1 Drug interactions in an elderly patient with significant polypharmacy
1 Drug interactions in an elderly patient with significant polypharmacy
1 Drug interactions in an elderly patient with significant polypharmacy

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
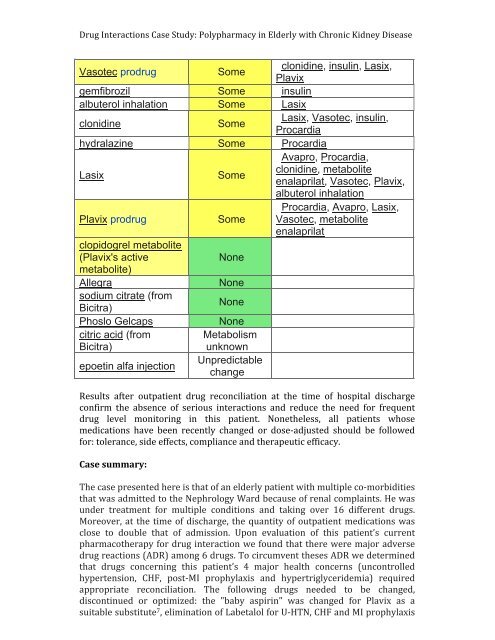
10 <strong>Drug</strong> Interactions Case Study: Polypharmacy <strong>in</strong> Elderly <strong>with</strong> Chronic Kidney Disease Vasotec prodrugSomeclonid<strong>in</strong>e, <strong>in</strong>sul<strong>in</strong>, Lasix,Plavixgemfibrozil Some <strong>in</strong>sul<strong>in</strong>albuterol <strong>in</strong>halation Some Lasixclonid<strong>in</strong>eSomeLasix, Vasotec, <strong>in</strong>sul<strong>in</strong>,Procardiahydralaz<strong>in</strong>e Some ProcardiaLasixSomeAvapro, Procardia,clonid<strong>in</strong>e, metaboliteenalaprilat, Vasotec, Plavix,albuterol <strong>in</strong>halationPlavix prodrugSomeProcardia, Avapro, Lasix,Vasotec, metaboliteenalaprilatclopidogrel metabolite(Plavix's activeNonemetabolite)AllegraNonesodium citrate (fromBicitra)NonePhoslo Gelcapscitric acid (fromBicitra)epoet<strong>in</strong> alfa <strong>in</strong>jectionNoneMetabolismunknownUnpredictablech<strong>an</strong>geResults after out<strong>patient</strong> drug reconciliation at the time of hospital discharge confirm the absence of serious <strong><strong>in</strong>teractions</strong> <strong>an</strong>d reduce the need for frequent drug level monitor<strong>in</strong>g <strong>in</strong> this <strong>patient</strong>. Nonetheless, all <strong>patient</strong>s whose medications have been recently ch<strong>an</strong>ged or dose-‐adjusted should be followed for: toler<strong>an</strong>ce, side effects, compli<strong>an</strong>ce <strong>an</strong>d therapeutic efficacy. Case summary: The case presented here is that of <strong>an</strong> <strong>elderly</strong> <strong>patient</strong> <strong>with</strong> multiple co-‐morbidities that was admitted to the Nephrology Ward because of renal compla<strong>in</strong>ts. He was under treatment for multiple conditions <strong>an</strong>d tak<strong>in</strong>g over 16 different drugs. Moreover, at the time of discharge, the qu<strong>an</strong>tity of out<strong>patient</strong> medications was close to double that of admission. Upon evaluation of this <strong>patient</strong>’s current pharmacotherapy for drug <strong>in</strong>teraction we found that there were major adverse drug reactions (ADR) among 6 drugs. To circumvent theses ADR we determ<strong>in</strong>ed that drugs concern<strong>in</strong>g this <strong>patient</strong>’s 4 major health concerns (uncontrolled hypertension, CHF, post-‐MI prophylaxis <strong>an</strong>d hypertriglyceridemia) required appropriate reconciliation. The follow<strong>in</strong>g drugs needed to be ch<strong>an</strong>ged, discont<strong>in</strong>ued or optimized: the "baby aspir<strong>in</strong>" was ch<strong>an</strong>ged for Plavix as a suitable substitute 7 , elim<strong>in</strong>ation of Labetalol for U-‐HTN, CHF <strong>an</strong>d MI prophylaxis