Emergency Medical Fillable Form (pdf) - Albion Central School District
Emergency Medical Fillable Form (pdf) - Albion Central School District
Emergency Medical Fillable Form (pdf) - Albion Central School District

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
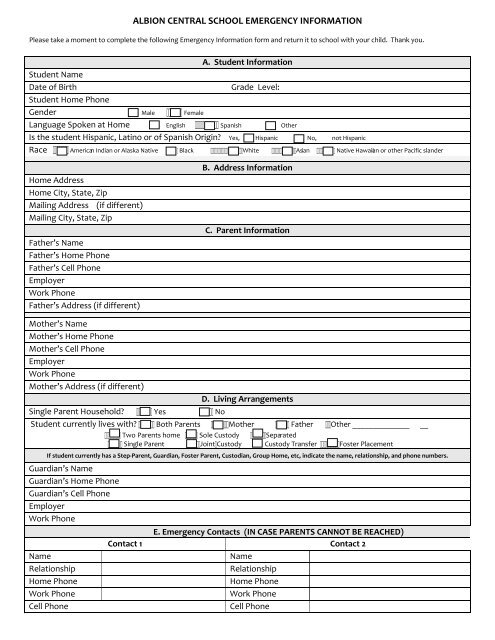
ALBION CENTRAL SCHOOL EMERGENCY INFORMATIONPlease take a moment to complete the following <strong>Emergency</strong> Information form and return it to school with your child. Thank you.A. Student InformationStudent NameDate of BirthGrade Level:Student Home PhoneGender Male FemaleLanguage Spoken at Home English Spanish OtherIs the student Hispanic, Latino or of Spanish Origin? Yes, Hispanic No, not HispanicRace American Indian or Alaska Native Black White Asian Native Hawaiian or other Pacific slanderHome AddressHome City, State, ZipMailing Address (if different)Mailing City, State, ZipFather’s NameFather’s Home PhoneFather’s Cell PhoneEmployerWork PhoneFather’s Address (if different)B. Address InformationC. Parent InformationMother’s NameMother’s Home PhoneMother’s Cell PhoneEmployerWork PhoneMother’s Address (if different)D. Living ArrangementsSingle Parent Household? Yes NoStudent currently lives with? Both Parents Mother Father Other ______________ __ Two Parents home Sole Custody Separated Single Parent JointCustody Custody Transfer Foster PlacementIf student currently has a Step‐Parent, Guardian, Foster Parent, Custodian, Group Home, etc, indicate the name, relationship, and phone numbers.Guardian’s NameGuardian’s Home PhoneGuardian’s Cell PhoneEmployerWork PhoneE. <strong>Emergency</strong> Contacts (IN CASE PARENTS CANNOT BE REACHED)Contact 1 Contact 2NameNameRelationshipRelationshipHome PhoneHome PhoneWork PhoneWork PhoneCell PhoneCell Phone
Doctor NameDoctor Phone NumberHospital of ChoiceDentist NameDentist Phone NumberF. <strong>Medical</strong> InformationAllergiesDoes student use an Epi‐Pen?Medications? (Please List)Health Problems – all existingmedical conditions.AsthmaDiabetesHearingFrequent Infections,HearingAids, orTubes‐Seizures‐Vision – Contacts/Glasses‐Other (Describe)Has any health condition resulted ina medical emergency?G. To Be Completed by the Parent/GuardianIn case of a medical emergency, and I can not be reached, I give my child’s doctor or any attending physicianpermission to administer medical treatment.Yes NoList ALL siblings living in the household. (Please include children not yet enrolled in school)BROTHER/SISTER DATE OF BIRTH MALE/FEMALE GRADEWould you like to receive district and school updates through email? Yes NoEmail address: _______________ _________________________________________________________________________________________________________________(signature of Parent/Guardian)_____________________(Date)If there is additional information about the health and welfare of your child of which the school needs to beaware, please contact the school office directly (589‐2050).