

Recent Advances in Follicular Variant of Papillary Thyroid Carcinoma
Recent Advances in Follicular Variant of Papillary Thyroid Carcinoma
Recent Advances in Follicular Variant of Papillary Thyroid Carcinoma

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
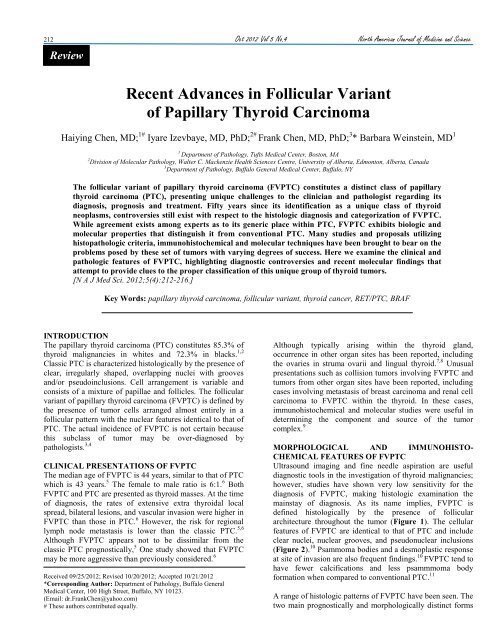
212 Oct 2012 Vol 5 No.4 North American Journal <strong>of</strong> Medic<strong>in</strong>e and ScienceReview<strong>Recent</strong> <strong>Advances</strong> <strong>in</strong> <strong>Follicular</strong> <strong>Variant</strong><strong>of</strong> <strong>Papillary</strong> <strong>Thyroid</strong> Carc<strong>in</strong>omaHaiy<strong>in</strong>g Chen, MD; 1# Iyare Izevbaye, MD, PhD; 2# Frank Chen, MD, PhD; 3 * Barbara We<strong>in</strong>ste<strong>in</strong>, MD 11Department <strong>of</strong> Pathology, Tufts Medical Center, Boston, MA2 Division <strong>of</strong> Molecular Pathology, Walter C. Mackenzie Health Sciences Centre, University <strong>of</strong> Alberta, Edmonton, Alberta, Canada3 Department <strong>of</strong> Pathology, Buffalo General Medical Center, Buffalo, NYThe follicular variant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma (FVPTC) constitutes a dist<strong>in</strong>ct class <strong>of</strong> papillarythyroid carc<strong>in</strong>oma (PTC), present<strong>in</strong>g unique challenges to the cl<strong>in</strong>ician and pathologist regard<strong>in</strong>g itsdiagnosis, prognosis and treatment. Fifty years s<strong>in</strong>ce its identification as a unique class <strong>of</strong> thyroidneoplasms, controversies still exist with respect to the histologic diagnosis and categorization <strong>of</strong> FVPTC.While agreement exists among experts as to its generic place with<strong>in</strong> PTC, FVPTC exhibits biologic andmolecular properties that dist<strong>in</strong>guish it from conventional PTC. Many studies and proposals utiliz<strong>in</strong>ghistopathologic criteria, immunohistochemical and molecular techniques have been brought to bear on theproblems posed by these set <strong>of</strong> tumors with vary<strong>in</strong>g degrees <strong>of</strong> success. Here we exam<strong>in</strong>e the cl<strong>in</strong>ical andpathologic features <strong>of</strong> FVPTC, highlight<strong>in</strong>g diagnostic controversies and recent molecular f<strong>in</strong>d<strong>in</strong>gs thatattempt to provide clues to the proper classification <strong>of</strong> this unique group <strong>of</strong> thyroid tumors.[N A J Med Sci. 2012;5(4):212-216.]Key Words: papillary thyroid carc<strong>in</strong>oma, follicular variant, thyroid cancer, RET/PTC, BRAFINTRODUCTIONThe papillary thyroid carc<strong>in</strong>oma (PTC) constitutes 85.3% <strong>of</strong>thyroid malignancies <strong>in</strong> whites and 72.3% <strong>in</strong> blacks. 1,2Classic PTC is characterized histologically by the presence <strong>of</strong>clear, irregularly shaped, overlapp<strong>in</strong>g nuclei with groovesand/or pseudo<strong>in</strong>clusions. Cell arrangement is variable andconsists <strong>of</strong> a mixture <strong>of</strong> papillae and follicles. The follicularvariant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma (FVPTC) is def<strong>in</strong>ed bythe presence <strong>of</strong> tumor cells arranged almost entirely <strong>in</strong> afollicular pattern with the nuclear features identical to that <strong>of</strong>PTC. The actual <strong>in</strong>cidence <strong>of</strong> FVPTC is not certa<strong>in</strong> becausethis subclass <strong>of</strong> tumor may be over-diagnosed bypathologists. 3,4CLINICAL PRESENTATIONS OF FVPTCThe median age <strong>of</strong> FVPTC is 44 years, similar to that <strong>of</strong> PTCwhich is 43 years. 5 The female to male ratio is 6:1. 6 BothFVPTC and PTC are presented as thyroid masses. At the time<strong>of</strong> diagnosis, the rates <strong>of</strong> extensive extra thyroidal localspread, bilateral lesions, and vascular <strong>in</strong>vasion were higher <strong>in</strong>FVPTC than those <strong>in</strong> PTC. 6 However, the risk for regionallymph node metastasis is lower than the classic PTC. 5,6Although FVPTC appears not to be dissimilar from theclassic PTC prognostically, 5 One study showed that FVPTCmay be more aggressive than previously considered. 6Received 09/25/2012; Revised 10/20/2012; Accepted 10/21/2012*Correspond<strong>in</strong>g Author: Department <strong>of</strong> Pathology, Buffalo GeneralMedical Center, 100 High Street, Buffalo, NY 10123.(Email: dr.FrankChen@yahoo.com)# These authors contributed equally.Although typically aris<strong>in</strong>g with<strong>in</strong> the thyroid gland,occurrence <strong>in</strong> other organ sites has been reported, <strong>in</strong>clud<strong>in</strong>gthe ovaries <strong>in</strong> struma ovarii and l<strong>in</strong>gual thyroid. 7,8 Unusualpresentations such as collision tumors <strong>in</strong>volv<strong>in</strong>g FVPTC andtumors from other organ sites have been reported, <strong>in</strong>clud<strong>in</strong>gcases <strong>in</strong>volv<strong>in</strong>g metastasis <strong>of</strong> breast carc<strong>in</strong>oma and renal cellcarc<strong>in</strong>oma to FVPTC with<strong>in</strong> the thyroid. In these cases,immunohistochemical and molecular studies were useful <strong>in</strong>determ<strong>in</strong><strong>in</strong>g the component and source <strong>of</strong> the tumorcomplex. 9MORPHOLOGICAL AND IMMUNOHISTO-CHEMICAL FEATURES OF FVPTCUltrasound imag<strong>in</strong>g and f<strong>in</strong>e needle aspiration are usefuldiagnostic tools <strong>in</strong> the <strong>in</strong>vestigation <strong>of</strong> thyroid malignancies;however, studies have shown very low sensitivity for thediagnosis <strong>of</strong> FVPTC, mak<strong>in</strong>g histologic exam<strong>in</strong>ation thema<strong>in</strong>stay <strong>of</strong> diagnosis. As its name implies, FVPTC isdef<strong>in</strong>ed histologically by the presence <strong>of</strong> folliculararchitecture throughout the tumor (Figure 1). The cellularfeatures <strong>of</strong> FVPTC are identical to that <strong>of</strong> PTC and <strong>in</strong>cludeclear nuclei, nuclear grooves, and pseudonuclear <strong>in</strong>clusions(Figure 2). 10 Psammoma bodies and a desmoplastic responseat site <strong>of</strong> <strong>in</strong>vasion are also frequent f<strong>in</strong>d<strong>in</strong>gs. 10 FVPTC tend tohave fewer calcifications and less psammmoma bodyformation when compared to conventional PTC. 11A range <strong>of</strong> histologic patterns <strong>of</strong> FVPTC have been seen. Thetwo ma<strong>in</strong> prognostically and morphologically dist<strong>in</strong>ct forms
North American Journal <strong>of</strong> Medic<strong>in</strong>e and Science Oct 2012 Vol 5 No.4 213are the diffuse variant and the encapsulated variant. Thediffuse follicular variant shows diffuse replacement <strong>of</strong> thegland by the neoplasm. Compared to the encapsulated form,the diffuse variant <strong>of</strong> FVPTC carries a worse prognosis anddemonstrates a higher rate <strong>of</strong> the BRAF V600E mutation,lymph node <strong>in</strong>volvement and distant metastasis. 12-14 Theencapsulated variant <strong>of</strong> FVPTC, def<strong>in</strong>ed by a complete peritumoralcapsule, has an overall excellent prognosis. 10,15,16Encapsulated FVPTC shows a dist<strong>in</strong>ctive tumor biologycompared to conventional PTC. 17 While conventional PTC(encapsulated and nonencapsulated) has a greater propensityfor lymph node metastasis (26% vs 3%) and an <strong>in</strong>creasedfrequency <strong>of</strong> capsular <strong>in</strong>vasion (65% vs 38%), encapsulatedFVPTC has a higher rate <strong>of</strong> vascular <strong>in</strong>vasion thanconventional PTC (25% vs 5%). As vascular and capsular<strong>in</strong>vasion are the most important <strong>in</strong>dicators <strong>of</strong> metastaticpotential, histopathologic evaluation <strong>of</strong> FVPTC must <strong>in</strong>cludea meticulous and thorough search for these features. Thenon<strong>in</strong>vasive variety <strong>of</strong> FVPTC can be managed likem<strong>in</strong>imally <strong>in</strong>vasive follicular carc<strong>in</strong>oma by lobectomywithout radioactive iod<strong>in</strong>e (RAI) therapy. On average, theoverall cl<strong>in</strong>ical course <strong>of</strong> FVPTC with capsular <strong>in</strong>vasion isnoted to be quite <strong>in</strong>dolent particularly if no distant metastasisis identified at presentation.Rare histologic patterns <strong>of</strong> FVPTCs, such as mixed follicularand papillary pattern, adenoid cystic pattern, andmacr<strong>of</strong>ollicular pattern, have been reported <strong>in</strong> the literature.A reported case <strong>of</strong> FVPTC conta<strong>in</strong><strong>in</strong>g adenoid cystic areasexhibited prom<strong>in</strong>ent follicular clusters conta<strong>in</strong><strong>in</strong>g hyal<strong>in</strong>eglobules and areas with morula-like groups <strong>of</strong> neoplasticcells. 18 Immunohistochemical sta<strong>in</strong><strong>in</strong>g was positive forthyroglobul<strong>in</strong> <strong>in</strong> the follicular region but negative <strong>in</strong> thehyal<strong>in</strong>e globules. This feature may be <strong>of</strong> importance to thecytopathologist when consider<strong>in</strong>g the possibility <strong>of</strong> adenoidcystic carc<strong>in</strong>oma metastatic to the thyroid.Reported cases <strong>of</strong> mixed follicular and papillary patterns <strong>of</strong>PTC have shown molecular features suggest<strong>in</strong>g that they bestfit <strong>in</strong>to the category <strong>of</strong> conventional PTC rather FVPTC. 19BRAF mutation occurred with a frequency more consistentwith conventional PTC. Furthermore, both follicular andpapillary areas <strong>of</strong> these mixed tumors displayed the BRAFmutations.Macr<strong>of</strong>ollicular FVPTC is another unusual variant that canbe confused with nodular goiter or follicular adenoma. 20 Thisvariant <strong>of</strong> FVPTC, despite be<strong>in</strong>g described as hav<strong>in</strong>g a goodprognosis with a low <strong>in</strong>cidence <strong>of</strong> metastases, can onoccasion present as a highly aggressive tumor, mak<strong>in</strong>g itsdetection and proper characterization <strong>of</strong> importance.Common diagnostic difficulties posed by FVPTC <strong>in</strong>clude: (1)A high number <strong>of</strong> these tumors develop with<strong>in</strong> a background<strong>of</strong> nodular goiter, resembl<strong>in</strong>g an adenoma or adenomatoidnodules which are mostly encapsulated and lack vascular orcapsular <strong>in</strong>vasion. 21 (2) Lesions can be multifocal, without adiffuse distribution <strong>of</strong> the typical nuclear features <strong>of</strong> PTC. Inthese cases, the presence <strong>of</strong> <strong>in</strong>complete or focal characteristicnuclear features makes the dist<strong>in</strong>ction from follicularadenoma or follicular carc<strong>in</strong>oma difficult. 21 (3) Mostencapsulated FVPTCs are solitary, with no evidence <strong>of</strong><strong>in</strong>vasion, and are conf<strong>in</strong>ed to the thyroid. 10 These facts havepractical importance <strong>in</strong> the management <strong>of</strong> these tumorsbecause overdiagnosis results <strong>in</strong> excessive treatment,<strong>in</strong>clud<strong>in</strong>g total thyroidectomy with radioactive iodidetherapy.Significant <strong>in</strong>ter-observer and <strong>in</strong>tra-observer variation havebeen noted even among experts, with major <strong>in</strong>ter-observerdisagreements reported <strong>in</strong> up to 40% <strong>of</strong> cases. Ironically,<strong>in</strong>tra-observer agreement was found to range from 17 -100%. 21 A general consensus exists as to the most importantdiagnostic features, which <strong>in</strong>clude nuclear clear<strong>in</strong>g, nucleargrooves, nuclear overlapp<strong>in</strong>g and crowd<strong>in</strong>g, nuclearmembrane irregularity and nuclear enlargement. 21Discrepancies arise due to the lack <strong>of</strong> agreement on them<strong>in</strong>imal criteria necessary for a def<strong>in</strong>ite diagnosis <strong>of</strong>FVPTC. 21The absence <strong>of</strong> a strict and uniform approach among expertpathologists, particularly <strong>in</strong> difficult cases, results <strong>in</strong> the use<strong>of</strong> terms such as “multifocal papillary thyroid carc<strong>in</strong>omaaris<strong>in</strong>g <strong>in</strong> a benign nodule”, “follicular tumor <strong>of</strong> uncerta<strong>in</strong>malignant potential” or the consideration <strong>of</strong> an entire noduleshow<strong>in</strong>g only focal nuclear changes as a FVPTC. A range <strong>of</strong>proposals have been made to clarify this issue. LiVolsi andBaloch prefer a scheme <strong>in</strong> which a diagnosis <strong>of</strong> FVPTC ismade on any encapsulated lesion that shows any area withthe characteristic cytologic features <strong>of</strong> papillary thyroidcarc<strong>in</strong>oma. 22 Chan suggests us<strong>in</strong>g stricter criteria <strong>in</strong>clud<strong>in</strong>gthe evaluation <strong>of</strong> major and m<strong>in</strong>or features. 3 The four majorfeatures proposed <strong>in</strong>clude: (1) oval rather than round nuclei,(2) crowd<strong>in</strong>g <strong>of</strong> nuclei with lack <strong>of</strong> polarity <strong>in</strong> the follicles,(3) clear or pale nuclear chromat<strong>in</strong> pattern throughout theentire lesion or prom<strong>in</strong>ent nuclear grooves, and (4) presence<strong>of</strong> psammoma bodies. When only a s<strong>in</strong>gle one <strong>of</strong> thesefeatures is identified, the presence <strong>of</strong> all <strong>of</strong> the follow<strong>in</strong>gsubsidiary criteria is necessary to establish the diagnosis.These subsidiary criteria <strong>in</strong>clude: (1) presence <strong>of</strong> abortivepapillae, (2) predom<strong>in</strong>antly elongated or irregularly shapedfollicles, (3) dark-sta<strong>in</strong><strong>in</strong>g colloid, (4) presence <strong>of</strong> rarenuclear pseudo<strong>in</strong>clusions, and (5) mult<strong>in</strong>ucleated histiocytes<strong>in</strong> the lumen <strong>of</strong> the follicles. A group <strong>of</strong> Chernobylpathologists advocates the use <strong>of</strong> the term<strong>in</strong>ology <strong>of</strong> “welldifferentiatedthyroid tumor <strong>of</strong> uncerta<strong>in</strong> malignant potential(WDT-UMP)” when <strong>in</strong>complete or equivocal features arepresent rather than an outright diagnosis <strong>of</strong> carc<strong>in</strong>oma. 4 Thismay obviate the fear <strong>of</strong> litigation that results <strong>in</strong> theoverdiagnosis <strong>of</strong> malignancy and the excessively aggressivetreatment <strong>of</strong> this group <strong>of</strong> tumors, which have been shownnot to be associated with any significant risk <strong>of</strong> recurrence ormetastasis by many authors. 3,4Many studies demonstrate the use <strong>of</strong> immunohistochemistryand molecular assays <strong>in</strong> separat<strong>in</strong>g FVPTC from other benignconditions. 23,24 A study <strong>of</strong> the immunomarkers, galect<strong>in</strong>-3,cytokerat<strong>in</strong> 19 (CK19), Ret oncoprote<strong>in</strong> (RET), and HBME-1suggested a high utility <strong>of</strong> these markers <strong>in</strong> differentiat<strong>in</strong>gbenign lesions from malignant tumors. 24 Saleh and collegues
214 Oct 2012 Vol 5 No.4 North American Journal <strong>of</strong> Medic<strong>in</strong>e and Sciencehave demonstrated galect<strong>in</strong>-3 expression <strong>in</strong> a large number <strong>of</strong>malignant tumors <strong>in</strong> contrast to benign lesions with areported sensitivity and specificity <strong>of</strong> 92.6% and 77.3%respectively. In the same study, sta<strong>in</strong><strong>in</strong>g for HBME-1 wasalso pronounced <strong>in</strong> malignant lesions and showed asensitivity and specificity <strong>of</strong> 88.9% and 72.7%. However, theuse <strong>of</strong> these markers is limited by their expression <strong>in</strong> asmaller number <strong>of</strong> benign lesions (22.7% for galect<strong>in</strong>-3, 31%for Ret and 29.5% for CK19). The illustration <strong>of</strong> positivegalect<strong>in</strong>-3 sta<strong>in</strong><strong>in</strong>g <strong>of</strong> FVPTC and positive CK19 sta<strong>in</strong><strong>in</strong>g areshown <strong>in</strong> Figure 3 and Figure 4.Figure 1. Low-power view <strong>of</strong> <strong>Follicular</strong> <strong>Variant</strong> <strong>of</strong><strong>Papillary</strong> <strong>Thyroid</strong> Carc<strong>in</strong>oma. Tumor shows follicles <strong>of</strong>vary<strong>in</strong>g sizes with colloid. (Magnification 100x).Figure 2. High-power view <strong>of</strong> <strong>Follicular</strong> <strong>Variant</strong> <strong>of</strong> <strong>Papillary</strong><strong>Thyroid</strong> Carc<strong>in</strong>oma. Tumor shows follicles with nuclearfeatures <strong>of</strong> papillary carc<strong>in</strong>oma. Blue arrow: Nucear grooves;Black arrow: pseudonuclear <strong>in</strong>clusion. (Magnification 400x).Figure 3. <strong>Follicular</strong> <strong>Variant</strong> <strong>of</strong> <strong>Papillary</strong> <strong>Thyroid</strong>Carc<strong>in</strong>oma is strongly positive for Galact<strong>in</strong> 3(Magnification 100x).Figure 4. <strong>Follicular</strong> <strong>Variant</strong> <strong>of</strong> <strong>Papillary</strong> <strong>Thyroid</strong> Carc<strong>in</strong>omais positive for CK19 (Magnification 100x).MOLECULAR GENETICS OF FVPTCTumorigenesis <strong>of</strong> thyroid carc<strong>in</strong>omas <strong>in</strong>volves <strong>in</strong> severaloncogenes, <strong>in</strong>clud<strong>in</strong>g RET, RAS, and BRAF, etc. 25,26 RETgene encodes a membrane receptor tyros<strong>in</strong>e k<strong>in</strong>ase <strong>in</strong>volved<strong>in</strong> signal<strong>in</strong>g via a ligand-coreceptor-RET prote<strong>in</strong> complex.RET dimerization is triggered by ligand b<strong>in</strong>d<strong>in</strong>g and complexformation, result<strong>in</strong>g <strong>in</strong> tyros<strong>in</strong>e residue autophosphorylationwith<strong>in</strong> its <strong>in</strong>tracytoplasmic doma<strong>in</strong>. Further tyros<strong>in</strong>ephosphorylation <strong>of</strong> downstream target prote<strong>in</strong>s produces anactivated signal<strong>in</strong>g pathway. Target prote<strong>in</strong>s <strong>in</strong>cludemitogen-activat<strong>in</strong>g prote<strong>in</strong> k<strong>in</strong>ase (MAPK), extracellularsignal-regulated k<strong>in</strong>ase (ERK)1/2, phosphatidyl<strong>in</strong>ositol 3-k<strong>in</strong>ase, c-Jun N-term<strong>in</strong>al k<strong>in</strong>ase, p38, ERK5 and cAMPresponsive element-b<strong>in</strong>d<strong>in</strong>g prote<strong>in</strong>. 25
North American Journal <strong>of</strong> Medic<strong>in</strong>e and Science Oct 2012 Vol 5 No.4 215FVPTC has a molecular identity <strong>in</strong>termediate between thetwo well differentiated thyroid carc<strong>in</strong>omas,,follicularcarc<strong>in</strong>oma (FC) and PTC. FC is characterized by RASmutations and PAX8/PPARγ rearrangement. 26-30 The genefusion <strong>of</strong> PAX8/PPARγ rearrangement has beencytogenetically def<strong>in</strong>ed as translocation t(2:3)(q13;p25). 29PTC has a genetic pr<strong>of</strong>ile consist<strong>in</strong>g <strong>of</strong> somaticrearrangements <strong>of</strong> the RET protooncogene 25,31 and BRAFmutations. 32,33 FVPTC has a high occurrence <strong>of</strong> RASmutations and PAX8/PPARγ rearrangements 34 but a lesscommon BRAF K601E form, which is present <strong>in</strong> about 7%<strong>of</strong> cases. 35 Other BRAF mutations reported <strong>in</strong> FVPTC<strong>in</strong>clude V600E, G474R and a novel ga<strong>in</strong> <strong>of</strong> function T5991-VKSR(600-603) del. 36 These mutations with the exception <strong>of</strong>G474R share biological similarities <strong>in</strong> activat<strong>in</strong>g the MAPKpathway. The G474R mutation knocks down the enzymaticactivity <strong>of</strong> BRAF, provid<strong>in</strong>g a first example <strong>of</strong> a knockdownmutation <strong>in</strong> FVPTC. The genetic pr<strong>of</strong>il<strong>in</strong>g <strong>of</strong> thyroid tumors<strong>of</strong>fers potential diagnostic and therapeutic targets <strong>in</strong> theirmanagement. Candidate compounds, many with tyros<strong>in</strong>ek<strong>in</strong>ase <strong>in</strong>hibitor function, are presently <strong>in</strong> various phases <strong>of</strong>cl<strong>in</strong>ical trials. 37 The role <strong>of</strong> these mutations <strong>in</strong> prognosisrema<strong>in</strong>s controversial. Some studies suggest a correlationbetween RET/PTC and tumor aggressiveness 38 while others<strong>in</strong>dicate that tumors harbor<strong>in</strong>g RET/PTC show slow growthand lower risk <strong>of</strong> progression to poorly differentiated andundifferentiated thyroid carc<strong>in</strong>oma. 25,31,39CLINICAL UTILITY OF MOLECULAR TESTING INFVPTCWhen us<strong>in</strong>g the Bethesda classification for the diagnosis <strong>of</strong>thyorid neoplasms, up to 3.6% <strong>of</strong> specimen will fall <strong>in</strong>to the<strong>in</strong>determ<strong>in</strong>ate category. 40 The risk <strong>of</strong> malignancy <strong>in</strong> thiscategory may be up to 15-30%. 40 Molecular tests (especiallyassays for BRAF V600E and Kras mutations) have beenshown to play an adjunct role to cytology samples <strong>in</strong>equivocal cases classified as follicular lesions <strong>of</strong>undeterm<strong>in</strong>ed significance, improv<strong>in</strong>g diagnostic accuracy <strong>of</strong>malignancy and direct<strong>in</strong>g subsequent therapy. 41,42 Althoughthese molecular techniques have not achieved widespreadcl<strong>in</strong>ical usage, but they are ga<strong>in</strong><strong>in</strong>g ground <strong>in</strong> referencelaboratories. Their utility, nevertheless, is restricted toclassical PTC due to the low <strong>in</strong>cidence <strong>of</strong> BRAF mutations <strong>in</strong>FVPTC and the high occurrence <strong>of</strong> Kras mutations <strong>in</strong> benignfollicular lesions. 35 Suitable cl<strong>in</strong>ical molecular biomarkers forFVPTC still await discovery.CONCLUSIONS<strong>in</strong>ce its description fifty years ago, knowledge regard<strong>in</strong>gFVPTC has expanded significantly. However, difficultypersists regard<strong>in</strong>g the precise histopathologic calssification <strong>of</strong>those cases with less dist<strong>in</strong>ctive diagnostic features or withcharacteristics overlapp<strong>in</strong>g with that <strong>of</strong> FC or <strong>Follicular</strong>adenoma. The use <strong>of</strong> molecular techniques, while furtherelucidat<strong>in</strong>g tumor biology and <strong>in</strong>dicat<strong>in</strong>g potentialtherapeutic targets, have not been completely successful <strong>in</strong>improv<strong>in</strong>g diagnostic sensitivity or specificity. Furtherresearch will be necessary to achieve this goal.CONFLICT OF INTERESTThe authors have no conflict <strong>of</strong> <strong>in</strong>terest to disclose.REFERENCES1. Correa P, Chen VW. Endocr<strong>in</strong>e gland cancer. Cancer. 1995;75(1Suppl):338-352.2. Ito Y, Miyauchi A. Prognostic factors and therapeutic strategies fordifferentiated carc<strong>in</strong>omas <strong>of</strong> the thyroid. Endocr J. 2009;56(2):177-192.3. Chan JK. Strict criteria should be applied <strong>in</strong> the diagnosis <strong>of</strong>encapsulated follicular variant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma. Am JCl<strong>in</strong> Pathol. 2002;117(1):16-18.4. Williams ED. Two proposals regard<strong>in</strong>g the term<strong>in</strong>ology <strong>of</strong> thyroidtumors. Int J Surg Pathol. 2000;8(3):181-183.5. Zidan J, Karen D, Ste<strong>in</strong> M, Rosenblatt E, Basher W, Kuten A. Pureversus follicular variant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma: cl<strong>in</strong>icalfeatures, prognostic factors, treatment, and survival. Cancer.2003;97(5):1181-1185.6. Hagag P, Hod N, Kummer E, Cohenpour M, Horne T, Weiss M.<strong>Follicular</strong> variant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma: cl<strong>in</strong>ical-pathologicalcharacterization and long-term follow-up. Cancer J. 2006;12(4):275-282.7. Celest<strong>in</strong>o R, Magalhães J, Castro P, et al. A folicular variant <strong>of</strong>papillary thyroid carc<strong>in</strong>oma <strong>in</strong> struma ovarii. Case report with uniquemoleualr alterations. Histopathology. 2009;55(4):482-487.8. Hari CK, Kumar M, Abo-Khatwa MM, Adams-Williams J, Zeitoun H.<strong>Follicular</strong> variant <strong>of</strong> papillary carc<strong>in</strong>oma aris<strong>in</strong>g from l<strong>in</strong>gual thryoid.Ear Nose Throat J. 2009;88(6):E7.9. Yu J, Nikiforova MN, Hodak SP, et al. Tumor to tumor Metastses to<strong>Follicular</strong> <strong>Variant</strong> <strong>of</strong> <strong>Papillary</strong> <strong>Thyroid</strong> Carc<strong>in</strong>oma:Histoloic,Immunohistochemical amd molecular studeis <strong>of</strong> two unusual cases.Endocr Pathol. 2009;20(4):235-242.10. Baloch ZW, Livolsi VA. <strong>Follicular</strong>-patterned lesions <strong>of</strong> the thyroid:thebane <strong>of</strong> the pathologist. Am J Cl<strong>in</strong> Pathol. 2002;117(1):143-150.11. Lam AK, Lo CY, Lam KS. <strong>Papillary</strong> carcimoma <strong>of</strong> thyroid: a 30-yrclicopathologial revview <strong>of</strong> the histological variants. Endocr Pathol.2005;16(4):323-330.12. Gupta S, Ajise O, Dultz L, et al. <strong>Follicular</strong> variant <strong>of</strong> papillary thyroidcancer: encapsulated, nonencapsulated, and diffuse: dist<strong>in</strong>ct biologicand cl<strong>in</strong>ical entities. Arch Otolaryngol Head Neck Surg.2012;138(3):227-233.13. Ivanova R, Soares P, Castro P, Sobr<strong>in</strong>ho-Simões M. Diffuse (ormult<strong>in</strong>odular) follicular variant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma: acl<strong>in</strong>icopathologic and immunohistochemical analysis <strong>of</strong> ten cases <strong>of</strong> anaggressive form <strong>of</strong> differentiated thyroid carc<strong>in</strong>oma. Virchows Arch.2002;440(4):418-424.14. Mizukami Y, Nonomura A, Michigishi T, Ohmura K, Noguchi M,Ishizaki T. Diffuse follicular variant <strong>of</strong> papillary carc<strong>in</strong>oma <strong>of</strong> thethyroid. Histopathology. 1995;27(6):575-577.15. Chem KT, Rosai J. <strong>Follicular</strong> variant <strong>of</strong> thyroid papillary carc<strong>in</strong>oma: acl<strong>in</strong>icopathologic study <strong>of</strong> six cases. Am J Surg Pathol. 1977;1(2):123-130.16. Ghosse<strong>in</strong> R. Encapsulated malignant follicular cell-derived thyroidtumors. Endocr Pathol. 2010;21(4):212-218.17. Rivera M, Tuttle RM, Patel S, Shaha A, Shah JP, Ghosse<strong>in</strong> RA.Encapsulated papillary thyroid carc<strong>in</strong>oma: a cl<strong>in</strong>ico-pathologic study <strong>of</strong>106 cases with emphasis on its morphologic subtypes (histologicgrowth pattern). <strong>Thyroid</strong>. 2009;19(2):119-127.18. Mandal S, Ja<strong>in</strong> S. Adenoid cystic pattern <strong>in</strong> follicular variant <strong>of</strong>papillary thyroid carc<strong>in</strong>oma: a report <strong>of</strong> four cases. Cytopathology.2010;21(2):93-96.19. Jakubowski M, Hunt JL. BRAF mutational analysis <strong>in</strong> papillarycarc<strong>in</strong>omas with mixed follicular and papillary growth patterns.2009;33(11):1590-1593.20. Cardenas MG, K<strong>in</strong>i S, Wisgerh<strong>of</strong> M. Two patients with highlyaggressive macr<strong>of</strong>ollicular variant <strong>of</strong> papillary thyroid carc<strong>in</strong>oma.<strong>Thyroid</strong>. 2009;19(4):413-416.21. Elsheikh TM, Asa SL, Chan JK, et al. Interobserver and <strong>in</strong>traobservervariation among experts <strong>in</strong> the diagnosis <strong>of</strong> thyroid follicular lesionswith borderl<strong>in</strong>e nuclear features <strong>of</strong> papillary carc<strong>in</strong>oma. Am J Cl<strong>in</strong>Pathol. 2008;130(5):736-744.22. LiVolsi VA, Baloch ZW. <strong>Follicular</strong> neoplasms <strong>of</strong> the thyroid: view,biases, and experiences. Adv Anat Pathol. 2004;11(6):279-287.23. Saleh HA, J<strong>in</strong> B, Barnwell J, Alzohaili O. Utility <strong>of</strong>immunohistochemical markers <strong>in</strong> differentiat<strong>in</strong>g benign frommalignant follicular-derived thyroid nodules. Diagn Pathol. 2010;5:9.24. Saleh HA, Feng J, Tabassum F, Al-Zohaili O, Husa<strong>in</strong> M, Giorgadze T.Differential expression <strong>of</strong> galect<strong>in</strong>-3, CK19, HBME1, and Ret
216 Oct 2012 Vol 5 No.4 North American Journal <strong>of</strong> Medic<strong>in</strong>e and Scienceoncoprote<strong>in</strong> <strong>in</strong> the diagnosis <strong>of</strong> thyroid neoplasms by f<strong>in</strong>e needleaspiration biopsy. Cytojournal. 2009;6:18.25. Nikiforov YE. RET/PTC rearrangement <strong>in</strong> thyroid tumors. EndocrPathol. 2002;13(1):3-16.26. Nikiforova MN, Lynch RA, Bidd<strong>in</strong>ger PW, et al. RAS po<strong>in</strong>t mutationsand PAX8-PPAR gamma rearrangement <strong>in</strong> thyroid tumors: evidencefor dist<strong>in</strong>ct molecular pathways <strong>in</strong> thyroid follicular carc<strong>in</strong>oma. J Cl<strong>in</strong>Endocr<strong>in</strong>ol Metab. 2003;88(5):2318-2326.27. Vasko V, Ferrand M, Di Crist<strong>of</strong>aro J, Carayon P, Henry JF, de MiccoC. Specific pattern <strong>of</strong> RAS oncogene mutations <strong>in</strong> follicular thyroidtumors. J Cl<strong>in</strong> Endocr<strong>in</strong>ol Metab. 2003;88(6):2745-2752.28. Marques AR, Espad<strong>in</strong>ha C, Catar<strong>in</strong>o AL, et al. Expression <strong>of</strong> PAX8-PPAR gamma 1 rearrangements <strong>in</strong> both follicular thyroid carc<strong>in</strong>omasand adenomas. J Cl<strong>in</strong> Endocr<strong>in</strong>ol Metab. 2002;87(8):3947-3952.29. Kroll TG, Sarraf P, Pecciar<strong>in</strong>i L, et al. PAX8-PPARgamma1 fusiononcogene <strong>in</strong> human thyroid carc<strong>in</strong>oma [corrected]. Science.2000;289(5483):1357-1360. Erratum <strong>in</strong> Science 2000;289(5484):1474.30. Fukahori M, Yoshida A, Hayashi H, et al. The associations betweenRAS mutations and cl<strong>in</strong>ical characteristics <strong>in</strong> follicular thyroid tumors:new <strong>in</strong>sights from a s<strong>in</strong>gle center and a large patient cohort. <strong>Thyroid</strong>.2012;22(7):683-689.31. Soares P, Fonseca E, Wynford-Thomas D, Sobr<strong>in</strong>ho-Simões M.Sporadic ret-rearranged papillary carc<strong>in</strong>oma <strong>of</strong> the thyroid: a subset <strong>of</strong>slow grow<strong>in</strong>g, less aggressive thyroid neoplasms? J Pathol.1998;185(1):71-78.32. Soares P, Trovisco V, Rocha AS, et al. BRAF mutations and RET/PTCrearrangements are alternative events <strong>in</strong> the etiopathogenesis <strong>of</strong> PTC.Oncogene. 2003;22(29):4578-4580.33. Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fag<strong>in</strong>JA. High prevalence <strong>of</strong> BRAF mutations <strong>in</strong> thyroid cancer: geneticevidence for constitutive activation <strong>of</strong> the RET/PTC-RAS-BRAFsignal<strong>in</strong>g pathway <strong>in</strong> papillary thyroid carc<strong>in</strong>oma. Cancer Res.2003;63(7):1454-1457.34. Castro P, Rebocho AP, Soares RJ, et al. PAX8-PPARgammarearrangement is frequently detected <strong>in</strong> the follicular variant <strong>of</strong>papillary thyroid carc<strong>in</strong>oma. J Cl<strong>in</strong> Endocr<strong>in</strong>ol Metab. 2006;91(1):213-220.35. Trovisco V, Vieira de Castro I, Soares P, et al. (2004). BRAFmutations are associated with some histological types <strong>of</strong> papillarythyroid carc<strong>in</strong>oma. J Pathol. 2004;202(2):247-251.36. De Falco V, Giann<strong>in</strong>i R, Tamburr<strong>in</strong>o A, et al. Functionalcharacterization <strong>of</strong> the novel T599I-VKSRdel BRAF mutation <strong>in</strong> afollicular variant papillary thyroid carc<strong>in</strong>oma. J Cl<strong>in</strong> Endocr<strong>in</strong>ol Metab.2008;93(11):4398-4402.37. Couto JP, Prazeres H, Castro P, et al. How molecular pathology ischang<strong>in</strong>g and will change the therapeutics <strong>of</strong> patients with follicularcell-derived thyroid cancer. J Cl<strong>in</strong> Pathol. 2009;62(5):414-421.38. Jhiang SM, Caruso DR, Gilmore E, et al. Detection <strong>of</strong> the PTC/retTPConcogene <strong>in</strong> human thyroid cancers. Oncogene. 1992;7(7):1331-1337.39. Tall<strong>in</strong>i G, Santoro M, Helie M, et al. RET/PTC oncogene activationdef<strong>in</strong>es a subset <strong>of</strong> papillary thyroid carc<strong>in</strong>omas lack<strong>in</strong>g evidence <strong>of</strong>progression to poorly differentiated or undifferentiated tumorphenotypes. Cl<strong>in</strong> Cancer Res. 1998;4(2):287-294.40. Cibas ES, Ali SZ. The Bethesda System for Report<strong>in</strong>g <strong>Thyroid</strong>Cytopathology. American Journal <strong>of</strong> Cl<strong>in</strong>ical Pathology.2009;132(5):658-665.41. Nikiforova MN, NIkiforov YE. Molecular Diagnostics and Predictors<strong>in</strong> <strong>Thyroid</strong> Cancer. <strong>Thyroid</strong>. 2009;19(12):1351-1361.42. Marchetti I, Lessi F, Mazzanti CM, et al. A morpho-moleculardiagnosis <strong>of</strong> PTC: Braf V600E detection as an important tool <strong>in</strong>preoperative evaluation <strong>of</strong> FNA. <strong>Thyroid</strong>. 2009;19(8): 837-842.













