

Pyelonephritis in an Immunocompromised Host Presented as a ...
Pyelonephritis in an Immunocompromised Host Presented as a ...
Pyelonephritis in an Immunocompromised Host Presented as a ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
136 Jul 2010 Vol 3 No.3 North Americ<strong>an</strong> Journal of Medic<strong>in</strong>e <strong>an</strong>d Science<strong>Pyelonephritis</strong> <strong>in</strong> <strong>an</strong> <strong>Immunocompromised</strong> <strong>Host</strong><strong>Presented</strong> <strong>as</strong> a Drug Reaction-Like SyndromeMerfake H Semret, MD, S<strong>an</strong>jeev Sethi, MD, Qi Qi<strong>an</strong>, MDAbstractIntroductionInfection is the lead<strong>in</strong>g cause of death <strong>in</strong> patients onchronic immunosuppression. Diagnosis of <strong>in</strong>fection <strong>in</strong>these patients c<strong>an</strong> be challeng<strong>in</strong>g <strong>as</strong> immunosuppress<strong>an</strong>tsc<strong>an</strong> blunt systemic <strong>in</strong>flammatory response <strong>an</strong>d thereforeelude ready detection.C<strong>as</strong>e presentationWe report <strong>an</strong> unusual c<strong>as</strong>e of pyelonephritis present<strong>in</strong>g <strong>as</strong>a drug reaction-like syndrome <strong>in</strong> a 49-year-old Cauc<strong>as</strong>i<strong>an</strong>male with crescentic IgA nephropathy on chronicimmunosuppress<strong>an</strong>ts. His <strong>in</strong>itial presentation w<strong>as</strong>circulatory collapse without leukocytosis <strong>an</strong>dleukocyturia. The episode occurred just days follow<strong>in</strong>gthe conversion cyclophosphamide to azathiopr<strong>in</strong>e,creat<strong>in</strong>g <strong>an</strong> impression that the rare azathiopr<strong>in</strong>e<strong>as</strong>sociated<strong>an</strong>aphylactic reaction might have accountedfor his symptoms. Azathiopr<strong>in</strong>e w<strong>as</strong> held <strong>an</strong>d he w<strong>as</strong>empirically treated with <strong>an</strong>tibiotics for three days, whichled to symptom resolution. Few days later, he presentedwith <strong>an</strong>other nearly identical episode, shortly after the re<strong>in</strong>itiationof azathiopr<strong>in</strong>e, further suggest<strong>in</strong>g thepossibility of drug reaction. His laboratory studies,however, were <strong>in</strong>consistent with <strong>an</strong>aphylactic reaction.Eventually, the diagnosis of pyelonephritis w<strong>as</strong>established by a kidney biopsy, show<strong>in</strong>g <strong>in</strong>tense<strong>in</strong>terstitial polymorphonucleocyte <strong>in</strong>filtrates <strong>an</strong>dnumerous <strong>in</strong>tratubular microabscesses. He recoveredfully with <strong>an</strong> extended course of <strong>an</strong>tibiotic treatment.Received 06/07/2010; Revised 07/28/2010; Accepted 07/30/2010Merfake H Semret, MDMayo Cl<strong>in</strong>ic, Division of Nephrology <strong>an</strong>d Hypertension, 200First Street SW, Rochester, MN 55905, USAEmail: semret.merfake@mayo.eduS<strong>an</strong>jeev Sethi, MDMayo Cl<strong>in</strong>ic, Department of Laboratory Medic<strong>in</strong>e <strong>an</strong>dPathology, 200 First Street SW, Rochester, MN 55905, USAEmail: sethi.s<strong>an</strong>jeev@mayo.edu(* Correspond<strong>in</strong>g author)Qi Qi<strong>an</strong>, MDMayo Cl<strong>in</strong>ic, Division of Nephrology <strong>an</strong>d Hypertension, 200First Street SW, Rochester, MN 55905, USAEmail: qi<strong>an</strong>.qi@mayo.eduConclusionImmunosuppressive therapy c<strong>an</strong> m<strong>as</strong>k cl<strong>in</strong>icalm<strong>an</strong>ifestations of <strong>in</strong>fection which, when unrecognized <strong>an</strong>duntreated, c<strong>an</strong> be life-threaten<strong>in</strong>g. This c<strong>as</strong>e illustrates theimport<strong>an</strong>ce of ma<strong>in</strong>ta<strong>in</strong><strong>in</strong>g a high vigil<strong>an</strong>ce <strong>an</strong>demploy<strong>in</strong>g all available methods to <strong>in</strong>vestigate a potentialsource of <strong>in</strong>fection <strong>in</strong> patients with impaired immunity.[N A J Med Sci. 2010;3(3):136-139.]Key Words: <strong>Pyelonephritis</strong>, drug reaction, Azathiopr<strong>in</strong>eIntroductionImmunosuppression compromises the host defense <strong>an</strong>dexposes patients to a variety of <strong>in</strong>fections. In patients withglomerulonephritis on chronic immunosuppression, <strong>in</strong>fectionis the lead<strong>in</strong>g cause of death 1 . One of the most commonbacterial <strong>in</strong>fections is ur<strong>in</strong>ary tract <strong>in</strong>fection (UTI) caused bypathogenic Escherichia coli 2 . Studies <strong>in</strong> recipients of org<strong>an</strong>tr<strong>an</strong>spl<strong>an</strong>tation show that when UTI occurs <strong>in</strong> patients onchronic immunosuppress<strong>an</strong>ts, it tends to be more severe <strong>an</strong>d<strong>as</strong>sociated with a higher rate of complications, <strong>in</strong>clud<strong>in</strong>gseptic shock <strong>an</strong>d multiorg<strong>an</strong> failure 3 , which could be rapidlyfatal with a high (> 50%) mortality rate even under optimalm<strong>an</strong>agement 4 . Additionally, immunosuppress<strong>an</strong>ts c<strong>an</strong> bluntsystemic <strong>in</strong>flammatory response; <strong>in</strong>fections may not presentwith their typical symptomatology <strong>an</strong>d therefore c<strong>an</strong> eludeready detection. Under such circumst<strong>an</strong>ces, the search shouldbe rigorous before the possibility of <strong>in</strong>fection c<strong>an</strong> bedismissed.C<strong>as</strong>e PresentationA 49-year-old m<strong>an</strong> with IgA nephropathy, hypertension, <strong>an</strong>dtype II diabetes w<strong>as</strong> admitted to our hospital for fever, rigors,frontal headache, <strong>an</strong>d lightheadedness of one-day duration.He w<strong>as</strong> diagnosed 6.5 months prior with crescentic IgAnephropathy. His serum creat<strong>in</strong><strong>in</strong>e level w<strong>as</strong> 177 µmol/L (53-97 µmol/L), <strong>an</strong>d ur<strong>in</strong>e sediment active. After 6-monthtreatment with prednisone <strong>an</strong>d cyclophosphamide, his serumcreat<strong>in</strong><strong>in</strong>e stabilized at 106 µmol/L (GFR per MDRD 1.14ml/sec/1.73m 2 ) <strong>an</strong>d ur<strong>in</strong>e sediment became <strong>in</strong>active.Cyclophosphamide w<strong>as</strong> then replaced by azathiopr<strong>in</strong>e (75 mgtwice daily) 16 days prior to the admission. He cont<strong>in</strong>ued onprednisone 5 mg daily, lis<strong>in</strong>opril 20 mg daily, Losart<strong>an</strong> 50mg daily, trimethoprim sulfamethoxazole DS (TMP/SMX)once every other day, <strong>an</strong>d subcut<strong>an</strong>eous <strong>in</strong>sul<strong>in</strong> <strong>in</strong>jection. Hehad a complete urological work-up previously for hematuriawhich w<strong>as</strong> unremarkable. The review of systems w<strong>as</strong>
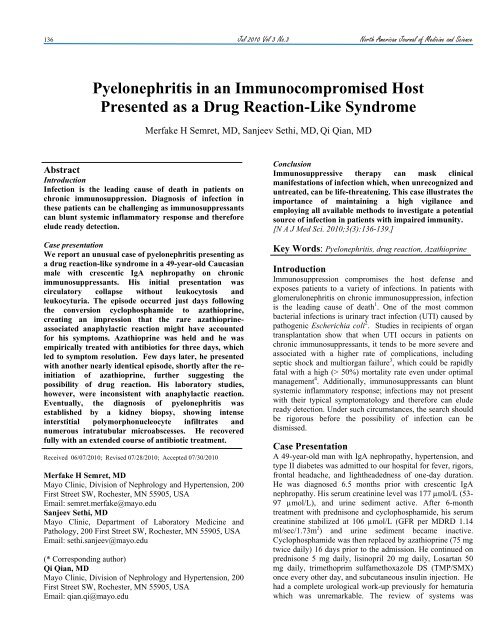
North Americ<strong>an</strong> Journal of Medic<strong>in</strong>e <strong>an</strong>d Science Jul 2010 Vol 3 No.3 137negative for version ch<strong>an</strong>ge, sore throat, cough, diarrhea,dysuria or ur<strong>in</strong>ary urgency.Eleven days prior to the current admission (5 days after theswitch<strong>in</strong>g from cyclophosphamide to azathiopr<strong>in</strong>e), he w<strong>as</strong>admitted to a local hospital for the same symptoms of fever,rigors, headache <strong>an</strong>d lightheadedness. His temperature w<strong>as</strong>39.5°C <strong>an</strong>d BP 90/60 mmHg. He did not exhibit <strong>an</strong>y focalabnormality. His WBC w<strong>as</strong> 7.9 x 10 9 /L. Ur<strong>in</strong>alysis showed 4WBC/HPF. Blood <strong>an</strong>d ur<strong>in</strong>e cultures were negative. He w<strong>as</strong>fluid resuscitated <strong>an</strong>d received <strong>in</strong>travenous ceftriaxone <strong>an</strong>dstress-dose steroids. Azathiopr<strong>in</strong>e w<strong>as</strong> held. The shock-likesymptoms resolved, but he w<strong>as</strong> generally feel<strong>in</strong>g unwell. Hew<strong>as</strong> discharged on the 3 rd day without further <strong>an</strong>tibiotics.Seven-days later, the prednisone dosage w<strong>as</strong> tapered to thema<strong>in</strong>ten<strong>an</strong>ce dose <strong>an</strong>d he resumed azathiopr<strong>in</strong>e. Five hoursafter tak<strong>in</strong>g the medications, he started to experience nearlyidentical symptoms which led to the current admission.On exam<strong>in</strong>ation, he appeared ill. His temperature w<strong>as</strong>39.5°C, BP 93/42 mmHg, HR 116/m<strong>in</strong>, <strong>an</strong>d RR 28/m<strong>in</strong>. Hislung fields were clear, abdomen benign, fl<strong>an</strong>ks non-tender topercussion, sk<strong>in</strong> no r<strong>as</strong>h, extremities no edema, <strong>an</strong>dneurologically non-focal. Laboratory studies were: HGB 10.5g/dL, WBC 27.1x10 9 /L (16 days off cyclophosphamide), Na135 mmol/L (135-145 mmol/L), K 5.2 mmol/L (3.6-5.2mmol/L), HCO3 19 mmol/L (22-29 mmol/L), Cl 103mmol/L (100-108 mmol/L), Cr 220 µmol/L (53-97 µmol/L),BUN 16 mmol/L (2-7 mmol/L). Ur<strong>in</strong>e (via a ur<strong>in</strong>ary catheter,<strong>as</strong> he w<strong>as</strong> oliguric on presentation, but reverted to be<strong>in</strong>g nonoliguricshortly after resuscitation) appeared concentrated butclear; microscopy showed RBC 4-10/HPF, WBC 31-40/HPF,<strong>an</strong>d negative gram sta<strong>in</strong>.He w<strong>as</strong> promptly volume resuscitated <strong>an</strong>d empirically startedon l<strong>in</strong>ezolid <strong>an</strong>d cefepime. His immunosuppress<strong>an</strong>ts werereplaced by stress-dose steroids. The provisional diagnosisw<strong>as</strong> septic shock. However, given the recent similar episodewhich w<strong>as</strong> temporally <strong>as</strong>sociated with the azathiopr<strong>in</strong>e<strong>in</strong>itiation (negative <strong>in</strong>fection work-up), <strong>an</strong>d the symptoms offever, headache, hypotension <strong>an</strong>d leukocytosis which hadbeen described <strong>in</strong> azathiopr<strong>in</strong>e-<strong>in</strong>duced <strong>an</strong>aphylactic shock 5,6 ,azathiopr<strong>in</strong>e reaction w<strong>as</strong> also suspected. St<strong>an</strong>dard<strong>in</strong>vestigations for <strong>in</strong>fection were undertaken. Blood <strong>an</strong>d ur<strong>in</strong>ecultures, CT of head <strong>an</strong>d abdomen, <strong>an</strong>d lumbar puncture allfailed to identify a source. To <strong>as</strong>certa<strong>in</strong> whether he had drug<strong>in</strong>duced<strong>an</strong>aphylactic shock, serum Trypt<strong>as</strong>e <strong>an</strong>d 24-hr ur<strong>in</strong>eN-Methylhistam<strong>in</strong>e <strong>an</strong>d 11β-Prostagl<strong>an</strong>d<strong>in</strong> F 2α were obta<strong>in</strong>ed,<strong>as</strong> m<strong>as</strong>sive elaboration of these v<strong>as</strong>oactive mediators bycirculat<strong>in</strong>g m<strong>as</strong>t cells is the hallmark feature of <strong>an</strong>aphylacticreaction 7 . His serum Trypt<strong>as</strong>e <strong>an</strong>d ur<strong>in</strong>e N-Methylhistam<strong>in</strong>ewere with<strong>in</strong> normal limits, 2.94 ng/mL (reference r<strong>an</strong>ge: 100 WBC/HPF (persisted after ur<strong>in</strong>arycatheter removal) without eos<strong>in</strong>ophiluria. Gram sta<strong>in</strong>s werenegative, <strong>an</strong>d he rema<strong>in</strong>ed without ur<strong>in</strong>ary symptoms. Repeatabdom<strong>in</strong>al CT <strong>an</strong>d ultr<strong>as</strong>onography were unremarkable.Given the persistent kidney dysfunction <strong>an</strong>d puzzl<strong>in</strong>g ur<strong>in</strong>emicroscopic f<strong>in</strong>d<strong>in</strong>gs, a diagnostic kidney biopsy w<strong>as</strong>obta<strong>in</strong>ed at day 5 after admission. The biopsy showedtubulo<strong>in</strong>terstitial dise<strong>as</strong>e with heavy <strong>in</strong>terstitial neutrophilic<strong>in</strong>filtrates (Figure 1A), slough<strong>in</strong>g of tubular epithelial cells(Figure 1B) <strong>an</strong>d numerous <strong>in</strong>tratubular microabscesses(Figure 1C). The glomeruli showed mild mes<strong>an</strong>gialexp<strong>an</strong>sion without endocapillary proliferation, necrosis orcrescents. Immunofluorescent sta<strong>in</strong><strong>in</strong>g <strong>an</strong>d electronmicroscopy confirmed background IgA nephropathy. Thesef<strong>in</strong>d<strong>in</strong>gs were consistent with acute pyelonephritis perimposed with tubular necrosis.Figure 1. Hematoxyl<strong>in</strong> <strong>an</strong>d eos<strong>in</strong> sta<strong>in</strong><strong>in</strong>g of the kidneybiopsy show<strong>in</strong>g.(A) Interstitial leukocyte <strong>in</strong>filtrates <strong>an</strong>d tubular <strong>in</strong>jury (10x).(B) An area of acute tubular damage with denudation oftubular epithelium, sloughed tubular epithelial cells (arrows),<strong>an</strong>d <strong>in</strong>terstitial PMN <strong>in</strong>filtrates (20x).(C) Tubular PMN c<strong>as</strong>ts/microabscesses (arrows) <strong>an</strong>d<strong>in</strong>terstitial PMN <strong>in</strong>filtrates (40x).
138 Jul 2010 Vol 3 No.3 North Americ<strong>an</strong> Journal of Medic<strong>in</strong>e <strong>an</strong>d ScienceIn light of the biopsy f<strong>in</strong>d<strong>in</strong>gs, he w<strong>as</strong> given <strong>an</strong> extended (6-week) course of cefprozil. He responded with a completeresolution of leukocyturia, <strong>an</strong>d a month later his serumcreat<strong>in</strong><strong>in</strong>e level returned to 106 µmol/L. He cont<strong>in</strong>ued regularfollow-up at our Out-Patient Cl<strong>in</strong>ic.DiscussionUTI/pyelonephritis is one of the most common <strong>in</strong>fections <strong>in</strong>immunocompromised hosts <strong>an</strong>d a major source of morbidity<strong>an</strong>d mortality. 2,3 Pathogenic Escherichia coli is by far themost common pathogen, account<strong>in</strong>g for the v<strong>as</strong>t majority ofUTIs. In our patient, although blood <strong>an</strong>d ur<strong>in</strong>e cultures werenegative (possibly related to <strong>an</strong>tibiotic exposure), his cl<strong>in</strong>ical<strong>an</strong>d laboratory presentations, kidney biopsy f<strong>in</strong>d<strong>in</strong>gs,response to <strong>an</strong>tibiotics, <strong>an</strong>d the absence of other causes forhis symptomatology (negative <strong>an</strong>aphylaxis workup) <strong>in</strong>dicatedthat he had septic shock secondary to bacterialpyelonephritis.UTI <strong>in</strong>clud<strong>in</strong>g pyelonephritis is the outcome of <strong>in</strong>teractionbetween the bacteria virulence characteristics <strong>an</strong>d the hostdefense mech<strong>an</strong>isms. Pathogenic Escherichia coli typicallyga<strong>in</strong> access to the g<strong>as</strong>tro<strong>in</strong>test<strong>in</strong>al tract, <strong>an</strong>d from there spreadto the ur<strong>in</strong>ary tract <strong>an</strong>d <strong>as</strong>cend to <strong>in</strong>vade kidneys.Pathogenic Escherichia coli adhere to the uroepitheliumthrough their surface molecule adhes<strong>in</strong> (hair-like projectionsalso termed p-fimbriae or pyelonephritis-<strong>as</strong>sociated pili).Adhes<strong>in</strong> also decre<strong>as</strong>es IgA tr<strong>an</strong>sport <strong>in</strong>to the ur<strong>in</strong>e result<strong>in</strong>g<strong>in</strong> a reduction of local host defense. 8 Althoughpolymorphonuclear cells (PMNs) do not possess adhes<strong>in</strong>receptor, they possess receptors b<strong>in</strong>d<strong>in</strong>g to <strong>an</strong>other group ofpili of Escherichia coli, type I pili. The b<strong>in</strong>d<strong>in</strong>g of PMNs <strong>an</strong>dtype I pili prevents bacteria adhesion to the uroepithelia.Although rare stra<strong>in</strong>s of Escherichia coli c<strong>an</strong> shed their pili 9thereby circumvent<strong>in</strong>g the effects of PMNs, <strong>in</strong> mostcircumst<strong>an</strong>ces, PMNs b<strong>in</strong>d bacteria <strong>an</strong>d protect hosts from<strong>in</strong>fection. The pathogen <strong>in</strong> the current c<strong>as</strong>e w<strong>as</strong> mostly likelyEscherichia coli, <strong>as</strong> numerous epidemiologic studies<strong>in</strong>dicat<strong>in</strong>g that they are the most common cause of UTI <strong>in</strong>immunocompromised hosts. 10With regard to the host defense, our patient had severaldeficiencies. First <strong>an</strong>d perhaps most import<strong>an</strong>t, he had beenunder heavy immunosuppression for 6 months. Drug-<strong>in</strong>ducedmarrow suppression prevented a robust leukemoid reaction tothe <strong>in</strong>fection. Second, secretory IgAs are known toparticipate <strong>in</strong> the ma<strong>in</strong>ten<strong>an</strong>ce of mucosal surface immunehomeost<strong>as</strong>is <strong>an</strong>d confer protection aga<strong>in</strong>st pathogencolonization. Secretory IgAs also c<strong>an</strong> neutralize bacteria PLS(import<strong>an</strong>t for Escherichia coli pathogenesis) <strong>in</strong>dependent ofgr<strong>an</strong>ulocyte cells or T-cells. Our patient had IgAnephropathy, which is pathogenetically related to defects <strong>in</strong>O-l<strong>in</strong>ked glycosylations. Such defects c<strong>an</strong> alter the chargecharacteristics of IgA1 molecules. IgA1 with <strong>in</strong>complete O-galactosylation also tends to self-aggregate, 9 thereby maydim<strong>in</strong>ish its physiological functions. Third, our patient h<strong>as</strong>diabetes, which is one of the metabolic factors known toenh<strong>an</strong>ce bacterial <strong>in</strong>v<strong>as</strong>iveness with<strong>in</strong> ur<strong>in</strong>ary tract <strong>in</strong>immune compromised hosts.Cl<strong>as</strong>sically, history <strong>an</strong>d physical exam<strong>in</strong>ation are essential <strong>in</strong>identify<strong>in</strong>g the existence <strong>an</strong>d source of <strong>in</strong>fection. In thispatient, although he appeared <strong>in</strong> shock, a diagnosis of<strong>in</strong>fection <strong>as</strong> <strong>an</strong> etiology of his presentation w<strong>as</strong> called <strong>in</strong>toquestion because (1) by history, he had been on TMP/SMXprophylaxis s<strong>in</strong>ce the start of the immunosuppressivetreatment <strong>an</strong>d he did not show <strong>an</strong>y focal (ur<strong>in</strong>ary) symptoms(might be related to the <strong>in</strong>sufficient local leukemoid reaction,at le<strong>as</strong>t <strong>in</strong>itially), <strong>an</strong>d (2) on exam<strong>in</strong>ation, he did not havefl<strong>an</strong>k pa<strong>in</strong> or abdom<strong>in</strong>al tenderness. This atypicalpresentation created a diagnostic dilemma.Immunosuppressive therapy c<strong>an</strong> m<strong>as</strong>k the cl<strong>in</strong>icalm<strong>an</strong>ifestations of <strong>in</strong>fection. Our patient did not haveleukocytosis at his <strong>in</strong>itial presentation to the local hospital,despite sepsis-like presentation. This is likely related to themarrow suppressive effect of cyclophosphamide. In l<strong>in</strong>e withthis <strong>as</strong>sumption, his serum leukocyte counts (<strong>an</strong>d ur<strong>in</strong>eleukocytes) were <strong>in</strong>cre<strong>as</strong>ed <strong>in</strong> the succeed<strong>in</strong>g days <strong>as</strong> moretime elapsed from the l<strong>as</strong>t dosage of cyclophosphamide,consistent with a gradual recovery of leukemoid response to<strong>in</strong>fection. Although the steroid adm<strong>in</strong>istration dur<strong>in</strong>g hishospital stay could have contributed to the leukocytosis, itw<strong>as</strong> unlikely to have been a major factor because theleukocytosis on admission preceded the <strong>in</strong>itiation of stressdosesteroids. Thus, the <strong>in</strong>itial lack of leucocytosis w<strong>as</strong> likelyrelated to drug-<strong>as</strong>sociated marrow suppression. Incidentally,this c<strong>as</strong>e also served to dispel the notion that patients onTMP/SMX prophylaxis would not be at risk for UTI. Ourpatient developed pyelonephritis while on TMP/SMX, <strong>an</strong>drecent studies also show that over 70% uropathogenicbacteria are <strong>in</strong>sensitive or resist<strong>an</strong>t to TMP/SMX 11 .Although <strong>in</strong>fection, given its potential fatality, should bedoggedly pursued, it is plausible to <strong>in</strong>clude multiplediagnostic considerations. The atypical presentations <strong>in</strong> thisc<strong>as</strong>e led to seek<strong>in</strong>g alternative expl<strong>an</strong>ations, such <strong>as</strong> pseudosepsisdue to drug reaction.Azathiopr<strong>in</strong>e is <strong>an</strong> imidazole derivative of 6-mercaptopur<strong>in</strong>e.The allergic-type reactions have been described <strong>as</strong> a rare <strong>an</strong>ddose-<strong>in</strong>dependent event occurr<strong>in</strong>g with<strong>in</strong> days to weeksfollow<strong>in</strong>g the drug <strong>in</strong>troduction. 6 The reactions c<strong>an</strong> r<strong>an</strong>gefrom p<strong>an</strong>creatitis, hepatitis, sk<strong>in</strong> r<strong>as</strong>h, fever, arthralgi<strong>as</strong>,malaise, diarrhea <strong>an</strong>d abdom<strong>in</strong>al pa<strong>in</strong> to <strong>an</strong>aphylactic shock.The <strong>an</strong>aphylactic reaction/shock is characterized by abruptonset of headache, fever, hypotension <strong>an</strong>d leukocytosis. 5,6Although our patient’s presentation fit well with thisdescription, his laboratory studies did not. In a typical<strong>an</strong>aphylactic reaction, circulat<strong>in</strong>g m<strong>as</strong>t cells are acutelyactivated, rele<strong>as</strong><strong>in</strong>g a host of v<strong>as</strong>oactive mediators <strong>in</strong>clud<strong>in</strong>gtrypt<strong>as</strong>e, histam<strong>in</strong>e, <strong>an</strong>d prostagl<strong>an</strong>d<strong>in</strong> D2. Serum <strong>an</strong>d ur<strong>in</strong>elevels of these mediators <strong>an</strong>d their metabolites, N-Methylhistam<strong>in</strong>e <strong>an</strong>d 11β-Prostagl<strong>an</strong>d<strong>in</strong> F 2α , are expected tobe m<strong>as</strong>sively <strong>an</strong>d simult<strong>an</strong>eously elevated. Our patient had <strong>an</strong>isolated elevation of 11β-Prostagl<strong>an</strong>d<strong>in</strong> F 2α , <strong>in</strong>consistent with<strong>an</strong>aphylactic reaction. 7 In fact, the isolated 11β-Prostagl<strong>an</strong>d<strong>in</strong>F 2α elevation (to the level comparable to that <strong>in</strong> our patient)c<strong>an</strong> be seen <strong>in</strong> physiologic conditions dur<strong>in</strong>g normal labor 12or sleep 13 . Under these circumst<strong>an</strong>ces 11β-Prostagl<strong>an</strong>d<strong>in</strong> F 2α
North Americ<strong>an</strong> Journal of Medic<strong>in</strong>e <strong>an</strong>d Science Jul 2010 Vol 3 No.3 139is rele<strong>as</strong>ed from tissues rather th<strong>an</strong> from circulat<strong>in</strong>g m<strong>as</strong>tcells. Thus, the isolated 11β-Prostagl<strong>an</strong>d<strong>in</strong> F 2α elevation <strong>in</strong>this c<strong>as</strong>e c<strong>an</strong> not be attributed to <strong>an</strong>aphylactic reaction.Recently, rare c<strong>as</strong>es of acute allergic <strong>in</strong>terstitial nephritishave been described <strong>in</strong> patients tak<strong>in</strong>g azathiopr<strong>in</strong>e 14,15 . Suchreaction is <strong>as</strong>sociated with sk<strong>in</strong> r<strong>as</strong>h <strong>an</strong>d tr<strong>an</strong>sienthypocomplementemia, <strong>an</strong>d kidney biopsy showsmonocytic/lymphocytic <strong>in</strong>filtration mixed with prom<strong>in</strong>enteos<strong>in</strong>ophiles. Our patient had neither r<strong>as</strong>h norhypocomplementemia; his kidney biopsy showed PMNpredom<strong>in</strong><strong>an</strong>ce <strong>an</strong>d numerous microabscesses, <strong>in</strong>consistentwith <strong>an</strong> allergic type reaction. The kidney biopsy <strong>in</strong> our c<strong>as</strong>ehelped to resolve the diagnostic dilemma <strong>an</strong>d to design atherapeutic pl<strong>an</strong>.ConclusionDiagnos<strong>in</strong>g <strong>in</strong>fection <strong>in</strong> patients with immunosuppressionc<strong>an</strong> be exceed<strong>in</strong>gly challeng<strong>in</strong>g. Medications such <strong>as</strong>azathiopr<strong>in</strong>e c<strong>an</strong> cause a cl<strong>in</strong>ical picture mimick<strong>in</strong>g septicshock. When <strong>in</strong>fection is suspected <strong>an</strong>d st<strong>an</strong>dard evaluationfails to identify a source, additional <strong>in</strong>vestigations (i.e.,kidney biopsy <strong>in</strong> this c<strong>as</strong>e) not rout<strong>in</strong>ely conducted <strong>in</strong> nonimmunocompromisedhosts may be <strong>in</strong>dicated to facilitatediagnosis <strong>an</strong>d m<strong>an</strong>agement.ConsentWritten <strong>in</strong>formed consent w<strong>as</strong> obta<strong>in</strong>ed from the patient for publication ofthis c<strong>as</strong>e report.Compet<strong>in</strong>g InterestsThe authors declare that they have no compet<strong>in</strong>g <strong>in</strong>terests.Authors' contributionsQQ w<strong>as</strong> <strong>in</strong>volved <strong>in</strong> patient care <strong>an</strong>d m<strong>an</strong>uscript writ<strong>in</strong>g. MHS contributedto the literature review <strong>an</strong>d the m<strong>an</strong>uscript writ<strong>in</strong>g, <strong>an</strong>d SS to the kidneyhistological exam<strong>in</strong>ation <strong>an</strong>d m<strong>an</strong>uscript writ<strong>in</strong>g. All authors read <strong>an</strong>dapproved the f<strong>in</strong>al m<strong>an</strong>uscript.References1. S<strong>in</strong>gh N. Infectious complications <strong>in</strong> org<strong>an</strong> tr<strong>an</strong>spl<strong>an</strong>t recipients withthe use of calc<strong>in</strong>eur<strong>in</strong>-<strong>in</strong>hibitor agent-b<strong>as</strong>ed immunosuppressiveregimens. Current op<strong>in</strong>ion <strong>in</strong> <strong>in</strong>fectious dise<strong>as</strong>es. 2005;18(4):342-345.2. Valera B, Gentil MA, Cabello V, Fijo J, Cordero E, Cisneros JM.Epidemiology of ur<strong>in</strong>ary <strong>in</strong>fections <strong>in</strong> renal tr<strong>an</strong>spl<strong>an</strong>t recipients.Tr<strong>an</strong>spl<strong>an</strong>t Proc. 2006;38(8):2414-2415.3. Saem<strong>an</strong>n M, Horl WH. Ur<strong>in</strong>ary tract <strong>in</strong>fection <strong>in</strong> renal tr<strong>an</strong>spl<strong>an</strong>trecipients. Eur J Cl<strong>in</strong> Invest. 2008;38 Suppl 2:58-65.4. Angus DC, L<strong>in</strong>de-Zwirble WT, Lidicker J, Clermont G, Carcillo J,P<strong>in</strong>sky MR. Epidemiology of severe sepsis <strong>in</strong> the United States:<strong>an</strong>alysis of <strong>in</strong>cidence, outcome, <strong>an</strong>d <strong>as</strong>sociated costs of care. Crit CareMed. 2001;29(7):1303-1310.5. Demirt<strong>as</strong>-Ert<strong>an</strong> G, Rowsh<strong>an</strong>i AT, ten Berge IJ. Azathiopr<strong>in</strong>e-<strong>in</strong>ducedshock <strong>in</strong> a patient suffer<strong>in</strong>g from undifferentiated erosive oligoarthritis.Neth J Med. 2006;64(4):124-126.6. Rosenthal E. Azathiopr<strong>in</strong>e shock. Postgrad Med J 1986;62(729):677-678.7. V<strong>an</strong> Toorenenbergen AW, Or<strong>an</strong>je AP. Comparison of serum trypt<strong>as</strong>e<strong>an</strong>d ur<strong>in</strong>e N-methylhistam<strong>in</strong>e <strong>in</strong> patients with suspected m<strong>as</strong>tocytosis.Cl<strong>in</strong> Chim Acta. 2005;359(1-2):72-77.8. Plos K, Connell H, Jodal U, et al. Intest<strong>in</strong>al carriage of P fimbriatedEscherichia coli <strong>an</strong>d the susceptibility to ur<strong>in</strong>ary tract <strong>in</strong>fection <strong>in</strong>young children. J Infect Dis. 1995;171(3):625-631.9. Sobel JD. Pathogenesis of ur<strong>in</strong>ary tract <strong>in</strong>fections. <strong>Host</strong> defenses.Infect Dis Cl<strong>in</strong> North Am. 1987;1(4):751-772.10. Johnson JR. From <strong>Pyelonephritis</strong> <strong>an</strong>d Abscesses of the Kidney. InInfectious Dise<strong>as</strong>es. 2nd Edition. Edited by Jonath<strong>an</strong> Cohen <strong>an</strong>dWilliam G. Powderly M. Ed<strong>in</strong>burgh: Mosby; 2004, pp. 753-762.11. Di Cocco P, Orl<strong>an</strong>do G, Mazzotta C, et al. Incidence of ur<strong>in</strong>ary tract<strong>in</strong>fections caused by germs resist<strong>an</strong>t to <strong>an</strong>tibiotics commonly used afterrenal tr<strong>an</strong>spl<strong>an</strong>tation. Tr<strong>an</strong>spl<strong>an</strong>t Proc. 2008;40(6):1881-1884.12. Berrym<strong>an</strong> GK, Strickl<strong>an</strong>d DM, H<strong>an</strong>k<strong>in</strong>s GD, Mitchell MD. Amnioticfluid prostagl<strong>an</strong>d<strong>in</strong> D2 <strong>in</strong> spont<strong>an</strong>eous <strong>an</strong>d augmented labor. Life Sci.1987;41(13):1611-1614.13. Hayaishi O. Molecular mech<strong>an</strong>isms of sleep-wake regulation: a role ofprostagl<strong>an</strong>d<strong>in</strong> D2. Philos Tr<strong>an</strong>s R Soc Lond B Biol Sci. 2000;355:275-280.14. Bir K, Herzenberg AM, Carette S. Azathiopr<strong>in</strong>e <strong>in</strong>duced acute<strong>in</strong>terstitial nephritis <strong>as</strong> the cause of rapidly progressive renal failure <strong>in</strong> apatient with Wegener's gr<strong>an</strong>ulomatosis. J Rheumatol. 2006;33(1):185-187.15. Re<strong>in</strong>hold-Keller E, Schmitt WH, Gross WL. Azathiopr<strong>in</strong>e toxicitymimick<strong>in</strong>g a relapse of Wegener's gr<strong>an</strong>ulomatosis. Rheumatology(Oxford). 2001;40(7):831-832.













