Adaptive Bayesian Designs in Dose-finding Studies
Adaptive Bayesian Designs in Dose-finding Studies
Adaptive Bayesian Designs in Dose-finding Studies

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Adaptive</strong> <strong>Bayesian</strong> <strong>Designs</strong> <strong>in</strong><strong>Dose</strong>-f<strong>in</strong>d<strong>in</strong>g <strong>Studies</strong>VICC Cancer Biostatistics Workshop Series2008Leena Choi, Ph.D.Department of BiostatisticsVanderbilt University School of Medic<strong>in</strong>eMay 16, 2008
Thomas Bayes – Bayes’ Theorem
Diagnostic Test<strong>in</strong>g• A woman at age 40 had a positivemammography <strong>in</strong> a rout<strong>in</strong>e screen<strong>in</strong>g• What is the probability that she actuallyhas breast cancer?An Intuitive Explanation of <strong>Bayesian</strong> Reason<strong>in</strong>g ©2003 byEliezer S. Yudkowsky.
Diagnostic Test<strong>in</strong>g• “The probability that a woman with apositive mammography has breastcancer”• “The probability that a woman with breastcancer has a positive mammography”An Intuitive Explanation of <strong>Bayesian</strong> Reason<strong>in</strong>g ©2003 byEliezer S. Yudkowsky.
Diagnostic Test<strong>in</strong>g• “The probability that a woman with a positivemammography has breast cancer”• “The probability that a woman with breast cancer has apositive mammography”• 3 pieces of <strong>in</strong>formation– the prior probability that a woman has breast cancer(prevalence)– the probability that a woman with breast cancer gets a positivemammography (sensitivity)– the probability that a woman without breast cancer gets apositive mammography (1-specificity)An Intuitive Explanation of <strong>Bayesian</strong> Reason<strong>in</strong>g ©2003 byEliezer S. Yudkowsky.
Diagnostic Test<strong>in</strong>g• Prevalence: 1% of women at age forty whoparticipate <strong>in</strong> rout<strong>in</strong>e screen<strong>in</strong>g have breastcancer• Sensitivity: 80% of women with breast cancerwill get positive mammographies• 1- specificity: 10% of women without breastcancer will also get positive mammographies• What is the probability that she actually hasbreast cancer?An Intuitive Explanation of <strong>Bayesian</strong> Reason<strong>in</strong>g ©2003 byEliezer S. Yudkowsky.
Diagnostic Test<strong>in</strong>g• 100 out of 10,000 women at age forty who participate <strong>in</strong> rout<strong>in</strong>escreen<strong>in</strong>g have breast cancer• Before the mammography screen<strong>in</strong>g:– Breast Cancer• 100 women +• 9,900 women -• After the mammography:– 100 women +• Group A: 80 women with breast cancer, and a positive mammography.• Group B: 20 women with breast cancer, and a negative mammography.– 9,900 women -• Group C: 990 women without breast cancer, and a positive mammography.• Group D: 8,910 women without breast cancer, and a negativemammography.• A/(A + C) = 80 / (80 + 990) = 80 / 1070 = 7.5%An Intuitive Explanation of <strong>Bayesian</strong> Reason<strong>in</strong>g ©2003 byEliezer S. Yudkowsky.
Bayes’ RuleP [cancer| T (+)]P[cancer] × P[T (+) | cancer]=P[cancer] × P[T (+) | cancer] + P[~ cancer] × P[T (+)| ~ cancer]0.01 × 0.8= = 7.5%0.01 × 0.8 + (1-0.01) × (1-0.9)
Bayes’ RuleP [cancer| T (+)]=P[cancer] × P[T (+) | cancer]P[cancer] × P[T (+) | cancer] + P[~ cancer] × P[T (+)| ~ cancer]• prior probability - the orig<strong>in</strong>al proportion ofpatients with breast cancer.• posterior probability - the estimated probabilitythat a patient has breast cancer, given that weknow she has a positive result on hermammography - is known as the revisedprobability• Prior × Data Posterior
Bayes’ RuleP [cancer| T (+)]=P[cancer] × P[T (+) | cancer]P[cancer] × P[T (+) | cancer] + P[~ cancer] × P[T (+)| ~ cancer]• Posterior belief <strong>in</strong> H (hypothesis, cancer) given the data∝Prior belief <strong>in</strong> H × support for H by the data– The probability of H before the data (prior)– The likelihood of the data given H (likelihood)– The probability of H given the data (posterior)• Posterior is a synthesis of Prior and Data us<strong>in</strong>g Bayes’ rule
Prior, Likelihood and Posterior• Prior distribution: represents the prior<strong>in</strong>formation associated with parameter– Information available <strong>in</strong> literature, cl<strong>in</strong>ical data base,expert op<strong>in</strong>ion, or any other appropriate source– Non-<strong>in</strong>formative represent<strong>in</strong>g very little or norelevant <strong>in</strong>formation• Data distribution (Likelihood)• Posterior distribution: updat<strong>in</strong>g the prior withthe likelihood, formally done via Bayes’theorem– Prior is merged with the likelihood to give a f<strong>in</strong>alposterior
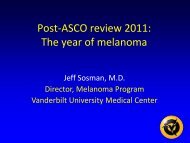
Example: Placenta Previa• The proportion of female births <strong>in</strong> the generalpopulation = 0.485 (female births < male births)• 437 out of total 980 births <strong>in</strong> placenta previa(437/980=0.446) were females <strong>in</strong> GermanThe sex of placenta previa births:Female 437 (0.446)--------------------------------------------Male 543 (0.554)Total 980 (1.0)Hypothesis:the proportion of placentaprevia female births is lessthan 0.485
0.485Prior0.30 0.35 0.40 0.45 0.50 0.55 0.60thetaLikelihood0.4850.30 0.35 0.40 0.45 0.50 0.55 0.60theta0.485Posterior0.30 0.35 0.40 0.45 0.50 0.55 0.60theta
0.485Posterior distribution0.30 0.35 0.40 0.45 0.50 0.55 0.6095% credible <strong>in</strong>tervalstheta[.425, .475]
Why <strong>Bayesian</strong> <strong>Adaptive</strong> <strong>Designs</strong>?• Update beliefs <strong>in</strong> light of new evidence• <strong>Dose</strong> f<strong>in</strong>d<strong>in</strong>g (dose dropp<strong>in</strong>g)• Stopp<strong>in</strong>g early, or late– Efficacy– Futility• Seamless phases• Add arms or drop arms• <strong>Adaptive</strong> randomization• Advantages– smaller trials (usually)– More precise conclusions, earlier decision– Increase the probabilities of success (faster, better drug development,reduce cost)– Better treatment of patients (right drug to right patient at right time)
Challenges <strong>in</strong> <strong>Bayesian</strong> Approach• Need appropriate priors – def<strong>in</strong>e what weknow based on external evidence(conclusions may depend priors )• Def<strong>in</strong>e complexity of our models – whatlikelihood to use• Require good knowledge of probabilitytheory• Computational challenge
<strong>Dose</strong> F<strong>in</strong>d<strong>in</strong>g <strong>Studies</strong>Garrett-Mayer E. Cl<strong>in</strong> Trials 2006• Oncology compounds are cytotoxic: the rational <strong>in</strong> cancerdose-f<strong>in</strong>d<strong>in</strong>g trials: to f<strong>in</strong>d the highest dose that is also safefor use <strong>in</strong> a Phase II trial• Maximum Tolerated <strong>Dose</strong> (MTD): “optimal” dose, “target”,relatively high dose with manageable side effects• <strong>Dose</strong>-limit<strong>in</strong>g toxicities (DLTs): 1 if toxicity occurs, 0otherwise• Standard “3+3” dose escalation design starts at dose k withfixed number of ordered dose levelsLevel k-1 k k+1 k+2 k+3 k+4<strong>Dose</strong> 100 mg 200 mg 400 mg 600 mg 800 mg 1000 mg• MTD def<strong>in</strong>ed as the highest dose at which 0 or 1 DLTs areobserved <strong>in</strong> 6 patients• If de-escalation occurs at the first dose level, the study isdiscont<strong>in</strong>ued
<strong>Dose</strong> F<strong>in</strong>d<strong>in</strong>g <strong>Studies</strong>:Traditional “3 + 3” dose escalation designsTreat 3 patients at dose kGarrett-Mayer E. Cl<strong>in</strong> Trials 20060 DLTs 1 DLTs > 1 DLTsEscalate to dose k+1:Return to top offlow chart with dose k+1Treat 3 morePatients at dose k1 DLTs outof 6 patients>1 DLTs outof 6 patientsIf 6 patients alreadytreated at dose k-1De-escalate todose k-1If 3 patientsalready treatedat dose k-1DLT: dose-limit<strong>in</strong>g toxicityEscalate to dose k+1:Return to top offlow chart with dose k+1StopStudyTreat 3 morePatients atdose k-1
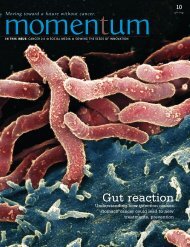
<strong>Bayesian</strong> <strong>Dose</strong>-f<strong>in</strong>d<strong>in</strong>g MethodCont<strong>in</strong>ual Reassessment Method• Cont<strong>in</strong>ual Reassessment methoda priori dose-toxicity(CRM) developed by O’Quigleyet al. (1990): a <strong>Bayesian</strong> Phase Idesign to estimate MTD• Assumption: probabilities of bothefficacy and toxicity <strong>in</strong>creasewith <strong>in</strong>creas<strong>in</strong>g dose• Use dose-toxicity relationship(dose-efficacy relationship fornon-cytotoxic): have rough ideaat least– Starts with a priori dosetarget DLT rate = 0.3response curve: parameterschosen based on <strong>in</strong>vestigators’prior belief– As data accumulate, the curvecompletely determ<strong>in</strong>ed by thedata, little like the a priori curve 1 2 3 4 5 6Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0<strong>Dose</strong> Leval
<strong>Bayesian</strong> <strong>Dose</strong>-f<strong>in</strong>d<strong>in</strong>g MethodCont<strong>in</strong>ual Reassessment Method• Advantages:– Superior to traditional dose-escalationdesigns because it “learns” form<strong>in</strong>formation ga<strong>in</strong>ed at early time po<strong>in</strong>ts– Less likely to treat patients at toxicdoses, more likely to treat patients atefficacious doses – more ethical– Shown that CRM-based designs to bemore efficient and safer (MTD is moreprecise, fewer cases of DLT – willshow comparison• Criticism:– a priori curve could be dangerous dueto large uncerta<strong>in</strong>ty– Large dose escalation could occurbased on little <strong>in</strong>formation– Practical issue: duration of time forcompletion of study (orig<strong>in</strong>al CRMevaluate every patient)• Modified CRMsProbability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0a priori dose-toxicitytarget DLT rate = 0.31 2 3 4 5 6<strong>Dose</strong> Leval
Modified CRMFraries, Goodman et al., Möller• Pre-def<strong>in</strong>ed dose levels forescalation as if for a “3+3”design• Always start at the lowestdose level under consideration• Any given dose escalationcannot <strong>in</strong>crease by more thanone level, although dose deescalationcan be large• Enrol two or three patients ateach prescribed cohort (notone)• Proceed as a standard doseescalation design <strong>in</strong> theabsence of dose-limit<strong>in</strong>gtoxicitiesProbability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0target DLT rate = 0.3a priori dose-toxicity1 2 3 4 5 6<strong>Dose</strong> Leval
<strong>Bayesian</strong> <strong>Dose</strong>-f<strong>in</strong>d<strong>in</strong>g MethodCont<strong>in</strong>ual Reassessment Method• Choice of dose level: practicalconsideration of preparation andpackag<strong>in</strong>ga priori dose-toxicity• Target rate of toxicity (or response)– Chemotherapy given short time period:serious side effects, often set 0.2 – 0.3(efficacy 0.8)– Choice not from statistician or s<strong>in</strong>gle<strong>in</strong>vestigator, consultations with colleagues –dramatic difference, beneficial• Choose a priori dose-toxicity curve– Visual display: clear understand<strong>in</strong>g of theimplications of various choices– One-parameter or two parameter models:hyperbolic tangent, one- or two-parameterlogistic models– CRM robust <strong>in</strong> choos<strong>in</strong>g MTD even if themodel is <strong>in</strong>correct– Good choice of model <strong>in</strong>crease efficiency(smaller size of trial)– Informative: Pass through doses for highDLT (eg, 90%) and low DLT (eg, 5%)Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0target DLT rate = 0.31 2 3 4 5 6<strong>Dose</strong> Leval
A priori dose-toxicity curvetarget DLT rate = 0.3DLT=1DLT=00.0 0.2 0.4 0.6 0.8 1.01 2 3 4 5 6<strong>Dose</strong> LevalProbability of Toxicity
A priori dose-toxicity curvenon-<strong>in</strong>formative<strong>in</strong>formativeProbability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0target DLT rate = 0.3Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0target DLT rate = 0.250.050.850 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)
<strong>Bayesian</strong> <strong>Dose</strong>-f<strong>in</strong>d<strong>in</strong>g MethodCont<strong>in</strong>ual Reassessment Method• Number of patients per dose level (cohort size)– 2-3 /cohort– Logistical issues: how long, accrual rate, total numberof patients available, maximum number of patients,number of dose levels, seriousness of DLT, etc.• Stopp<strong>in</strong>g and sample size: fixed number ofpatients (cont<strong>in</strong>ue until total sample size reachedfor cont<strong>in</strong>uous dose levels, <strong>in</strong>fusion), fixednumber of patients/dose (6-8 treated at the MTDfor discrete dose)
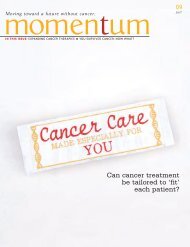
Example: A priori curve dose-toxicitywith until first DLT observedCohort <strong>Dose</strong> Outcomes (0 if no DLT, 1 if DLT)Garrett-Mayer E. Cl<strong>in</strong> Trials 20061 50 mg 0 02 100 mg 0 03 200 mg 0 0350 mg4 400 mg 0 1450 mg500 mg550 mg5 800 mg• Cohort size = 2• <strong>Dose</strong> levels: 50 – 800 by50 mg• DLT rate = 0.25• A priori curve: twoparameter logistic model• Stopp<strong>in</strong>g rule: 10patients treated at thesame doseProbability of Toxicity0.0 0.2 0.4 0.6 0.8 1.00.85target DLT rate = 0.250.050 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)
Probability of ToxicityDataCRM Cohort 4 Cohort 5target DLT rate = 0.250.05Prior0.85Posterior0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)<strong>Dose</strong> (mg)Cohort 6 Cohort 7 Cohort 80.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0 50 100 200 300 400 500 600 700 8000 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)<strong>Dose</strong> (mg)0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.00 50 100 200 300 400 500 600 700 8000 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)
Probability of ToxicityCohort 9 Cohort 10Cohort 110 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)Cohort 12 Cohort 13 Cohort 140.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.00 50 100 200 300 400 500 600 700 800 0 50 100 200 300 400 500 600 700 800<strong>Dose</strong> (mg)95% CI = [0.1, 0.47]<strong>Dose</strong> (mg)MTD
Accrual of DataCohort<strong>Dose</strong> Outcomes (0 if no DLT, 1 if DLT)CRMMTD1 50 0 02 100 0 03 200 0 04 400 0 15 350 0 06 400 0 07 550 1 08 450 0 09 500 0 010 550 1 111 450 0 112 450 0 013 450 1 014 450 0 015 450 STOPStopp<strong>in</strong>g rule: 10 patients treated at the same dose
Comparison of CRM and “3+3” <strong>Designs</strong>us<strong>in</strong>g Simulations Garrett-Mayer E. Cl<strong>in</strong> Trials 2006CRM I CRM II CRM III “3+3” I “3+3” II “3+3” III1 Total sample size 30 50 60 27 27 392 Patients per cohort 3 5 3 3 3 33 Number of cohorts 10 10 20 9 9 13Probability of Toxicity0.0 0.2 0.4 0.6 0.8 1.0target DLT rate = 0.30.1A priori0.9True curve“3+3” I“3+3” II“3+3” III0 400 800 1200 1600 2000 2400 2800 3200 3600 4000 4400 4800<strong>Dose</strong> (mg)True MTD = 1656 mg
Comparison of CRM and “3+3” <strong>Designs</strong>us<strong>in</strong>g Simulations Garrett-Mayer E. Cl<strong>in</strong> Trials 2006CRM I CRM II CRM III “3+3” I “3+3” II “3+3” III4 % of trials with recommend. dosewith<strong>in</strong> 250 mg of true (1656 mg)5 % of trials with recommend. dosewith<strong>in</strong> 400 mg of true (1656 mg)6 % of trials with recommend. dose DLTrate > 40%7 % of trials with recommend. dose DLTrate > 50%8 % of trials with recommend. dose DLTrate < 20%9 % of trials with recommend. dose DLTrate < 10%10 Average % of patients treated at doseswith 40% or greater DLT rate11 Average % of patients treated at doseswith 20% or less DLT rate12 Average % of patients treated at doseswith DLT rate57% 72% 71% 41% 35% 32%80% 91% 89% 41% 54% 58%9.5% 5.8% 5.9% 7.1% 21% 12%0.9% 0.2% 0.6% 7.1% 2.0% 0.6%13% 5.7% 6.2% 52% 44% 38%0.0% 0.1% 0.0% 11% 16% 6.9%7.6% 7.8% 5.7% 17% 23% 7.5%32% 19% 24% 62% 53% 64%26% 28% 26% 21% 22% 19%
Discussions• Real collaboration between cl<strong>in</strong>ician andstatistician– Cl<strong>in</strong>ician: dose levels, DLT rate, range ofsample sizes, accrual rate– Statistician: cohort size, stopp<strong>in</strong>g rule– Together: dose-response curve