile flow isimpeded. ERCP may be associated withcomplications. You should discuss these riskswith your doctor.PTC (Percutaneous TranshepaticCholangiogram) - With the use of sedation orlocal anaesthetic, a small needle or catheter ispassed into the bile ducts through the skin <strong>and</strong><strong>liver</strong>. Pictures are taken of the bile ducts. Thisprocedure allows access to the <strong>liver</strong> so thatprocedures, such as treatment of bile ductnarrowing, can be per<strong>for</strong>med.Endoscopy - The inside of the oesophagus(gullet), stomach <strong>and</strong> upper small bowel can beexamined using a flexible telescope called an“endoscope”. This procedure is done using mildsedation injected into a vein <strong>and</strong> is usually notunpleasant. A similar device called a“colonoscope” is used <strong>for</strong> examining the largeINFORMATION MANUAL
THE LIVER TRANSPLANT UNITbowel via the anus. Endoscopy is commonlydone be<strong>for</strong>e <strong>transplant</strong>ation to check <strong>for</strong> thepresence of varices, ulcers <strong>and</strong> cancer of thegastrointestinal tract. Your doctor will discuss thespecific risks of an endoscopic procedure.Liver biopsyA <strong>liver</strong> biopsy involves collecting a small sampleof tissue the size of half a matchstick from your<strong>liver</strong> by passing a needle through the skin intoyour <strong>liver</strong>. The sample is then examined under amicroscope.It is an important way that your doctor c<strong>and</strong>etermine the cause of a <strong>liver</strong> problem, <strong>and</strong>assess the severity of any damage. Liver biopsyusually requires admission to hospital <strong>for</strong> theday, <strong>and</strong> is generally per<strong>for</strong>med by agastroenterology registrar or radiologist during anultrasound or CT scan. You lie flat on your backin bed as the doctor applies antiseptic to theskin over the right side of the rib cage then injecta local anaesthetic. The biopsy needle is thenpassed briefly through the skin <strong>and</strong> into the <strong>liver</strong>be<strong>for</strong>e being removed. The entire proceduretakes a few minutes <strong>and</strong> generally causes onlyminor discom<strong>for</strong>t. Liver biopsy may occasionallybe required prior to <strong>transplant</strong>, <strong>and</strong> is notuncommonly required after <strong>transplant</strong> if there isdeterioration of <strong>liver</strong> blood tests. The biopsy is acritical test <strong>for</strong> assessing rejection, hepatitis, orother causes of <strong>liver</strong> disease.INFORMATION MANUAL42
THE LIVER TRANSPLANT UNITAppendix A:GLOSSARYAcute: Occurring rapidly - commonly used by thepublic to convey seriousness or urgency. In medicalterminology it only refers to the time course of aproblem.Acute hepatitis: Acute inflammation of the <strong>liver</strong>which is usually due to viral infection.Albumin: One of the most important proteins madeby the <strong>liver</strong>. Low albumin levels in the blood usuallyindicate poor <strong>liver</strong> function.Auto-immune: Immunity misdirected against thebody instead of against an invading infection.Auto-immune hepatitis: A <strong>for</strong>m of chronichepatitis which occurs when the body’s immunesystem attacks its own <strong>liver</strong> cells.Autosomal recessive inheritance: Aninherited problem which occurs only when aparticular inherited gene is inherited from bothparents.Bile: Yellow-green fluid produced in the <strong>liver</strong> <strong>and</strong>stored in the gall bladder. Bile helps the body breakdown fats <strong>and</strong> digest fat-soluble vitamins.Alcoholic <strong>liver</strong> disease: Liver damage, causedby excessive consumption of alcohol, ranging fromtoo much fat in the <strong>liver</strong> to cirrhosis.Alpha-fetoprotein: A protein normally present inthe foetus but occurring in high levels in primary <strong>liver</strong>cancer.Alkaline phosphatase: An enzyme normallymade by bile duct cells. If the bile duct is blocked,the level of alkaline phosphate in the blood rises.Aminotransferase enzymes: Proteins thatoccur normally in <strong>liver</strong> cells which are released inincreased amounts into the bloodstream when cellsare damaged. Two of these enzymes - alanineaminotransferase (ALT) <strong>and</strong> aspartateaminotransferase (AST) - are commonly measured in<strong>liver</strong> function tests.Anaemia: A condition in which the blood isdeficient in red blood cells or oxygen-carryingproteins.Antibody: Part of the immune system that helps thebody fight infection <strong>and</strong> <strong>for</strong>eign substances.Antigen: A substance <strong>for</strong>eign to the body (usually aprotein) which causes the immune system toproduce antibodies.Anti-viral drugs: Drugs used to treat viralinfections including viral hepatitis, CMV <strong>and</strong> herpes.Ascites: Uncom<strong>for</strong>table accumulation of fluidcausing abdominal swelling. This occurs when theblood flow through the <strong>liver</strong> is obstructed. Ascitesoften occurs with cirrhosis of the <strong>liver</strong>. It may persist<strong>for</strong> some weeks after successful <strong>liver</strong> <strong>transplant</strong>.43Bile acids: Cholic <strong>and</strong> cheno deoxycholic acidsmade in the <strong>liver</strong> from cholesterol.Bile ducts: Tubes which carry bile from <strong>liver</strong> cellsto the gall bladder <strong>and</strong> duodenum.Bile salts: Sodium <strong>and</strong> potassium salts in bileacids. Produced in the <strong>liver</strong>, secreted into the bile<strong>and</strong> de<strong>liver</strong>ed to the intestine where they help thedigestion <strong>and</strong> absorption of fats.Biliary atresia: Congenital condition in which bilefrom the <strong>liver</strong> cannot reach the intestine because thebile ducts have developed poorly or not at all.Bilirubin: The breakdown product of old red bloodcells excreted by the <strong>liver</strong>. Bilirubin is normallyexcreted in bile. If this does not occur, theconcentration of bilirubin in the blood rises <strong>and</strong> leadsto jaundice.Blood pressure: The pressure of blood in thearteries. For blood to circulate through the body, thecirculatory system must be under pressure to <strong>for</strong>ceblood through the system. When blood pressure ismeasured, the higher number, called the “systolic”,refers to blood pressure when the heart iscontracting. The lower number, the “diastolic”, iswhen the heart muscle is relaxed.Blood products: A general term <strong>for</strong> differentcomponents of blood which can be transfused intopatients to replace various deficiencies.Bone marrow cells: The cells in the bone wherered & white cells <strong>and</strong> platelets are made.Cholestasis: Failure of bile to flow from the <strong>liver</strong>through the bile ducts.INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALChronic: Occurring over a long period of time. Thisterm does not refer to the severity of a process, onlyits duration.Chronic active hepatitis: Long-term <strong>liver</strong> injurydue to inflammation of the <strong>liver</strong>.Chronic viral hepatitis: Chronic infection of the<strong>liver</strong> due to the hepatitis viruses B <strong>and</strong> C.Cirrhosis: The end stage of chronic <strong>liver</strong> diseasefrom any cause. The <strong>liver</strong> is scarred <strong>and</strong> its functionmay be significantly impaired.Clotting factors/proteins: Substances mademainly in the <strong>liver</strong> to help the normal clotting ofblood. The ability of blood to clot is controlled by thepresence of clotting proteins. Most of these proteinsare made in the <strong>liver</strong> <strong>and</strong> exported into the blood.Declining <strong>liver</strong> function results in reduced clottingpower. Patients with <strong>liver</strong> disease often have bleedingproblems <strong>and</strong> lack of clotting factors is one of thereasons <strong>for</strong> this.Creatinine: A product of muscle metabolism that isexcreted by the kidneys. Creatinine level serves as avery good indicator of kidney function.Cross matching: A test of compatibility betweenthe potential donor’s <strong>and</strong> prospective recipient’sblood.Cytomegalovirus (CMV): A very common virusthat harmlessly infects many normal people. Itcauses lots of trouble in <strong>transplant</strong> patients becausethe drugs that prevent rejection of the <strong>liver</strong> allow thisvirus to be active. Virus activity can effect the <strong>liver</strong>,blood <strong>and</strong> eyes. It can be treated if necessary with adrug called Ganciclovir.Coma: A state of drowsiness followed by loss ofconsciousness. May occur in <strong>liver</strong> failure.Computer Assisted Tomography (CT scan):An X-ray technique using a computer reconstructionof multiple images of the body.Corticosteroids: Drugs used to suppressinflammation, such as prednisolone, prednisone orhydrocortisone.Cryptogenic: Literally means “unknown cause”.Some cases of <strong>liver</strong> cirrhosis have no known cause<strong>and</strong> are given the diagnosis “cryptogenic cirrhosis” to44distinguish them from other known causes ofcirrhosis such as alcoholic cirrhosis.Cyclosporin (Neoral): A very important drugwhich virtually all <strong>transplant</strong> patients now receive.Its function is to prevent rejection of the <strong>liver</strong> by thebody’s immune system.Cytotoxic: Damaging to cells, <strong>for</strong> example drugsused to destroy cancer cells.Defective virus: A virus which needs the help ofother viruses to grow, eg. hepatitis D.Dehydration: Loss of water from body cells.Diabetes mellitus: A condition of abnormalglucose metabolism. Blood glucose levels increasedue to the lack of or low effectiveness of the hormoneinsulin. Also affects the way the body uses proteins<strong>and</strong> fats.Donor <strong>liver</strong>: The <strong>liver</strong> provided to the recipientin a <strong>liver</strong> <strong>transplant</strong> operation.Donor: Someone who provides an organ <strong>for</strong><strong>transplant</strong>ation.Doppler Ultrasound: An easily per<strong>for</strong>med,painless test that is often per<strong>for</strong>med after <strong>liver</strong><strong>transplant</strong>ation <strong>and</strong> shows whether or not the bloodflow to <strong>and</strong> from the <strong>liver</strong> is normal.Duodenum: The first part of the small intestinejoins the stomach to the jejunum.Electrolytes: Minerals in solution in body fluids.The major electrolytes, sodium, potassium <strong>and</strong>chloride, influence the distribution of water in thebody. Magnesium <strong>and</strong> calcium are also electrolytes.Encephalopathy: Confusion or unconsciousnessthat can occur when someone has advanced <strong>liver</strong>failure or cirrhosis. It can be treated, but indicatesthat the <strong>liver</strong> disease is becoming severe.Endotracheal tube: An airway tube insertedthrough the mouth leading to your windpipe to helpyou breathe during surgery.ERCP: A special test <strong>for</strong> examining the bile ducts.An endoscope is passed down through the mouth<strong>and</strong> stomach <strong>and</strong> into the upper part of the smallintestine. Fluid that shows up on X-ray is then
THE LIVER TRANSPLANT UNITinjected into the opening of the main bile duct at thepoint where it drains into the small intestine. Theresulting X-ray picture is used to diagnose certaindiseases affecting the bile ducts.Fatty <strong>liver</strong>: Excessive deposit of fat in the <strong>liver</strong>.Fetor: A sweet smell on the breath of <strong>liver</strong> patientsthat results from an abnormal build up of certainchemicals in the blood.Fibrinogen: A protein factor important in bloodclotting.Fibrosis: Formation of excess fibrous (scar) tissuein an organ such as the <strong>liver</strong>.Flap: An uncontrollable jerking of the h<strong>and</strong>ssometimes seen in advanced <strong>liver</strong> disease. A flapindicates poor <strong>liver</strong> function.Foley catheter: A tube inserted into the bladder todrain urine.Gastroenterologist: A physician who specialisesin treating diseases of the digestive system <strong>and</strong> <strong>liver</strong>.Glucose: A type of sugar found in the blood.Graft: Your new <strong>liver</strong>.Haematemesis: Vomiting up of blood. May resultfrom bleeding from varices or a peptic ulcer (seebelow).Hepatitis: Acute inflammation of the <strong>liver</strong> oftencaused by viruses, drugs, alcohol or toxins.Hepatitis viruses: Viruses causing inflammationof the <strong>liver</strong>.Hepatocytes: Liver cells.Hepatologist: A physician who specialises in <strong>liver</strong>diseases.Immune system: The body’s natural systemdefending itself from viruses, infections or any <strong>for</strong>eignbody (such as a new organ).Immunosuppressives: Drugs used to reduce thebody’s defence mechanism, the immune system.These drugs keep the body from rejecting the<strong>transplant</strong>ed organ, but they also reduce the body’sability to fight off infection.Immunosuppressive medication: A drug thatsuppresses the body’s immune system. It helpsprevent the recipient’s own immune system fromattacking <strong>and</strong> rejecting the new <strong>liver</strong>.Imuran: Trade name <strong>for</strong> azathioprine (see above)Inflammation: The end result of the reaction of theimmune system to any <strong>for</strong>eign infection.Interferon: A protein produced by the immunesystem to fight viral infection. It is given as aninjection to treat chronic hepatitis C.Haemochromatosis: Deposition of excess iron inthe <strong>liver</strong>, skin, joints <strong>and</strong> pancreas. This is aninherited disease in which large amounts of iron aretransported from the intestine, accumulate in the<strong>liver</strong>, <strong>and</strong> cannot be processed normally. Iron buildup affects other areas of the body as well as the <strong>liver</strong>.Haemoglobin: The red pigment in blood cells thatcarries oxygen to the tissues.Hepatic: Referring to the <strong>liver</strong>.Hepatic artery: The artery which carries blood tothe <strong>liver</strong>. The portal vein is the other main source ofblood flow to the <strong>liver</strong>.Hepatic vein: The vein which drains blood fromthe <strong>liver</strong> towards the heart.45Intravenous (IV): The infusion of fluids, blood ordrugs into a vein.Jaundice: Yellow colour of the eyes <strong>and</strong> skin due toexcess bilirubin in the blood. Usually occurs becausethe <strong>liver</strong> fails to excrete bilirubin in the normalmanner due to <strong>liver</strong> failure or obstruction to bile flow.Lipids: Another term <strong>for</strong> fats.Liver: The largest organ inside the body with manyfunctions, including manufacturing proteins <strong>and</strong>blood clotting factors, excreting bilirubin <strong>and</strong> storingiron.Liver biopsy: The process of removing <strong>and</strong>inspecting a small sample of <strong>liver</strong>. A needle isinserted into the <strong>liver</strong> <strong>and</strong> a tiny piece removed tobe inspected under a microscope.INFORMATION MANUAL
THE LIVER TRANSPLANT UNITINFORMATION MANUALLiver cancer: Malignant cells in the <strong>liver</strong> whetherfrom a primary cancer (which originates in the <strong>liver</strong>),or, more commonly, a secondary cancer (whichspreads from somewhere else in the body). Primary<strong>liver</strong> cancer usually arises in a <strong>liver</strong> that is alreadydamaged through cirrhosis. Primary <strong>liver</strong> cancer mayalso be called hepatocellular carcinoma or hepatoma.Liver failure: Failure of the <strong>liver</strong> to carry out itsnormal function. May result in jaundice, ascites orcoma.Liver function tests (LFTs): Blood tests tomeasure the function of the <strong>liver</strong>. These are bloodtests that are ordered regularly by <strong>liver</strong> doctors. Theygive an indication of how well the <strong>liver</strong> is working <strong>and</strong>help sort out the type of problem that may bepresent. They are done daily immediately following<strong>transplant</strong>ation. Abnormalities can indicate rejection,infection, side effects from drugs <strong>and</strong> many otherthings. Experience is required to determine what theresults mean. Abnormal results do not necessarilyimply that a serious problem is present.Liver <strong>transplant</strong>ation: The surgical removal ofa diseased <strong>liver</strong> <strong>and</strong> its replacement by a donor <strong>liver</strong>.Noncompliance: Failure to take medicine asprescribed or follow the advice of medical <strong>and</strong>nursing staff.Obesity: Excess accumulation of body fat.Oedema: Swelling of the ankles <strong>and</strong> legs due to anabnormal collection of fluid in the body <strong>and</strong> adeficiency of the blood protein albumin (see above).This is an effect of chronic <strong>liver</strong> disease.Oesophagus: The tube between the mouth <strong>and</strong>stomach. Also known as the gullet.Osteoporosis: A decrease in the density of boneassociated with advanced <strong>liver</strong> disease <strong>and</strong> also withprolonged corticosteroid use. Bones with osteoporosisare more likely to fracture.Platelets: Cells in the blood that help the blood toclot. Numbers may fall in cirrhosis.Pneumonia: Inflammation of lung tissue (differentfrom bronchitis).Portal hypertension: High blood pressure in theportal venous system that carries blood from the46intestine, spleen <strong>and</strong> pancreas to the <strong>liver</strong>.Portal hypertension can result in ascites or bleeding.Portal vein: A large vein which carries the majorblood supply to the <strong>liver</strong> from the intestine. Carriesnutrients resulting from digestion of food.Prednisone: A steroid hormone taken by most<strong>transplant</strong> <strong>recipients</strong> to help prevent rejection.Prevalence: The number of people with a givendisease at a given time.Prophylaxis: The prevention of a problem. Forexample, antibiotics are often given to <strong>transplant</strong>patients in the first year after <strong>their</strong> operation toprevent Pneumocystis pneumonia - a complicationof the anti-rejection drugs.Red blood cells: Blood cells which carry oxygenattached to haemoglobin.Small intestine: Part of the gastrointestinal tractthat includes the duodenum, jejunum <strong>and</strong> ileum.The major site <strong>for</strong> digestion <strong>and</strong> absorption of food.Spider naevi: Small red skin spots with spideryprojections that indicate the presence of <strong>liver</strong> disease.Spleen: An organ which breaks down ageing bloodcells <strong>and</strong> is also an important part of the immunesystem.Tacrolimus (Prograf): Most commonimmunosuppressive drug used after <strong>liver</strong> <strong>transplant</strong>.Thrombosis: The <strong>for</strong>mation or presence of a bloodclot.Tissue typing: A blood test done to evaluate thecloseness of tissue match between organ donor <strong>and</strong>recipient (done be<strong>for</strong>e <strong>transplant</strong>).Transfusion: Giving blood or blood products (suchas platelets or plasma) through a vein.Triglyceride: A type of body fat or oil made up ofglycerol with three fatty acids attached. Triglyceridelevels in blood rise after a meal, falling again as thefat is used <strong>for</strong> energy or stored as body fat.A continuing high level may occur with high alcoholintake or diabetes.Vaccination: A technique to produce protectiveantibodies against an infection by exposing the
THE LIVER TRANSPLANT UNITimmune system to a vaccine made of living or deadorganisms.Valacyclovir (Valtrex): An anti-viral drug thatworks against the virus that causes cold sores.Valganciclovir (Valcyte): An anti-viral drug thatworks against a virus called CMV.Varices: Large veins in the oesophagus which maydevelop due to portal hypertension, <strong>and</strong> which placethe individual at significant risk of bleeding into theoesophagus or stomach.Viral hepatitis markers: Antigens <strong>and</strong>antibodies measured by laboratory tests to indicatethe presence or absence of viral infections that cause<strong>liver</strong> disease.White blood cells: Elements of blood that fightinfection.Wilson’s disease: A disease due to excessivestorage of copper in the <strong>liver</strong> <strong>and</strong> brain.47INFORMATION MANUAL
THE LIVER TRANSPLANT UNITAppendix B:ROYAL PRINCE ALFRED HOSPITALAUSTRALIAN NATIONAL LIVER TRANSPLANTATION UNITin association with the RPAH Department of Upper Gastrointestinal Surgery <strong>and</strong> the AW Morrow Gastroenterology <strong>and</strong> Liver CentreDirectors: Surgeons: Hepatologists:Prof GW McCaughan Dr PJ Gallagher Prof GW McCaughanDr MD Craw<strong>for</strong>d Dr DJ Verran A/Prof S StrasserDr MD Craw<strong>for</strong>dA/Prof D KooreyProf RDM AllenDr N ShackelDr H PleassDr D BowenDr D JosephDr Gokulan PavenDr C S<strong>and</strong>roussiDr M Stormon (Paed)Dr A Shun (Paed)Dr G Thomas (Paed)CONSENT FOR A LIVER TRANSPLANT OPERATION…………………………………………………………….. request that a <strong>liver</strong> <strong>transplant</strong> operation be per<strong>for</strong>medon me. The nature of the operation has been explained to me by Professor/Dr …………………………...I have been provided with a copy of the Patient In<strong>for</strong>mation Book on Liver <strong>transplant</strong>ation.The process of organ donor selection <strong>and</strong> retrieval has been explained to me. I am aware that the donor <strong>liver</strong>s maynot be entirely normal. Every ef<strong>for</strong>t is made to screen the donor <strong>for</strong> transmittable disorders. There can be noguarantee that the donor does not have such a disorder (including infection or cancer). Donor <strong>liver</strong>s can sometimes have fatty deposits or other abnormalities, which may not be recognised be<strong>for</strong>e implantation. These cancause slow initial function, <strong>and</strong> occasionally <strong>transplant</strong>ed <strong>liver</strong>s do not function adequately, leading to a need <strong>for</strong>re-<strong>transplant</strong>ation. I am aware that it is usual practice of the ANLTU to use organs from donors with primarytumours localised to the brain, as the risk of tumour transmission in these cases is extremely low.I am aware that in some circumstances I could be <strong>transplant</strong>ed only a portion of a donor <strong>liver</strong>, if the organ hasbeen thought suitable <strong>for</strong> a split procedure <strong>for</strong> use in a child as well as an c adult. I underst<strong>and</strong> that I may receivea <strong>liver</strong> from a donor after cardiac death <strong>and</strong> this is likely to have a slightly higher rate of initial non-function orlong term bile duct narrowings.The development of complications from the operation has been discussed with me. These include infection,bleeding, poor function <strong>and</strong> rejection of the <strong>liver</strong>.I underst<strong>and</strong> that <strong>liver</strong> <strong>transplant</strong>ation is a treatment <strong>for</strong> <strong>liver</strong> failure <strong>and</strong> not a cure <strong>and</strong> that I will need to takedrugs to suppress rejection indefinitely. These anti-rejection drugs have side affects specific <strong>for</strong> each drug <strong>and</strong>these have been explained to me. Patients treated long-term with these agents are at increased risk of infection <strong>and</strong>cancer development.I underst<strong>and</strong> there is a possibility (currently about 1 in 10) of death during the first year following the <strong>transplant</strong>operation. I am satisfied with the explanations regarding the risk of <strong>liver</strong> <strong>transplant</strong>ation that I have received.INFORMATION MANUALI have been in<strong>for</strong>med that the details of my <strong>liver</strong> disease <strong>and</strong> of my <strong>transplant</strong> procedure will be discussed withrelevant health professionals <strong>and</strong> that these details will be included on clinical databases run by the <strong>liver</strong><strong>transplant</strong> unit, which will be used <strong>for</strong> clinical audit <strong>and</strong> research purposes. I am also aware that tissue taken fromthe organ at the time of the operation <strong>for</strong> clinical management reasons may also be utilised <strong>for</strong> research.I underst<strong>and</strong> that signing this consent <strong>for</strong>m does not interfere with my legal rights in the event of negligence.SIGNED:………………………………………WITNESS:…………………………………….K:LIVER/LETTERHEADS/Ltx Consent Form_Jan09DATE:……………………Secretariat: Transplantation Services, Level 9 East, Royal Prince Alfred Hospital, Missenden Road, Camperdown NSW 2050Telephone: 02 9515 7275 Facsimile: 02 9515 3606Email: anltu@email.cs.nsw.gov.au http://www.anltu.com.au48
THE LIVER TRANSPLANT UNITAppendix C:CONTACT NUMBERSLiver Transplant Sisters:Monday to Friday - 8am-4.30pmSr Margaret Gleeson9515 7263 or 9515 6111 <strong>and</strong> page no 80883Email: Margaret.Gleeson@sswahs.nsw.gov.auSr Fiona Burrell9515 6408Email: Fiona Burrell@sswahs.nsw.gov.auSr Allison Hinckson9515 7801Email: Allison.Hinckson@sswahs.nsw.gov.auLiver Transplant Registrar:Gastroenterology Registrar:Monday to Friday – 8am-5pm. 9515 6111 <strong>and</strong> pageAfter hours <strong>and</strong> Weekends . 9515 6111 <strong>and</strong> pageChaplain 9515 6111Clinical Nurse ConsultantDietitiansSr Jennifer Watson (Theatre Sister)9515 7275 <strong>and</strong> page no 86542Ms Helen Vidot & Ms Joanne Heyman9515 8053Clinic appointments 9515 7268Liver TransplantMonday to FridayAdministration Centre 9515 7275Nurse Unit Manager 9515 7543PsychiatristDr Robert Gribble9515 6111 <strong>and</strong> page no 80135Psychologist Ms Suzanne Roche – 9515 7426Social Worker Through Switch on 9515 6111Transplant Coordinator:Claire Baker9515 7274Email: Claire.Baker@sswahs.nsw.gov.au49INFORMATION MANUAL
THE LIVER TRANSPLANT UNITAppendix D:Membership ApplicationName: __________________________________________Address: __________________________________________Phone:(Home)__________________________________________Please tick the appropriate box:(Work)__________________________________________Email: __________________________________________Yes, I would like to become a member, please find payment <strong>for</strong>membership.I would prefer not to become a member, however I would like to be keptin<strong>for</strong>med about the group.I would prefer not to become a member, please do not contact meagain.To enable us to produce a newsletter that is of both use <strong>and</strong> interest, please take a fewmoments to jot down some notes or questions that you may have;-INFORMATION MANUALMargaret McKinlayPresidentLiver Support Group4 Berowra RoadMount Colah NSW 207950
THE LIVER TRANSPLANT UNITThe Liver Support Group Inc was founded on the 10th 0f November 1992.It was established to aid <strong>transplant</strong>ations patients with emotional supportwhere possible.Over the past 11 years the group has grown to provide the following services.The goal of the group today is to;-• Provide peer support to <strong>liver</strong> patients <strong>and</strong> <strong>their</strong> <strong>families</strong>.• Demonstrate the quality of life that may be obtainable after a <strong>liver</strong> <strong>transplant</strong>.• Offering opportunities to talk <strong>and</strong> meet with others that have experienced what they are or will beexperiencing.• Offering support to carers <strong>and</strong> <strong>their</strong> <strong>families</strong>.• Providing some financial assistance.• Moral support.• Practical support – many members have valuable expertise in various fields.• Raising funds to aid research projects.• Heighten the community’s awareness of Transplantation within Australia.• Provide a regular Newsletter to keep people in<strong>for</strong>med, in<strong>for</strong>mal meetings, be it face to face or byphone or email.• The Liver Support Group Website is currently under construction <strong>and</strong> upon its completion will be asimple way <strong>for</strong> people to keep up to date <strong>and</strong> in contact with other people in the same position.How do we achieve this?• Through various fundraising activities, such as raffles <strong>and</strong> the monthly stall.• Provide a regular Newsletter to keep people in<strong>for</strong>med <strong>and</strong> in<strong>for</strong>mal meetings, be it face to face orby phone or email.• Canvass <strong>for</strong> Corporate sponsorship• Assist in patient education schemes/days.Cost of Membership.The cost of membership is $5.00 per family per calendar year, (1st January to 31st December).NOTE: to be able to vote within the group it is necessary to be a financial member. Membership <strong>for</strong>msshould be completed <strong>and</strong> cheques made to The Liver Support Group <strong>and</strong> <strong>for</strong>warded to the addressbelow.Contact Details.If you would like further <strong>in<strong>for</strong>mation</strong> on the group or becoming a member of the group, please contact:Margaret McKinlay – PresidentEmail:mailto:president@<strong>liver</strong>supportgroup.orgWeb:http://www.<strong>liver</strong>supportgroup.orgAll mail can be <strong>for</strong>warded to:The Liver Support Group4 Berowa RoadMt Colah, NSW 207951INFORMATION MANUAL
THE LIVER TRANSPLANT UNITAppendix E:Transplantation Research at Royal Prince Alfred HospitalThe RPA Transplant Institute was established in 2006 to <strong>for</strong>mally recognize the interdependence of bestclinical practice <strong>and</strong> clinically based research at all levels.The scope of our research interests at RPA is as varied <strong>and</strong> as broad as our multi-disciplinary careteam. Our central research theme is the provision of greater access to better <strong>and</strong> safer <strong>transplant</strong>ation,<strong>and</strong> revolves around the shortcomings of the following two truths about current clinical <strong>transplant</strong>practice:1. More people can benefit from <strong>transplant</strong>ation than we have kidneys or <strong>liver</strong>s to <strong>transplant</strong>.2. The success of <strong>transplant</strong>ation has been made possible by the combination of powerful drugs tocontrol <strong>transplant</strong> rejection <strong>and</strong> our sophisticated ability to diagnose <strong>and</strong> treat the problems causedby those drugs.Our MissionThe RPA Transplant Institute is the research heart of Transplantation Services at RPA. Our mission is toconduct high quality scientific <strong>and</strong> clinical research that will lead to cures <strong>for</strong> diseases <strong>and</strong> findsolutions to one of the key challenges facing <strong>transplant</strong>ation medicine, the need <strong>for</strong>immunosuppressant therapy <strong>and</strong> the side effects it brings.INFORMATION MANUALWe aim to advance the knowledge of <strong>transplant</strong> healthcare professionals <strong>and</strong> create treatments that willcontribute to prolonged, improved health <strong>for</strong> all <strong>transplant</strong> patients.Through the education of patients, physicians <strong>and</strong> the wider community we will create a greaterunderst<strong>and</strong>ing of <strong>transplant</strong>ation <strong>and</strong> the significance of <strong>transplant</strong>ation as a critical means ofprolonging life.How can you help?The RPA Transplant Institute has unparalleled clinical facilities <strong>and</strong> <strong>transplant</strong> results. Our challengingclinical service provides a stimulating environment <strong>for</strong> research. The endeavors of our productiveclinical <strong>and</strong> laboratory research team require ongoing financial or equivalent support. Also, it is vital thatwe continue to grow <strong>and</strong> improve. Your donation will help us to attract <strong>and</strong> train the best <strong>and</strong> mostenthusiastic young clinicians <strong>and</strong> scientists, just as we have done <strong>for</strong> the last 40 years.Please ask the clinic staff or your <strong>transplant</strong> doctor if you would like more <strong>in<strong>for</strong>mation</strong> about the RPATransplant Institute52
THE LIVER TRANSPLANT UNITProfessional WebsitesPlease note that some of these websites are international sites. Organ allocation is country specific.For <strong>in<strong>for</strong>mation</strong> on organ allocation in Australia please talk to your doctor or the Transplant Coordinator.A. Liver TransplantationLiver Transplantation: Medline Pluswww.nlm.nih.gov/medlineplus/<strong>liver</strong><strong>transplant</strong>ation.htmlAustralia <strong>and</strong> New Zeal<strong>and</strong> Liver Transplant Registrywww.anzltr.orgDigestive Diseases: Liver Transplantation – Medicine Netwww.medicinenet.com/<strong>liver</strong>_<strong>transplant</strong>/article.htmB. Liver DiseaseAustralian Liver Foundationwww.<strong>liver</strong>.org.auLove Your Liverwww.loveyour<strong>liver</strong>.org.ukAmerican Liver Foundationwww.<strong>liver</strong>foundation.orgHealth Insitewww.healthinsite.gov.au/topics/Liver_DiseasesCanadian Liver Foundationwww.<strong>liver</strong>.caChildren’s Liver Disease Foundationwww.child<strong>liver</strong>disease.org53INFORMATION MANUAL
THE LIVER TRANSPLANT UNITNotesINFORMATION MANUAL54
Missenden Road, CamperdownHospital Phone: 02 9515 6111AUSTRALIAN NATIONAL LIVERTRANSPLANTATION UNITAVS 69069