Criminal justice liaison and diversion schemes - Offender Health ...
Criminal justice liaison and diversion schemes - Offender Health ...
Criminal justice liaison and diversion schemes - Offender Health ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Mental health briefing September 2008<strong>Criminal</strong> <strong>justice</strong> <strong>liaison</strong> <strong>and</strong><strong>diversion</strong> <strong>schemes</strong>: A focuson women offendersIntroductionAgainst the backdrop of a rapidly increasing female prison population <strong>and</strong>concern at the significant number of women with mental health problems heldin custody, criminal <strong>justice</strong> <strong>liaison</strong> <strong>and</strong> <strong>diversion</strong> (CJLD) <strong>schemes</strong> have beentasked with diverting offenders* with mental health needs away from thecriminal <strong>justice</strong> system into the care of health <strong>and</strong> social services. Thisbriefing paper presents key findings from an evaluation conducted betweenJanuary 2006 <strong>and</strong> March 2007 of 10 CJLD <strong>schemes</strong>. The evaluation aimed toprovide a qualitative <strong>and</strong> quantitative description of the <strong>schemes</strong> <strong>and</strong> theextent <strong>and</strong> nature of the service they provided for women offenders withmental health needs.Contents Introduction page 1 The <strong>schemes</strong> page 3 CJLD <strong>schemes</strong>’ datafindings page 8 Recommendationspage 10Written by:Gillian Hunter Institutefor <strong>Criminal</strong> PolicyResearchIsabella Boyce Institutefor <strong>Criminal</strong> PolicyResearchLucy Smith NacroThree areas were addressed by the evaluation:The extent to which CJLD <strong>schemes</strong> were able to contact women offenderswith mental health needs.The extent to which <strong>schemes</strong> provided access to support <strong>and</strong> treatment toenable women to remain in the community rather than receive a custodialsentence.The factors that helped or hindered CJLD <strong>schemes</strong> in their task ofidentifying <strong>and</strong> supporting women offenders with mental health needs.The <strong>schemes</strong> included in the evaluation reflect different types of <strong>liaison</strong> <strong>and</strong><strong>diversion</strong> services. They were located in police stations <strong>and</strong> magistrates’courts, rural <strong>and</strong> urban locations, include <strong>schemes</strong> with <strong>and</strong> withoutpsychiatric input <strong>and</strong> those which used proactive <strong>and</strong> reactive methods ofworking (checking for evidence of mental health problems or relying oncustody staff <strong>and</strong> other criminal <strong>justice</strong> practitioners to make referrals).For each scheme the evaluation:reviewed operational policies <strong>and</strong> protocols, where availablewww.nacromentalhealth.org.ukwww.nacro.org.ukNacro 2008compiled socio-demographic <strong>and</strong> an assessment outcome data profile foroffenders assessed by the scheme (based on routine monitoring <strong>and</strong> casefile data for 2005)collated information about multi-agency involvement to map local serviceprovision <strong>and</strong> examine the links between the scheme <strong>and</strong> other agenciesconducted interviews with key professionals (scheme staff <strong>and</strong> others frompolice, courts, probation <strong>and</strong> receiving services) <strong>and</strong> women service usersNacroPark Place, 10-12 Lawn Lane,London SW8 1UDTelephone 020 7840 1209Fax 020 7840 1213Email mentalhealth@nacro.org.ukNacro is a registered charity no. 226171placed scheme activity in context through examination of local arrest <strong>and</strong>sentencing data.* This briefing paper has used the term ‘offenders’, but includes those who come into contact with the criminal <strong>justice</strong> systembecause they are suspected of committing an offence.1
<strong>Criminal</strong> <strong>justice</strong> <strong>liaison</strong> <strong>and</strong> <strong>diversion</strong> <strong>schemes</strong>: A focus on women offendersPolicy contextDiverting offenders with mental health needsaway from the criminal <strong>justice</strong> system into thecare of health <strong>and</strong> social services has been apolicy aim for some time. 1-3 As far back as 1992,the Reed Review of <strong>Health</strong> <strong>and</strong> Social Services forMentally Disordered <strong>Offender</strong>s (the Reed report)recommended that there should be nationwideprovision of properly resourced court assessment<strong>and</strong> <strong>diversion</strong> <strong>schemes</strong> to achieve this goal.Prison exacerbates mental ill health, heightensvulnerability <strong>and</strong> increases the risk of self-harm<strong>and</strong> suicide. In addition, mental health serviceswithin prison are unsuitable <strong>and</strong> inadequate fordealing with prisoners with chronic <strong>and</strong> severemental health conditions. 4-7 Recent developmentsin this area include a government review ofservices for offenders with mental health needsconducted by Lord Keith Bradley, <strong>and</strong> theforthcoming publication in 2009 of the firstoffender healthcare strategy. 8 There are alsoefforts afoot to improve <strong>and</strong> st<strong>and</strong>ardise theprovision of court assessment, <strong>liaison</strong> <strong>and</strong><strong>diversion</strong> services through the introduction ofservice level agreements (SLA) betweenmagistrates’ courts <strong>and</strong> mental health services.Pilot projects using SLAs are currently beingundertaken in the south-west of Engl<strong>and</strong> <strong>and</strong>north-west London.*Baroness Corston conducted a review of vulnerablewomen in the criminal <strong>justice</strong> system. 9 Thishighlighted the failure of the NHS to properlyresource <strong>schemes</strong> to divert women with mentalhealth needs away from prison <strong>and</strong> intocommunity-based healthcare. The Women’sOffending Reduction Programme (WORP) sought todevelop more appropriate communityinterventions for women to encourage their<strong>diversion</strong> at pre-court <strong>and</strong> pre-sentence stages ofthe criminal process <strong>and</strong> the greater use ofcommunity disposals. 10 In addition, the GenderEquality Duty (April 2007) placed a legal obligationon public bodies to show that they werepromoting equality of opportunity between men<strong>and</strong> women through the Equality Act 2006. Theimplications for criminal <strong>justice</strong> agencies includedrecognising <strong>and</strong> catering for the potentiallydifferent needs of male <strong>and</strong> female offenders. 11,12What we know about the femaleoffending populationMost female prisoners are serving short sentencesfor non-violent crimes <strong>and</strong> over a third have noprevious convictions. 13 The majority (66%) are* For more details contact <strong>Offender</strong> <strong>Health</strong> at the Department of <strong>Health</strong>.mothers, 14 yet the small size of the female prisonestate means that many are held far from homemaking it difficult to maintain regular family ties,which can have damaging consequences for theirchildren <strong>and</strong> for the women’s mental health.Ensuring that community-based disposals areavailable wherever possible for women withmental health issues could help to reduce thenumber serving these short prison sentences. 9Mental ill health is high among women offenders.Female prisoners are twice as likely as males tohave had contact with mental health servicesprior to their imprisonment. They are also morelikely than male prisoners to suffer fromfunctional psychosis <strong>and</strong> neurotic disorders suchas depression, anxiety <strong>and</strong> phobias. Two-thirds ofwomen prisoners have been assessed as having aneurotic disorder. 15 Approximately 50% of womenprisoners were receiving prescribed medicationsuch as anti-depressants <strong>and</strong> anti-psychoticmedicine. 15 A more recent study has reported thatwomen in custody were five times more likely tohave a mental health problem than women in thegeneral population. 9Nearly a third of women prisoners self-harmed in2003 compared to only 6% of men, <strong>and</strong> whilewomen comprise a minority (6%) in the prisonpopulation, they accounted for 46% of all selfharmincidents. 16 Furthermore, nearly half offemale rem<strong>and</strong> prisoners had attempted suicidein their lifetime compared to a quarter of malerem<strong>and</strong> prisoners. 17 There were 54 self-inflicteddeaths of women prisoners between 2000 <strong>and</strong>2005 <strong>and</strong> the majority of prisoners who commitor attempt suicide have a history of mental13, 18disorder.Substance misuse is common, with femaleprisoners more likely than men to be dependenton opiates. 15 In a sample of 301 women from 10prisons, 34% reported hazardous levels ofdrinking in the year before prison <strong>and</strong> 43%reported use of crack cocaine <strong>and</strong> 44% use ofheroin in that time frame. Over a quarter (27%)had used heroin <strong>and</strong> 9% had used crack cocainewhile in prison. 19 Unsurprisingly, there is also ahigh degree of comorbidity: one study found that83% of female rem<strong>and</strong> prisoners <strong>and</strong> 70% offemale sentenced prisoners had two or moremental disorders. 15 Other issues includeexperience of violence: 50% of women prisonershave experienced domestic violence <strong>and</strong> about athird have been sexually abused. 132
Mental health briefing 2008Linking with women’s prisonsA common problem was the relatively poor links<strong>schemes</strong> had with women’s prisons. Two relatedissues were noted: the geographic dispersal of thewomen’s estate meant it was often impractical toarrange visits <strong>and</strong> the infrequency of contactmade it difficult to build up workingrelationships with prison health teams. This hasimplications for transferring mental healthassessment information from the scheme to theprison <strong>and</strong> vice versa on release. Although thereare st<strong>and</strong>ard procedures for the notification of aprisoner’s risk of suicide <strong>and</strong> self-harm, otherinformation about mental health may be lost.Scheme 9 had appointed a prison link worker forwomen. Her role was to ensure continuity of care<strong>and</strong> access to services on leaving prison. She alsotried to help women stay in contact with families<strong>and</strong> carers through practical help such asarranging transport for visits.Guidance <strong>and</strong> trainingDespite the emphasis on guidance <strong>and</strong> trainingfor those working with women offenders withmental health needs, 10, 21 only two <strong>schemes</strong>reported receiving any gender-specific training<strong>and</strong> this was focused on self-harm. None of the<strong>schemes</strong> had received guidance on dealing witheating disorders or sexual abuse.User involvementThere is an increasing emphasis on the centralityof the service user in mental health policy 21 <strong>and</strong>regular consultation with service users isrecommended as a routine factor in serviceplanning. 23 None of the <strong>schemes</strong> in our samplehad any routine procedures for collating feedbackfrom their service users or any recent findingsfrom user consultations. Our own limitedendeavours show that it was difficult for thewomen to differentiate the service input they hadfrom different health <strong>and</strong> criminal <strong>justice</strong>agencies, which has implications for any futuremethods <strong>schemes</strong> may use to collect serviceusers’ opinions. The interviews we undertookwith service users (11 in all) did however showthat women were generally positive about theservice provided by the <strong>schemes</strong> <strong>and</strong> gainedvaluable help <strong>and</strong> support from the receivingagencies. The following interview extracts showthe importance the women placed on havingsomeone at court or in the police station who hadtime to listen to their concerns <strong>and</strong> who hadsome underst<strong>and</strong>ing of what they were goingthrough:‘I thought it helped me more, because thenother people get to underst<strong>and</strong> from mypoint of view, rather than just going inthere <strong>and</strong> they don’t underst<strong>and</strong> everything,I mean, at least people then have, youknow, realise reasons why you get yourselfinto trouble… if I could kiss that man, Iwould, from the [CJLD scheme], you know, Iwould, he done wonders for me… <strong>and</strong> heactually sat down <strong>and</strong> he listened to me,you don’t get many people like that.’Wilma, 23 years old‘Just being able to go in <strong>and</strong> speak aboutanything really <strong>and</strong> knowing that it ain’tgoing to go any further. It’s private <strong>and</strong>confidential. Nobody else needs to knowabout it. He’s always saying, it stays in theroom that we’re in. It’s just nice to knowthat he’s not in judgement.’Emily, 24 years oldBelow, Gale, 25 years old, describes her situationbefore <strong>and</strong> after intervention by the CJLD schemewhich led to a transfer to a mental health facility:‘I feel better here [in the secure unit]because in jail I had the voices really bad<strong>and</strong> I was trying to pretend to everybody Iam all right. I was making a joke with itbecause me voices kept saying ‘out thewindow’ <strong>and</strong> I said ‘you’re telling me to goout the window’ <strong>and</strong> I was making a joke ofit. And I was making out I was all right toeveryone because I didn’t want anyonetaking the piss out of me… And I had neverbeen to jail before so I was trying to makeout I was all right when I wasn’t. Where hereI have been able to get better <strong>and</strong> tell thetruth.’ResourcesAs a general point, all the <strong>schemes</strong> talked aboutoperating with very limited resources. Thefollowing extract from an interview with asteering group chair <strong>and</strong> commissioner offorensic services is used to illustrate the issuesfaced by many <strong>schemes</strong>:‘It’s way under capacity… it’s very difficultto keep it on the commissioning agendabecause you are going through this tieringon the commissioning side. You are in there7
<strong>Criminal</strong> <strong>justice</strong> <strong>liaison</strong> <strong>and</strong> <strong>diversion</strong> <strong>schemes</strong>: A focus on women offenderswith all the other service programmes, likecancer, like heart diseases, all the other bits<strong>and</strong> pieces… They all get dealt with first.Mental health comes way down thecommissioning list <strong>and</strong> within mentalhealth you have all those targets that youare performance-managed… Court <strong>diversion</strong>has not appeared in that. It barely got amention in the criminal <strong>justice</strong> carepathway… never mind a target.’CJLD <strong>schemes</strong>’ datafindingsData qualityWe collated local police arrest <strong>and</strong> sentencingdata <strong>and</strong> scheme monitoring data from 2005 toprovide an indication of the need for CJLD<strong>schemes</strong> for women offenders in different areas.From the outset it was clear that the extent <strong>and</strong>quality of routine monitoring data would vary. Anearlier Nacro survey 22 found that one in five<strong>schemes</strong> did not collect service level activity data,while two-fifths did not record details of clients’gender. As anticipated, much of this activity datawas paper-based.The quality <strong>and</strong> consistency of activity data wasgenerally poor <strong>and</strong> monitoring systems wereinadequate. The minimum data set proposed forthis study (see Box 2, page 11) representedcommon core data that were available across the<strong>schemes</strong>, according to screening <strong>and</strong> assessmenttools. However, only four <strong>schemes</strong> routinelytransferred these data onto an electronicdatabase, three had no electronic data at all, twogave us partial electronic data <strong>and</strong> one schemecould provide no activity data. As a result, theproportion of missing data was high, particularlyon items such as primary diagnosis <strong>and</strong> referralrecommendations. <strong>Criminal</strong> <strong>justice</strong> outcomeswere not easily available at eight of the <strong>schemes</strong>.Likewise, the outcome of referrals to communityservices were not recorded routinely.This meant that we were unable to draw anyconclusions about the recommendations made tothe court by CJLD <strong>schemes</strong> for women offenders<strong>and</strong> the proportion of recommendations taken upby courts, or the proportion of successfulreferrals from CJLD of women to hospital <strong>and</strong>community-based mental health services <strong>and</strong>criminal <strong>justice</strong> system interventions. Thesekinds of outcome data were not recordedroutinely by most <strong>schemes</strong>, making it very hardto judge the effectiveness of the <strong>schemes</strong>. Whatwe can say about the CJLD contacts <strong>and</strong> referralsources is limited. This dearth of monitoring datais an important finding in its own right.Nature <strong>and</strong> extent of contact byCJLD <strong>schemes</strong>We can say that the <strong>schemes</strong> were seeing onaverage 2% to 3% of the total number of offenderspassing through the police station <strong>and</strong> courts.This suggests a considerable level of unmet need.Surveys of the offender population haveconsistently found a high proportion with mentalhealth problems. 15There were 2,155 adult referrals to the nine CJLD<strong>schemes</strong> between January <strong>and</strong> December 2005,ranging from 16 to 688 referrals per scheme (themean was 239). Around three-quarters of referralsduring this period were made via police custody(n=1,123; 52%), probation (n=289; 13%) or thecourts (n=192; 9%).Four <strong>schemes</strong> operated at the police station. *Between January <strong>and</strong> December 2005 these policeforce areas came into contact with a total of49,666 arrestees. During the same period theCJLD <strong>schemes</strong> received 1,492 referrals, but notsolely from custody suites – equivalent to 3% ofthe arrestee population at these sites. The rate ofcontact was similar for female suspects (3.5%).The level of contact with the arrestee populationvaried by area from 4.7% in Scheme 9 to 1.4% inScheme 10.At all nine CJLD sites it was possible to gathercomparable data on court activity (though onlysix operated as court-based <strong>schemes</strong>). During2005, 85,893 defendants were sentenced by thecourts. The <strong>schemes</strong> in these areas received 2,155referrals – equivalent to 2.5% of the populationprocessed by the courts. As with the arresteedata, the rate of contact was almost identical forfemale defendants (2.6%), but with the level ofcontact varying considerably between areas, from0.8% in Scheme 1 to 4.9% in Scheme 7, thisscheme also engaged the highest proportion offemale defendants (7.7%).The most common reasons for making a referralwere unspecified mental health concerns (n=500),* Two <strong>schemes</strong> operated both at the police station <strong>and</strong> at the court stage.8
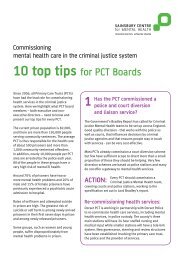
Mental health briefing 2008Table 2 Primary diagnosis for CJLD referrals requiring furtherintervention (%) (n=1146)35 32%16%3025201513%11% 11%1056%5%3%2% 2%1%0Substance useSerious <strong>and</strong> enduringmental illnessDepressionOtherPersonality disorderNo diagnosisLow level mentalhealth needsDual diagnosisLearning disabilityMissingSelf-harmself-harming (n=355), substance use (n=28) orother reasons (n=184). * The available activitydata from the nine sites suggests that less thanone-third (n=648) of those referred to CJLD<strong>schemes</strong> during 2005 had previous contact withpsychiatric services. ** In some cases CJLDworkers completed a full assessment with thereferrals they saw (n=820; 38%); however, wecannot be certain of the extent to which thishappened, as details on the type of assessmentundertaken were often missing.Over half the adults referred to the CJLD <strong>schemes</strong>were assessed as requiring further intervention(n=1146; 53%). *** Table 2 illustrates how substanceuse (n=362), SEMI (serious <strong>and</strong> enduring mentalillness, such as schizophrenia <strong>and</strong> bipolar/manicdepressive psychosis) (n=187) <strong>and</strong> depression(n=142) were the most common forms of primary* The reason for referral was not recorded in 51% of cases (n=1089).** Data on previous contact with psychiatric services was not recorded in 44%of cases (n=956).*** Data on referral recommendations were missing (including not known <strong>and</strong>not assessed) in 25% of cases (n=545).diagnosis made by CJLD workers followingassessment of need. The high rate of CJLDreferrals being identified with substance misuseproblems indicates some duplication of effort orthe potential for dual diagnosis of substancemisuse <strong>and</strong> mental health problems. Thisreinforces the need to establish links betweenCJLD <strong>schemes</strong> <strong>and</strong> DARS.How did the women seen by theCJLD <strong>schemes</strong> differ from the men?It is important to consider whether women’sexperiences of the CJLD <strong>schemes</strong> differed frommen’s <strong>and</strong> to underst<strong>and</strong> what factors wereimportant in shaping these experiences. Therewere a limited number of variables, for which wehad reasonable data, which we could hypothesiseas being potentially important factors (see Table 3overleaf).The women seen by the <strong>schemes</strong> were more likelythan men to be white; to have beenarrested/charged with a public order or violentoffence (but not section 136 detainees); <strong>and</strong>, to9
<strong>Criminal</strong> <strong>justice</strong> <strong>liaison</strong> <strong>and</strong> <strong>diversion</strong> <strong>schemes</strong>: A focus on women offendersTable 3 Female <strong>and</strong> male contactsseen by the CJLD <strong>schemes</strong>FemaleEthnicity (white) 96%(361/377)Marital status(single)74%(218/293)Homeless 14%(24/167)Has previousconvictions65%(107/166)Violent offender 17%(55/325)Male91%(1481/1637)79%(1132/1436)17%(133/766)80%(544/681)14%(193/1369)RecommendationsBelow we outline some recommendations, basedon our research, for how <strong>schemes</strong> might improvetheir service for women offenders with mentalhealth problems.ResourcesThe <strong>schemes</strong> are clearly under-resourced <strong>and</strong>the entire criminal <strong>justice</strong> system wouldbenefit from greater investment in them. Theirprofile might be raised if <strong>schemes</strong> weredirectly commissioned by primary care trusts<strong>and</strong> had clear performance targets from theDepartment of <strong>Health</strong>. For this to happen thereneeds to be good evidence about throughputs<strong>and</strong> impact, <strong>and</strong> this information will only beavailable if there is investment in theadministrative infrastructure of CJLD <strong>schemes</strong>.Public orderoffenderSection 136detaineeHas previouscontact withmental healthservicesMental healthneed (SEMI)Substancemisuse problem15%(50/325)9%(116/1369)1% (3/325) 1%(10/1369)94%(149/159)8%(25/325)38%(125/325)93%(498/537)14%(194/1371)29%(394/1371)Providing services for a higher proportion ofthose in need is in part a question ofresources. The <strong>schemes</strong> simply do not havethe capacity to provide sufficient coverage.However, a higher proportion of thepopulation in need could be located if<strong>schemes</strong>’ times of operation were more closelysynchronised with the times of peak dem<strong>and</strong>,such as evenings <strong>and</strong> weekends.If more resources were made available, CJLD<strong>schemes</strong> should aim for a more proactiveworking style by, for example, checkingcustody records <strong>and</strong> prisoner escort recordforms for evidence of mental health issues<strong>and</strong>/or previous contact with mental healthservices, rather than relying on referrals fromcustody staff.have been diagnosed with a substance use issue.They were less likely to have previous convictionsor have been diagnosed with SEMI than their malecounterparts. This is in contrast to researchshowing a higher prevalence of mental illness(including psychosis) among female prisonerscompared to male prisoners, 15 <strong>and</strong> suggests somedegree of unmet need <strong>and</strong> missed opportunities forthe mental health screening of women in contactwith the criminal <strong>justice</strong> system.Informed gender practiceProactive screening may be particularlyimportant for identifying women with mentalhealth problems because they may be lessobvious to the non-specialist. However, womenwho appear challenging can also be extremelyvulnerable.Wherever possible, the service user shouldhave the choice of speaking with a femalemember of staff. Schemes could encouragethe recruitment of female staff by offering,for example, job shares <strong>and</strong> part-timeappointments.10
Mental health briefing 2008Box 2Recommended minimumdata setDate of referral <strong>and</strong> assessmentAge, sex <strong>and</strong> ethnicity of clientSource of referral (eg, police, court, probation)Improving working relationships <strong>and</strong>communication between the <strong>schemes</strong> <strong>and</strong>prison inreach teams in female prisons is alsoa priority. Initially, this may simply be a matterof establishing links with other CJLD <strong>schemes</strong>to ensure a local (to the prison) team canprovide support to the offender until they arereleased <strong>and</strong> move back to their area ofresidence.Housing, employment <strong>and</strong> relationship status ofclientCJLD scheme staff should also be aware of anygender equality strategy produced by theiragencies under the Gender Equality Duty (April2007).If more resources are made available, thenthese should be deployed in a way thatpermits more gender-specific workingpractices. This should include training forscheme staff on women’s mental health <strong>and</strong>other needs <strong>and</strong> the profile of womenoffenders.Partnership workingCurrent offence <strong>and</strong> previous convictionsReason for referralPrevious contact with mental health servicesPrimary diagnosisReferral recommendations<strong>Criminal</strong> <strong>justice</strong> outcomeThere is clearly a need to improve <strong>and</strong>formalise links between the CJLD <strong>schemes</strong> <strong>and</strong>DARS <strong>and</strong> these links could be developed tobetter cater for those offenders with mentalhealth <strong>and</strong> substance misuse problems. Links with community-based services couldalso be improved. Signposting is limited <strong>and</strong>thus developing more formal referral linkswith appropriate local agencies (including thevoluntary sector) could result in betterattendance at follow-up services in thecommunity among CJLD clients. Schemesshould map out women’s organisations thatoffer counselling, women’s centres, womenonlyhostels, supported accommodation <strong>and</strong>drug projects, crisis centres <strong>and</strong> services thatengage with sex workers. The Griffin Society *has a resources database which may be useful.Any gaps that exist in provision, for example alack of women-only inpatient facilities, shouldbe raised with commissioners.Performance monitoring The minimum data set defined for this studyto monitor scheme activity (set out in Box 2above) could be achieved easily (all the<strong>schemes</strong> collected these data as part of routinescreening <strong>and</strong> assessment procedures) ifresources were available for administrativesupport, including database construction <strong>and</strong>management.User engagement Strategies for user engagement are at arudimentary level <strong>and</strong> should be developed.Publicity The work of the CJLD <strong>schemes</strong> needs to bepublicised via leaflets <strong>and</strong> posters at policestations <strong>and</strong> in courts <strong>and</strong> given to defencesolicitors to ensure that all criminal <strong>justice</strong>professionals, offenders <strong>and</strong> detainees areaware of the services they provide.* www.thegriffinsociety.org11
<strong>Criminal</strong> <strong>justice</strong> <strong>liaison</strong> <strong>and</strong> <strong>diversion</strong> <strong>schemes</strong>: A focus on women offendersReferences1 Reed J (1992) Review of <strong>Health</strong> <strong>and</strong> Social Services for Mentally Disordered<strong>Offender</strong>s <strong>and</strong> Others Requiring Similar Services London: HMSO.2 Home Office (1990) Circular 66/90 Provision for Mentally Disordered<strong>Offender</strong>s London: Home Office.3 Home Office (1995) Circular 12/95 Mentally Disordered <strong>Offender</strong>s: Interagencyworking London: HMSO.4 Edgar K (2004) Lacking Conviction: The rise of the women’s rem<strong>and</strong>population London: Prison Reform Trust.5 Department of <strong>Health</strong> (2005) <strong>Offender</strong> Mental <strong>Health</strong>care Pathway London:Department of <strong>Health</strong>.6 Sainsbury Centre (2006) London’s Prison Mental <strong>Health</strong> Services: A reviewLondon: The Sainsbury Centre.7 Care Services Improvement Partnership (2006) Women at Risk: The mentalhealth of women in contact with the judicial system London: Department of<strong>Health</strong>.8 Department of <strong>Health</strong> (2007) Improving <strong>Health</strong>, Supporting Justice: Aconsultation London: Department of <strong>Health</strong>.9 Baroness Jean Corston (2007) The Corston Report London: Home Office.10 Home Office (2004) Women’s Offending Reduction Programme Action PlanLondon: Home Office.11 Fawcett Society (2006) Doing Your Duty: Guide to the Gender Equality Duty,London: Fawcett Society.12 Fawcett Society (2006) Underst<strong>and</strong>ing Your Duty: Report on the GenderEquality Duty <strong>and</strong> the criminal <strong>justice</strong> system London: Fawcett Society.13 Howard League for Penal Reform (2006) Prison Information Bulletin 2:Women <strong>and</strong> girls in the penal system London: Prison Reform Trust.14 Women’s Estate Policy Unit (2003) Working with Women Prisoners London:Prison Service.15 Singleton N, Meltzer H, Gatward R, Coid J <strong>and</strong> Deasy D (1998) PsychiatricMorbidity Among Prisoners in Engl<strong>and</strong> <strong>and</strong> Wales London: The StationeryOffice.16 Rickford D (2003) Troubled Inside: Responding to the mental health needs ofwomen in prison London: Prison Reform Trust.17 Meltzer H, Jenkins R, Singleton N, Charlton J <strong>and</strong> Yar M (2003) ‘Non-fatalsuicide behaviour among prisoners’ International Review of Psychiatry, 15,pp. 148-149.18 Shaw J, Appleby L <strong>and</strong> Baker D (2003) A National Study of Prison Suicides1999-2000 London: Department of <strong>Health</strong>.19 Borrill J, Maden A, Martin A, Weaver T, Stimson G, Farrell M <strong>and</strong> Barnes T(2001) Differential Substance Misuse Treatment Needs of Women, EthnicMinorities <strong>and</strong> Young <strong>Offender</strong>s in Prison: Prevalence of substance misusetreatment needs London: Home Office.20 Centre for Public Innovation (2005) Court Diversion <strong>and</strong> Liaison Schemes:Recommendations for models of care London: Centre for Public Innovation.21 Department of <strong>Health</strong> (2003) Mainstreaming Gender <strong>and</strong> Women’s Mental<strong>Health</strong>: Implementation Guide London: Department of <strong>Health</strong>.22 Nacro (2005) Findings of the 2004 Survey of Court Diversion/<strong>Criminal</strong>Justice Mental <strong>Health</strong> Liaison Scheme for Mentally Disordered <strong>Offender</strong>s inEngl<strong>and</strong> <strong>and</strong> Wales London: Nacro.23 Nacro (2006) Liaison <strong>and</strong> Diversion Schemes for Mentally Disordered<strong>Offender</strong>s: A mental health good practice guide London: Nacro.24 Birmingham L (2001) ‘Diversion from custody’ Advances in PsychiatricTreatment, 7, pp. 198-207.Do you need this leafletin another format?Ring 020 7840 7220.Nacro’s Mental <strong>Health</strong> UnitNacro believes that responses to offenders withmental health needs should focus on their care <strong>and</strong>treatment rather than on punishment. To help bringabout this change, Nacro campaigns for: more effective working partnerships betweenagencies the development of specialist skills in the criminal<strong>justice</strong> system better information sharing the education <strong>and</strong> training of staff so that theyhave the skills <strong>and</strong> encouragement they need towork with a group who can be difficult <strong>and</strong>unrewarding.Nacro’s Mental <strong>Health</strong> Unit has been working to tackleproblems faced by offenders with mental healthneeds since 1990. We work with government agenciesat a national <strong>and</strong> local level to develop more effectiveways to deal with offenders with mental health needs.We provide a range of services: information <strong>and</strong>advice; policy development <strong>and</strong> other consultancyservices; <strong>and</strong> training. We also run a major annualconference on mental health <strong>and</strong> crime.Nacro has a specialist mental health websitewhich offers information <strong>and</strong> support for practitioners<strong>and</strong> policy makers working in the field of criminal<strong>justice</strong> <strong>and</strong> mental health. To find out more, visit thewebsite or contact the Mental <strong>Health</strong> Unit on 020 78401209 or email mentalhealth@nacro.org.uk.www.nacromentalhealth.org.ukICPRThe Institute for <strong>Criminal</strong> Policy Research (ICPR)carries out multi-disciplinary research into crime <strong>and</strong>the criminal <strong>justice</strong> system. We produce work whichis independent <strong>and</strong> objective. Our key audiences aremanagers <strong>and</strong> practitioners within the criminal <strong>justice</strong>system, other professionals working with offenders,<strong>and</strong> politicians <strong>and</strong> their advisors. Our researchapproaches incorporate both quantitative <strong>and</strong>qualitative methods. Our main areas of researchinclude:the quality <strong>and</strong> effectiveness of public services<strong>and</strong> resources (including police, probation <strong>and</strong>services for offenders <strong>and</strong> drug users)the causes, consequences <strong>and</strong> prevention ofoffendingpublic attitudes towards crime <strong>and</strong> sentencing,the police <strong>and</strong> community safety.www.umds.ac.uk/schools/law/research/icpr/12